
Abstract
External auditory canal cancer is a rare disease which can be treated by surgery or chemoradiation. The most common histological type is squamous cell carcinoma, but rare types such as adenocarcinoma have been reported and are thought to be derived from the ceruminous glands. Here, we present a case of ceruminous adenocarcinoma, not otherwise specified (NOS) in the external auditory canal. A 72-year-old woman was referred to our department with discomfort due to a mass in the external ear canal. No typical symptoms of malignancy, such as pain or bleeding, were noted at the initial examination. The patient underwent a total excision under local anesthesia as a diagnostic treatment. She was diagnosed with ceruminous adenocarcinoma, NOS based on the results of immunostaining of the excised specimen, and is currently being followed up as an outpatient. Adenocarcinoma is thought to originate from the cerumen glands of the ear canal and the lack of specific symptoms may make it difficult to differentiate it from benign tumors. Although adenocarcinoma, NOS has been reported in the head and neck region, there have been no reported cases occurring in the external ear canal, and to the best of our knowledge, this is the first report.
Keywords
Introduction
External ear canal cancer accounts for about 1% of all head and neck cancers and can be treated with various options such as surgery and chemoradiation but the prognosis of advanced cases is very poor. The majority of the cancers are histologically classified as squamous cell carcinomas, although adenoid cystic carcinoma and adenocarcinoma have been reported as rare histologic types. Among them, adenocarcinoma of the ear canal is thought to originate from the apocrine sweat glands of the cartilaginous skin of the ear canal and is often detected after the tumor has progressed because it does not have any characteristic clinical signs. Here, we report the first case of a ceruminous adenocarcinoma, not otherwise specified (NOS) type, occurring in the external auditory canal.
Case Report
A 72-year-old woman with no previous history of surgery was referred to our department because of discomfort in her left ear for about 2 months. The general practitioner had noted a mass in the external auditory canal which was treated with topical steroids with no apparent improvement. She complained of ear discomfort but no obvious pain, hearing loss, or dizziness. Physical examination revealed a smooth, superficial red mass arising from the inferior wall at the entrance of the right external auditory canal (Figure 1A). Suspecting an external auditory canal hemangioma or granuloma, the patient was admitted to the hospital for excision under local anesthesia. The mass was about 10 mm in length and slightly broad-based but was confined to the cartilage of the external auditory canal. We excised it using an electrocautery with a safety zone of approximately 3 mm placed around the perimeter, and the surgery was completed as an open wound without suturing. She was discharged the day after surgery with good postoperative progress and was followed up regularly by outpatient consultations. Epithelialization was completed at approximately 5 weeks postoperatively and good progress was observed (Figure 1B).
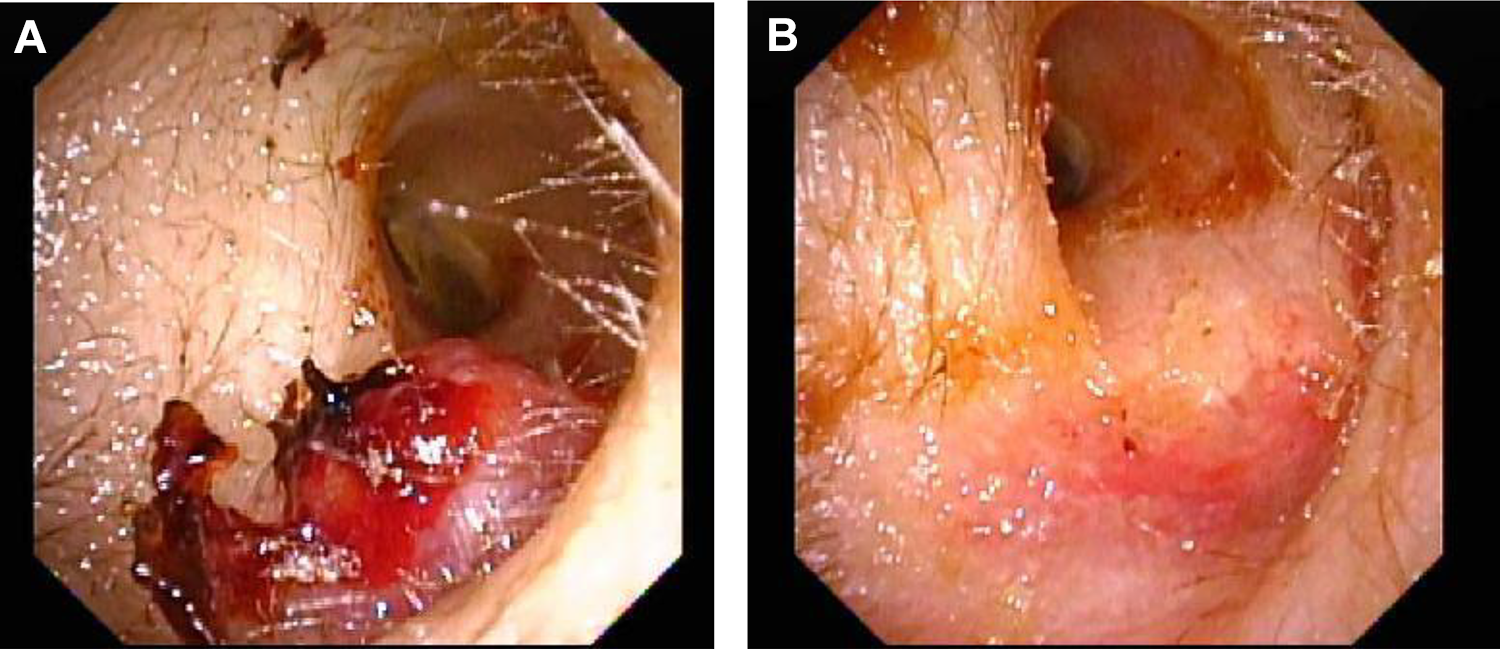
A red, smooth, superficial mass at the entrance to the external auditory canal was detected. Tumor stems were broad-based (A). The external auditory canal at 5 weeks postoperatively after removal of the mass. Good epithelialization of the wound can be observed. There was no evidence of suspicious tumor remnants (B).
Hematoxylin eosin staining of the excised specimen showed subepithelial infiltration of atypical cells with pale acidophilic cytoplasm and oval swollen nuclei (Figure 2A). Immunostaining revealed CK5/6(-), p63(-), p40(-), SMA (-), S100(-), c-kit (-), GATA-3(-), and HER2(+). After considering these findings and the site of occurrence, we diagnosed ceruminous adenocarcinoma, NOS (Figure 2B). Cervical contrast-enhanced computed tomography performed for the purpose of searching for potential metastases demonstrated no obvious metastases and no findings of suspected mass remnants.
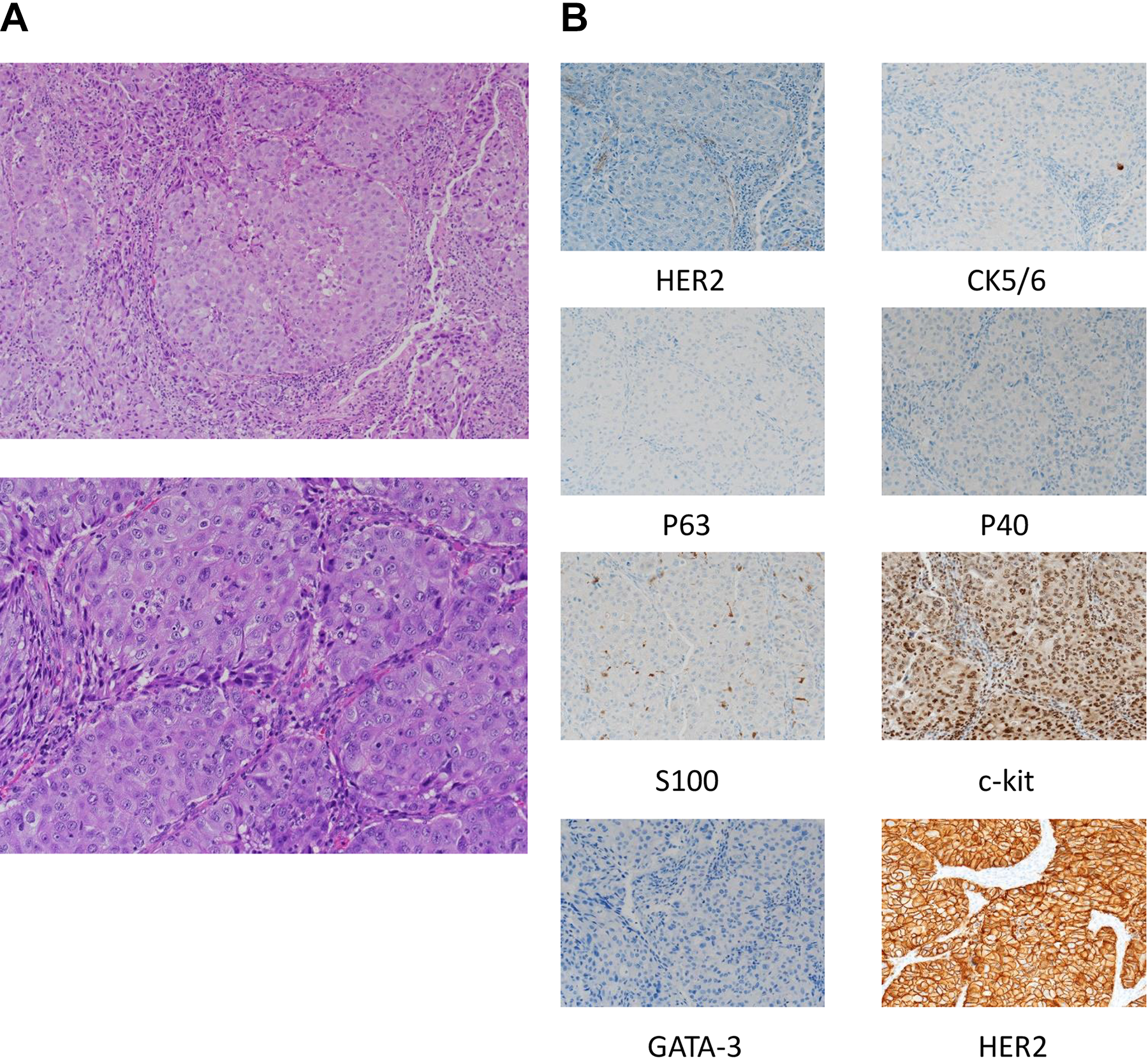
Hematoxylin eosin (HE) staining shows subepithelial infiltration of atypical cells with pale acidophilic cytoplasm and oval swollen nuclei (A). CK5/6(-), p63(-), p40(-), SMA(-), S100(-), c-kit(-), GATA-3(-), and HER2(+) cell infiltration is evident (B).
Discussion
External ear cancers are rare among head and neck cancers, accounting for about 1% of all head and neck cancers. The formation of a bleeding mass in the ear canal may cause associated pain and hearing impairment, and dizziness may also occur as the disease progresses. Surgery, radiation therapy, and chemotherapy (including arterial injections) can be used to treat the disease, but the prognosis is poor in patients with advanced cancer and Moody et al reported 2-year survival rates of 50% for T3 and 7% for T4 cancer in 2000. 1 Histologically, the majority of the cancers are squamous cell carcinomas, followed by adenoid cystic carcinomas. Adenocarcinomas have been reported to be very rare, and they are thought to arise from the sweat gland tissue that lies just beneath the skin of the ear canal. Tumors derived from the cerumen gland were classified in 1972 based on the pathological findings into 4 types; ceruminous adenomas, ceruminous adenocarcinomas, adenoid cystic carcinomas, and pleomorphic adenomas. 2 No unique symptoms of ceruminous adenocarcinomas have been reported and they are often diagnosed in the advanced stage. 3
Six pathological features have been reported in the past: (1) a strong tendency for cellular infiltration, (2) strong perineural infiltration, (3) eosinophilic cytoplasm, (4) irregular glandularity, (5) protruding nucleoli, and (6) increase in fission images and abnormal fission images. 4 In this patient, there were no symptoms such as easy bleeding or pain, and the tumor was smooth showing no obvious tendency for rapid growth. Therefore, we suspected a benign tumor and decided to perform surgery. Although pathology of the excised specimen did not clearly confirm perineural infiltration, the other findings were consistent with ceruminous adenocarcinoma. However, the characteristic pathological features described above are not always present in all cases. Consequently, this case was considered a valuable case because 5 of the 6 findings could be identified.
Adenocarcinoma with obvious glandular differentiation but not in any other category is specifically defined as adenocarcinoma, NOS. In the head and neck region, cases have been reported in the salivary glands, maxillary sinuses, tongue, and larynx.5-8 Although cases of adenocarcinoma of the external auditory canal have been reported, as far as we are aware, this is the first case of NOS type of ceruminous adenocarcinoma.
Ceruminous adenocarcinoma is associated with a high incidence of metastasis to the brain, lungs, and bone, and a lower incidence of metastasis to the cervical lymph nodes.9-11 Treatment is based on a single lumpectomy, but if involvement of the middle ear is observed, a temporal bone resection is recommended. Radiotherapy is often used for palliative purposes such as pain relief and control of recurrent lesions, but is rarely chosen as the first treatment. 3 However, in some cases where radical surgery is not feasible or there are distant metastases, a combination of surgery and radiotherapy has been reported to improve the prognosis and quality of life. 12 In our patient, the tumor was resected with a safe zone around it and there was no tumor invasion at the margins. Additionally, it was confirmed that there were no metastatic lesions. Hence, the patient is being carefully followed up on an outpatient basis without additional treatment.
In conclusion, we experienced a case of ceruminous adenocarcinoma, NOS, arising in the external ear canal. To the best of our knowledge, this is the first report of a NOS type adenocarcinoma of cerumen gland origin. Ceruminous-adenocarcinoma may be difficult to distinguish from benign diseases based on symptoms and local findings, and should be kept in mind when diagnosing and treating external auditory canal masses.
Footnotes
Authors’ Note
Written informed consent was obtained from the patient for patient information and images to be published in this article. K.W. contributed to concept, T.T. contributed to design and H.N contributed to supervision, K.W. contributed to materials, and Y.H. and K.M. contributed to analysis and interpretation.
Acknowledgments
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.