
Abstract
A 32-year-old female with a history of bipolar disorder and schizophrenia was transported to our tertiary-care hospital after swallowing a large toilet paper holder bracket. Removal of the large foreign body required coordination between anesthesiology, otolaryngology, and trauma surgery. A tracheostomy airway was established, and the object was removed transorally. The object was found to be a toilet paper holder bracket measuring 7.5 cm × 5.4 cm × 5.4 cm with a 2.6 cm screw protruding from the end. A review of articles describing the removal of foreign bodies from the upper aerodigestive tract found our object to be the largest foreign body ingestion described in literature. One report suggested that 18% of adult patients with foreign body ingestions had primary neuropsychiatric disorders. Our patient’s psychiatric disorder was a major underlying factor leading to the ingestion, with our patient reporting hallucinations instructing her to ingest household objects.
Introduction
Foreign body ingestion remains an important cause of mortality in the United States with as many as 1500 fatalities per year. 1 Although it is much more common in the pediatric population, it often presents in adults secondary to psychiatric disorders, alcohol consumption, or edentulous states. 2 Many studies have described removal of ingested coins, batteries, magnets, and other foreign bodies from the upper aerodigestive tract. 3 The Mütter Museum in Philadelphia displays a collection of 2374 swallowed objects removed by Chevalier Jackson, MD, in their Jackson Collection; however, most objects removed from the upper aerodigestive tract measure under 4 centimeters (cm). 3 Here, we present the extraction of a foreign body measuring 7.5 cm × 5.4 cm × 5.4 cm with an attached 2.6 cm screw from a patient with a history of bipolar disorder. This study was exempt by the Cooper Health System Institutional Review Board.
Case Report
A 32-year-old female with a history of bipolar I disorder, schizophrenia, multiple suicide attempts, and previous episodes of foreign body ingestion presented to our hospital via Emergency Medical Services after ingesting a toilet paper holder bracket with an attached screw. She arrived alert but with frequent gagging that made it difficult for her to phonate. Although she was able to oxygenate well without assistance, she was tachycardic and hypertensive. The neck X-ray revealed a 7.5 cm × 5.4 cm × 5.4 cm object with a 2.6 cm protrusion pointing superiorly in the upper aerodigestive tract (Figure 1). On initial evaluation, there was no evidence of subcutaneous emphysema, pneumomediastinum, or pneumoperitoneum. The patient was emergently brought to the operating room in an upright position.
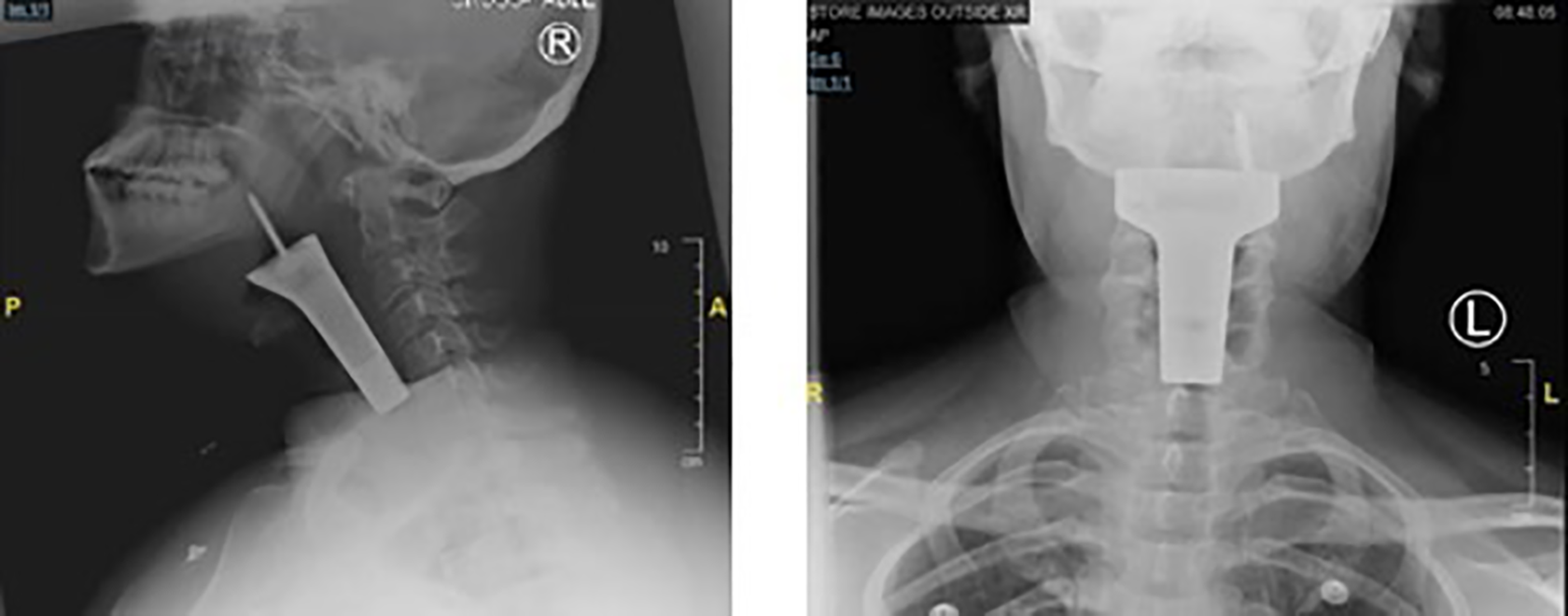
X-rays showing the radiopaque foreign body in the upper aerodigestive tract.
Both nasotracheal and orotracheal attempts at fiberoptic intubation were unsuccessful. Direct examination of the oral cavity and oropharynx revealed a screw pointing superiorly into the left lateral oropharyngeal wall. It was consistent with the foreign body visualized on X-ray. The screw was grasped with a sponge stick to prevent downward displacement of the object, and transoral removal was attempted, but not unsuccessful. At this point, the patient’s oxygen saturation began to drop and her respiratory status began to decline, so we decided to perform an emergent tracheostomy under local anesthesia. Lidocaine was administered in a field block manner and a size 6 Shiley tracheostomy tube (Medtronic-Dublin) was inserted between second and third tracheal rings. The patient was then connected to the ventilator and placed in a supine position with the neck extended. Next, direct laryngoscopy was attempted with a Macintosh laryngoscope, but collapsing soft tissue obscured visualization of the bracket. A Dedo laryngoscope was then inserted and the larynx was visualized. At this point, removal of the foreign body was once again attempted, but it was unsuccessful as the object was caught superiorly by the soft palate and inferiorly by hypopharyngeal tissue. A hemostat was clamped onto the rim of the object to provide additional leverage, and another hemostat was used to gently retract the soft palate superiorly to remove obstruction of the foreign body. This last maneuver cleared the way, and with alternating gentle pulling on the 2 sides of the metal object, the foreign body was fully extracted. Upon removal, the foreign body was visualized to be a bracket for a toilet paper holder with the screw still attached (Figure 2).
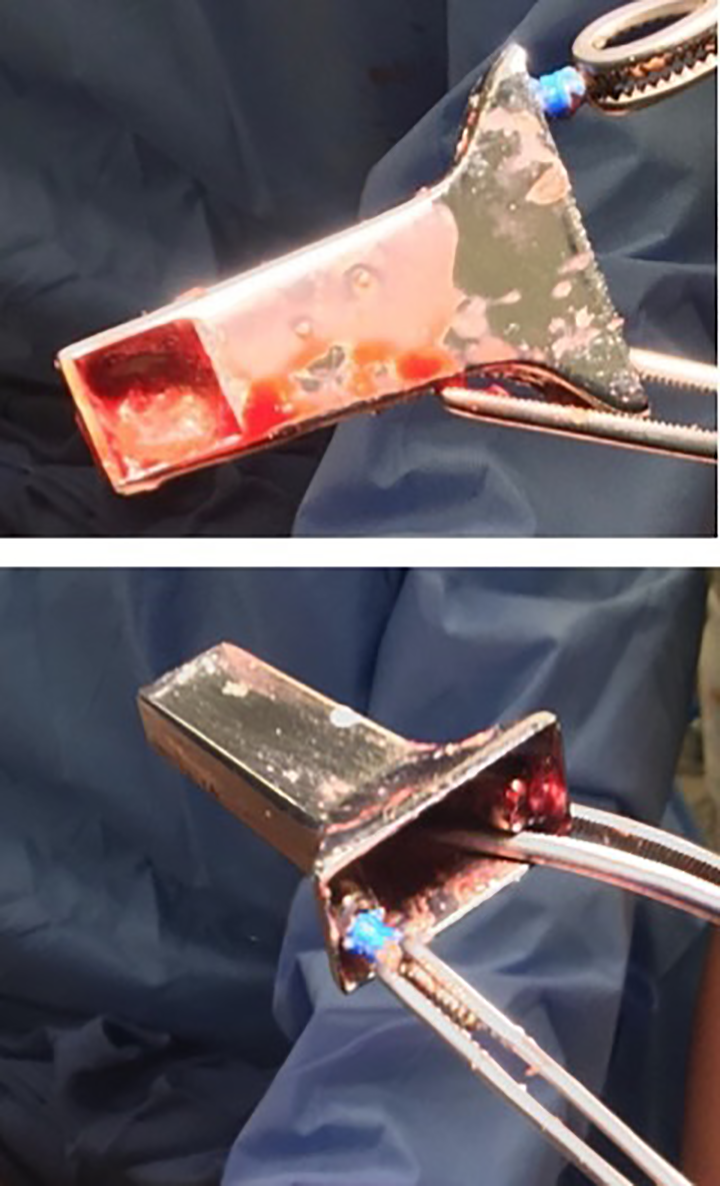
Foreign body after removal.
Following removal, direct laryngoscopy with a Dedo laryngoscope was once again performed. The laryngeal ventricles, arytenoids, postcricoid space, and vocal cords were noted to be normal. There were no obvious lacerations or sites of active bleeding, besides a minor ooze from the mucosa. After removal of the laryngoscope, the patient remained sedated and was transferred to the postanesthesia care unit in stable condition.
Just one day after discharge from our hospital to a nearby inpatient psychiatric center, our patient ingested a toothbrush and returned for an emergent removal from her stomach. Since the second admission, our patient has not returned for further medical assistance.
Discussion
This case demonstrates a challenging scenario in which an impressively large and potentially damaging foreign body required urgent removal from the upper aerodigestive tract and required an awake tracheostomy for airway management. Literature review reveals that although ingestion of a foreign object is not a rare event, few ingested objects are as large as the one in this case. 3 The 7.5 cm × 5.4 cm × 5.4 cm dimensions of this toilet paper holder bracket with a 2.6 cm screw attached represents the largest ingested foreign body in scientific literature. The object in this case posed great potential for harm due to its size and sharp nature, and effective coordination of otolaryngology and anesthesiology teams allowed for removal of the object with minimal harm to the patient.
Objects lodged in the upper aerodigestive tract have the potential to cause a variety of problems. Potential complications include airway compromise, infection, abscess formation, arterial aneurysm, carotid artery rupture, and vocal cord paralysis. A study of 60 cases of upper aerodigestive foreign body extractions found that acute complications from foreign body extractions are relatively uncommon, occurring in just 3 of the studied cases. 4 In another study of 327 patients with upper airway foreign body impaction, the most common complication among patients older than 10 years is the formation of retropharyngeal abscesses. Pulmonary complications such as aspiration, pneumonia, pneumonitis, and pulmonary collapse are second most common, and other reported complications include local infection and perforation. 5
In this report, the patient’s psychiatric illness was a major underlying factor leading to her presentation. Foreign body ingestion in adults is commonly attributed to psychiatric illness or neurocognitive disability. The previously mentioned review found that 18% of adult patients with foreign body ingestion had primary neurologic disorders including seizures, brain tumors, Parkinson disease, intellectual disability, and cerebral palsy. 4 Our patient, who was previously diagnosed with bipolar disorder and schizophrenia, experienced demand hallucinations instructing her to ingest household objects.
Conclusion
In psychiatric patients with the tendency to ingest foreign bodies, careful psychiatric management is essential to prevent future morbidity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.