
Abstract
Objective:
To develop and validate a clinical score to predict the risk of tympanosclerosis before surgery.
Methods:
A sample of 404 patients who underwent middle ear microsurgery for otitis media was enrolled. These patients were randomly divided into 2 cohorts: the training cohort (n = 243, 60%) and the validation cohort (n = 161, 40%). The preoperative predictors of tympanosclerosis were determined by multivariate logistic regression analysis and implemented using a clinical score tool. The predictive accuracy and discriminative ability of the clinical score were determined by the area under the curve (AUC) and the calibration curve.
Results:
The multivariate analysis in the training cohort (n = 243, 60%) identified independent factors for tympanosclerosis as the female sex (odds ratio [OR]: 3.83; 95% CI: 1.66-9.37), the frequency-specific air-bone gap at 250 Hz ≥ 45 dB HL (OR: 3.68; 95% CI: 1.68-8.57), aditus ad antrum blockage (OR: 3.29; 95% CI: 1.38-8.43), type I eardrum calcification (OR: 25.37; 95% CI: 8.41-88.91) or type II eardrum calcification (OR: 18.86; 95% CI: 6.89-58.77), and a history of otitis media ≥ 10 years (OR: 4.10; 95% CI: 1.58-11.83), which were all included in the clinical score tool. The AUC of the clinical score for predicting tympanosclerosis was 0.89 (95% CI: 0.85-0.93) in the training cohort and 0.89 (95% CI: 0.84-0.95) in the validation cohort. The calibration curve also showed good agreement between the predicted and observed probability.
Conclusions:
The clinical score achieved an optimal prediction of tympanosclerosis before surgery. The presence of calcification pearls on the promontorium tympani is a strong predictor of tympanosclerosis with stapes fixation.
Introduction
Tympanosclerosis is a common sequela of recurrent chronic middle ear infection. The incidence of tympanosclerosis in chronic otitis media ranged from 19% to 32% in previous reports.1,2 It is characterized by progressive hyaline degeneration and accumulation of calcified deposits within the tympanic membrane and the submucosa of the middle ear cavity.3-5 Although the etiopathogenesis of tympanosclerosis has not been fully elucidated, it is widely accepted that it is irreversible. 6 Hence, surgery is by far the most helpful procedure to restore hearing.7,8
However, for patients with tympanosclerosis, surgery should be performed with caution, because in many cases it is much more complicated than for patients without tympanosclerosis. 9 The calcified plaques which alter the compliance of the tympanic membrane and limit the mobility of the ossicles, need to be removed during the surgery.10,11 Therefore, the perforation of the tympanic membrane would become larger, which increased the difficulty of healing. Additionally, the removal of calcified plaques involving the stapes has long been considered formidable and high risk. 12 Serious complications such as floating footplate, labyrinthitis, and facial nerve injury are difficult to avoid without thorough preoperative evaluation and meticulous operative technique. 13
For otologists, encountering tympanosclerosis that was unsuspected preoperatively might present a greater surgical challenge than he or she anticipated, which increases the risk of surgery, especially for young doctors with less experience. 14 Most of patients with tympanosclerosis would gradually lose their hearing again due to the adhesion of the scar in the tympanic cavity after the operation. The patients with these conditions might complain about achieving a hearing result that is less satisfactory than what was indicated before surgery.5,7 Therefore, an accurate diagnosis before surgery is very important.
However, to our knowledge, a suitable preoperative diagnostic tool for tympanosclerosis is currently unavailable. Tympanic membrane calcification might be a good indicator, but there are exceptions, such as myringosclerosis. 15 Patients with myringosclerosis also have calcification on the eardrum, but it does not affect the ossicular chain and mucosa of the middle ear. Therefore, otoscopy examination is insufficient for us to distinguish between tympanosclerosis and myringosclerosis. 16 We also did not find any study suggesting specific computed tomography (CT) imaging signs of tympanosclerosis. Senior surgeons could identify patients with tympanosclerosis based on their own experience, however it is subjective and difficult to replicate and promote. This gives us the motivation to establish the prediction model. The aim of our study was to develop and validate a simple clinical score for predicting tympanosclerosis that would assist comprehensive surgery planning and better preoperative counseling.
Materials and Methods
Patients and Study Design
A retrospective study was conducted among patients who had been diagnosed with otitis media and underwent middle ear microsurgery between November 26, 2016, and January 18, 2020, at the Sir Run Shaw Hospital (Hangzhou, China). The exclusion criteria were revision surgery, cholesteatoma, middle ear tumor, or congenital malformation of the ear. All patients were evaluated by taking a proper history and performing routine preoperative examinations, including rigid otoscopy, pure tone audiometry, and CT of the temporal bone. A total of 60% of patients meeting the study criteria were randomly divided into the training cohort, while the remaining 40% were divided into the validation cohort.
The study was approved by the Institutional Ethics Committee of the Sir Run Shaw Hospital. Informed consent was obtained from all patients for their data to be used for research. Patients did not receive financial compensation.
Definitive Diagnostic Criteria of Tympanosclerosis
The definitive diagnostic criteria for tympanosclerosis are based on the exploration during surgery and postoperative pathology. Whitish, chalk-like plaques are present in the tympanum or on the medial side of the tympanic membrane. The ossicular chain is involved with the plaques, and its mobility is somewhat limited or even absent. The findings on hematoxylin and eosin staining of pathological sections include fibroblast proliferation, uniform collagen fibers, and the accumulation of hyaline collagen surrounding the fibroblasts. The collagen fibers of the connective tissue appear irregular, thick, and tightly set, leading to the appearance of an osseous-like matrix.17-19
All of the patients diagnosed with tympanosclerosis were classified into 4 types based on the location of tympanosclerosis according to the classification system proposed by Wieling and Kerr. 20
Type I: The lesion affects the tympanic membrane and sometimes involves the malleus.
Type II: The lesion fixes the malleus–incus complex while the stapes is mobile.
Type III: The stapes fixed or absent while the malleus–incus complex is mobile if present.
Type IV: The ossicular chain is completely fixed.
Candidate Variables
Ear discharge
Dry ear was defined as no history of otorrhea during the past 3 months before surgery.
Area of eardrum perforation
The eardrum was anatomically separated into 4 quadrants for clarity. Each quadrant accounted for 25% of the total perforated area. The perforated area in all quadrants was added to obtain the total perforated area as a percentage.
The type of perforation was also categorized as central or marginal perforation. A central perforation did not involve the edge of the eardrum (the annulus), whereas a marginal perforation did involve the edge of the eardrum. If the tympanic perforation type was central, the total percentage of the perforated area was halved.
Eardrum calcification location
None: No eardrum calcification is observed.
Type I: Calcification affects both the anterior–superior and posterior–superior quadrants of the tympanic membrane or more quadrants.
Type II: Calcification affects only the anterior–superior or posterior–superior quadrant of the tympanic membrane and/or another quadrant.
Air-bone gap
The frequency-specific air-bone gap (ABG) was obtained by measuring each ABG on pure tone audiometry at a frequency of 250, 500, 1, 2, and 4 kHz. The mean ABG was the average value of the ABGs at all of the above frequencies.
Aditus ad antrum blockage
Aditus ad antrum blockage was determined by detecting the soft tissue density in the aditus ad antrum on temporal bone CT before surgery.
Tympanum calcification pearls
Tympanum calcification pearls were indicated by white pearl-like beads observed scattered or in bunches on the promontorium tympani (Figure 1).
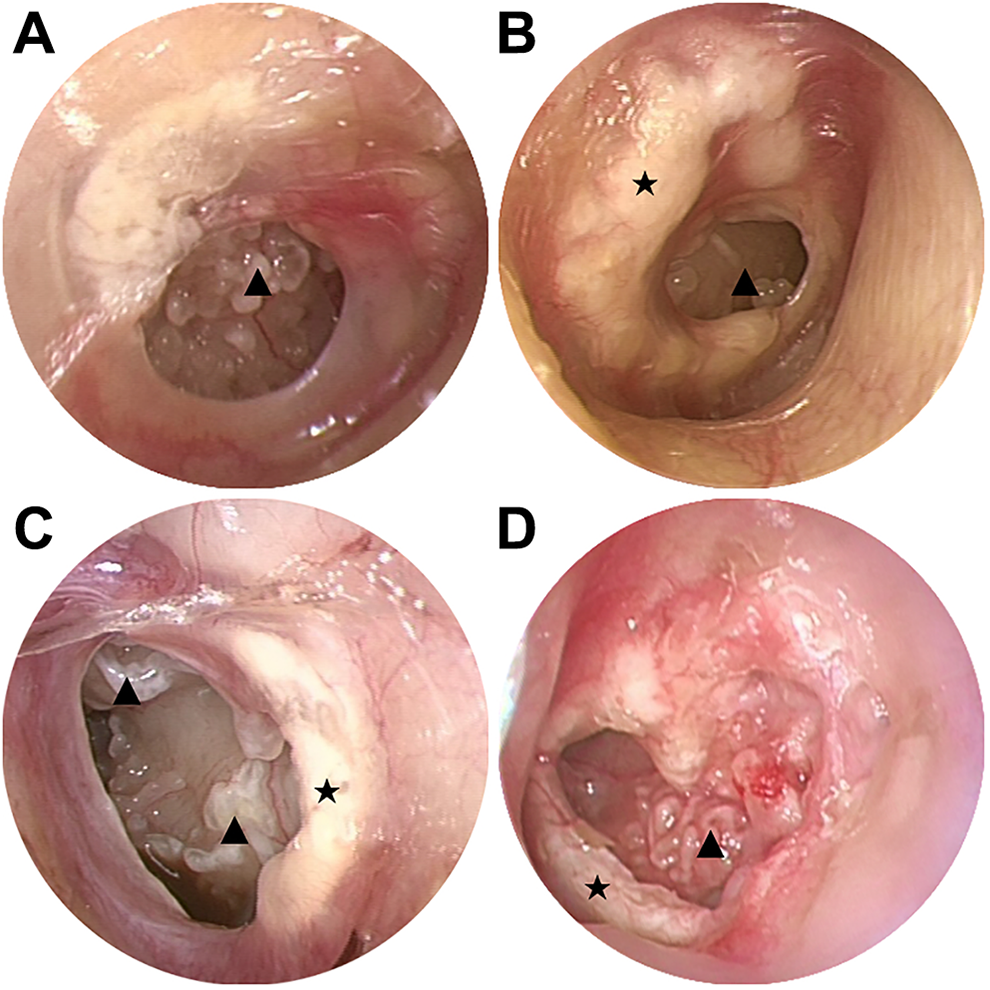
Characteristics of tympanosclerosis under rigid otoscopy. ▴ Tympanic calcification pearls: white pearl-like beads scattered or in bunches on the promontorium tympani. ★ Large, thick calcified patches on the eardrum.
Other variables
The patient age, sex, history of otitis media, and serum calcium were also recorded for analysis.
Statistical Analysis
All of the continuous variables were discretized into categorical variables to ensure that the model would be easy to use and interpret. The cutoff value for each continuous variable was determined by maximizing the Youden index (ie, sensitivity + specificity − 1). All variables are expressed as frequencies and percentages and were compared by chi-square test or Fisher exact test. The significance of each candidate variable was assessed by univariate logistic regression analysis to investigate the independent risk factors for tympanosclerosis. All variables associated with tympanosclerosis at a significant level were candidates for the multivariate logistic regression model.
Variables were carefully selected for inclusion. The number of predictor variables was limited by the number of positive events available to avoid overfitting of the model; the limit was approximately 1 in 15 to 20. The clinical relevance and ease of acquisition of variables were also considered.
A simplified clinical score tool for the multivariate logistic regression model was constructed by dividing the coefficient for each item by the lowest coefficient; these data were then converted to whole numbers as scores for each predictor variable. 21
Internal validity was tested using the validation cohort. The performance of the model was quantified by means of discrimination and calibration. Discrimination was quantified by the area under the curve (AUC) with the Delong method to compute the CI. A 2000-sample bootstrap test was used to compare the receiver operating characteristic (ROC) curves between the multivariate logistic regression model and the clinical score tool. All tests were 2-sided, and .05 was set as the P value to indicate statistical significance. Statistical analysis was performed using R programming language, version R 3.6.2.
Results
Patient Characteristics
Of 545 consecutive patients who underwent middle ear microsurgery, 404 met the criteria and were enrolled in this study. In 99 patients, chronic otitis media was complicated with tympanosclerosis, for an incidence of tympanosclerosis of 24.5% in our study. Twelve patients presented tympanum calcification pearls on otoscopy before surgery, and all of these patients were diagnosed with tympanosclerosis. Eleven of these patients were classified as having type IV tympanosclerosis. Two patients presented the coexistence of tympanosclerosis and cholesteatoma. The clinicopathological characteristics of the patients are listed in Table 1. The baseline data were similar between the training and validation cohorts.
Baseline Clinical Characteristics of the Training and Validation Cohorts.
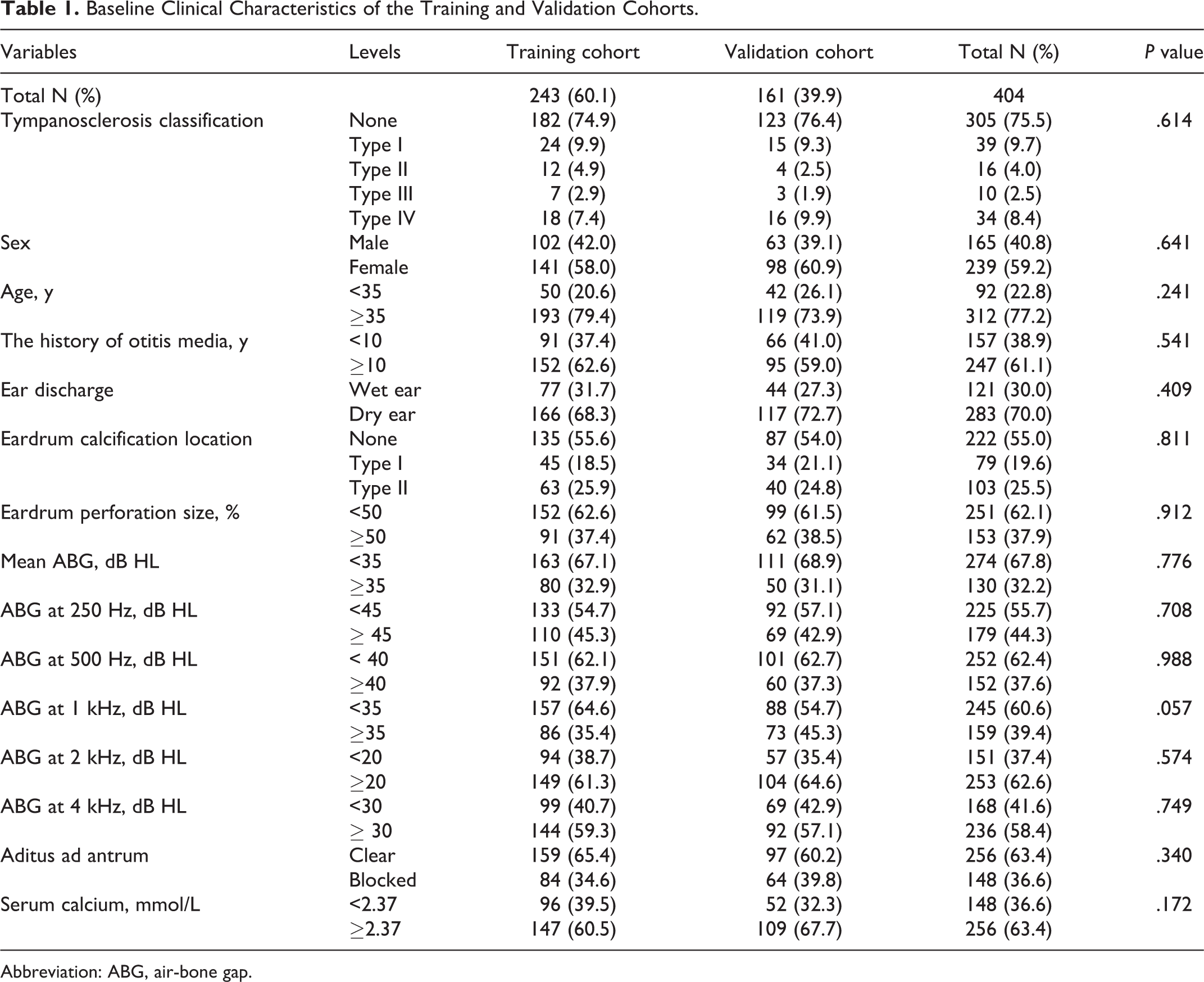
Abbreviation: ABG, air-bone gap.
Model Development
The results of the univariate and multivariate logistic analyses are presented in Table 2. According to the multivariate analysis, female sex (odds ratio [OR]: 3.83; 95% CI: 1.66-9.37), the frequency-specific ABG at 250 Hz ≥45 dB HL (OR, 3.68; 95% CI, 1.68-8.57), aditus ad antrum blockage (OR, 3.29; 95% CI, 1.38-8.43), type I eardrum calcification (OR: 25.37; 95% CI: 8.41-88.91) or type II eardrum calcification (OR: 18.86; 95% CI: 6.89-58.77), and a history of otitis media ≥10 years (OR: 4.10; 95% CI: 1.58-11.83) were independently associated with tympanosclerosis (Table 2).
Results of Univariate and Multivariate Logistic Regression Analyses Based on Data in the Training Cohort.
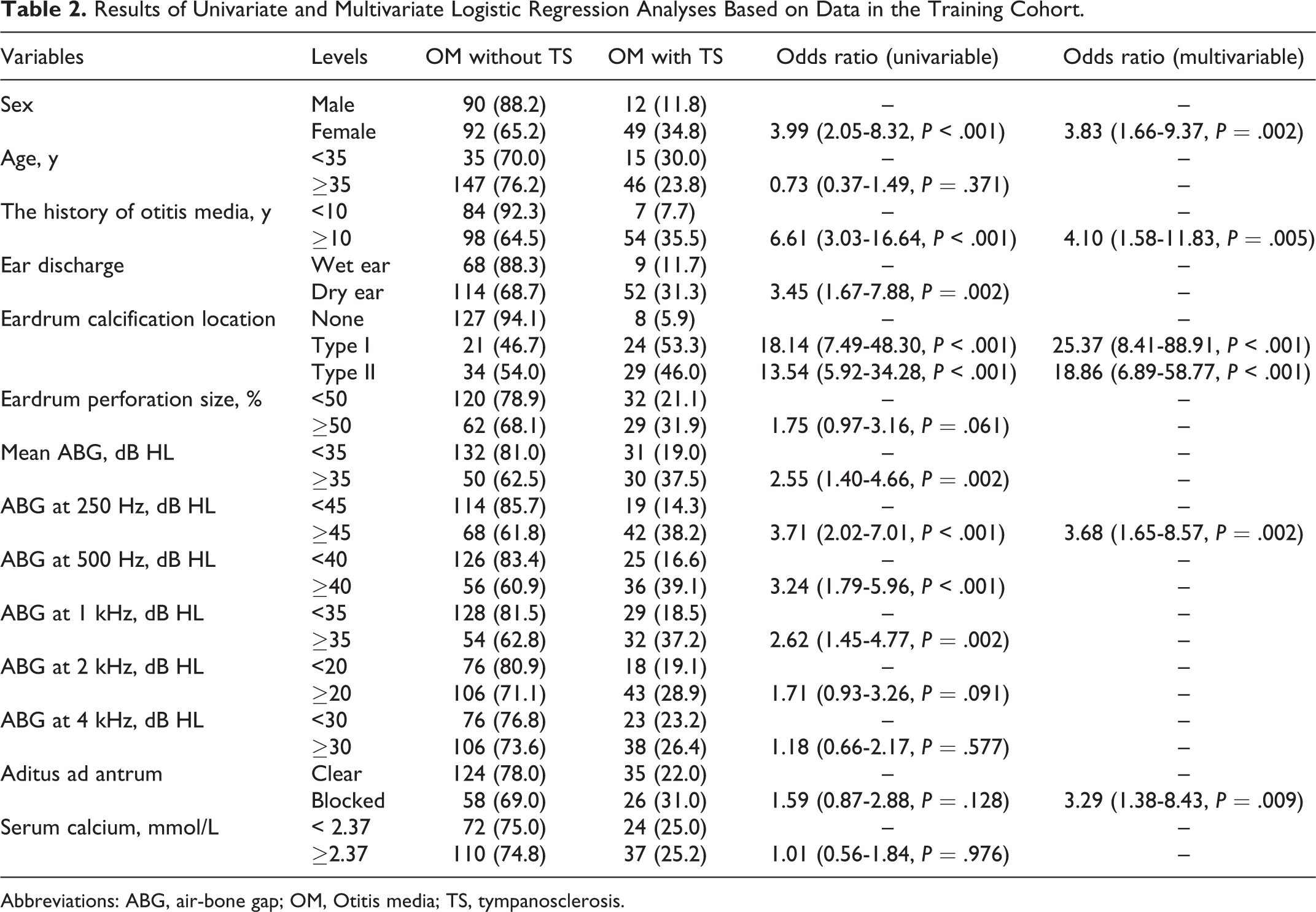
Abbreviations: ABG, air-bone gap; OM, Otitis media; TS, tympanosclerosis.
The clinical score tool based on the multivariate logistic regression model was derived with correlation coefficients (95% CI) and weighted scores present together in Table 3. The corresponding probabilities of complicating tympanosclerosis calculated using the clinical score are shown in Figure 2A.
Score Chart Based on Multivariable Logistic Regression Analysis for Predicting Tympanosclerosis.
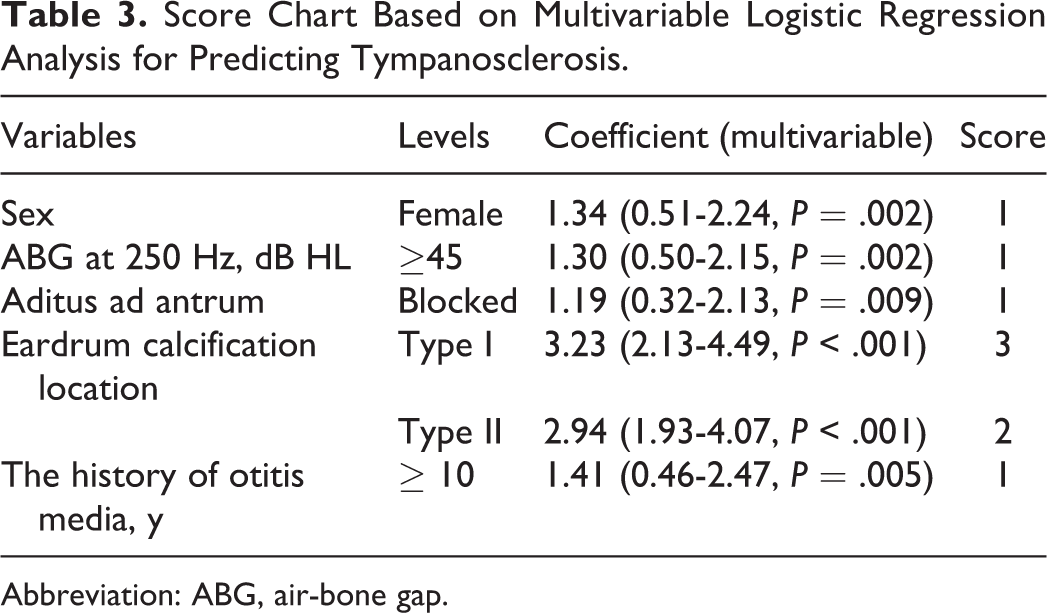
Abbreviation: ABG, air-bone gap.
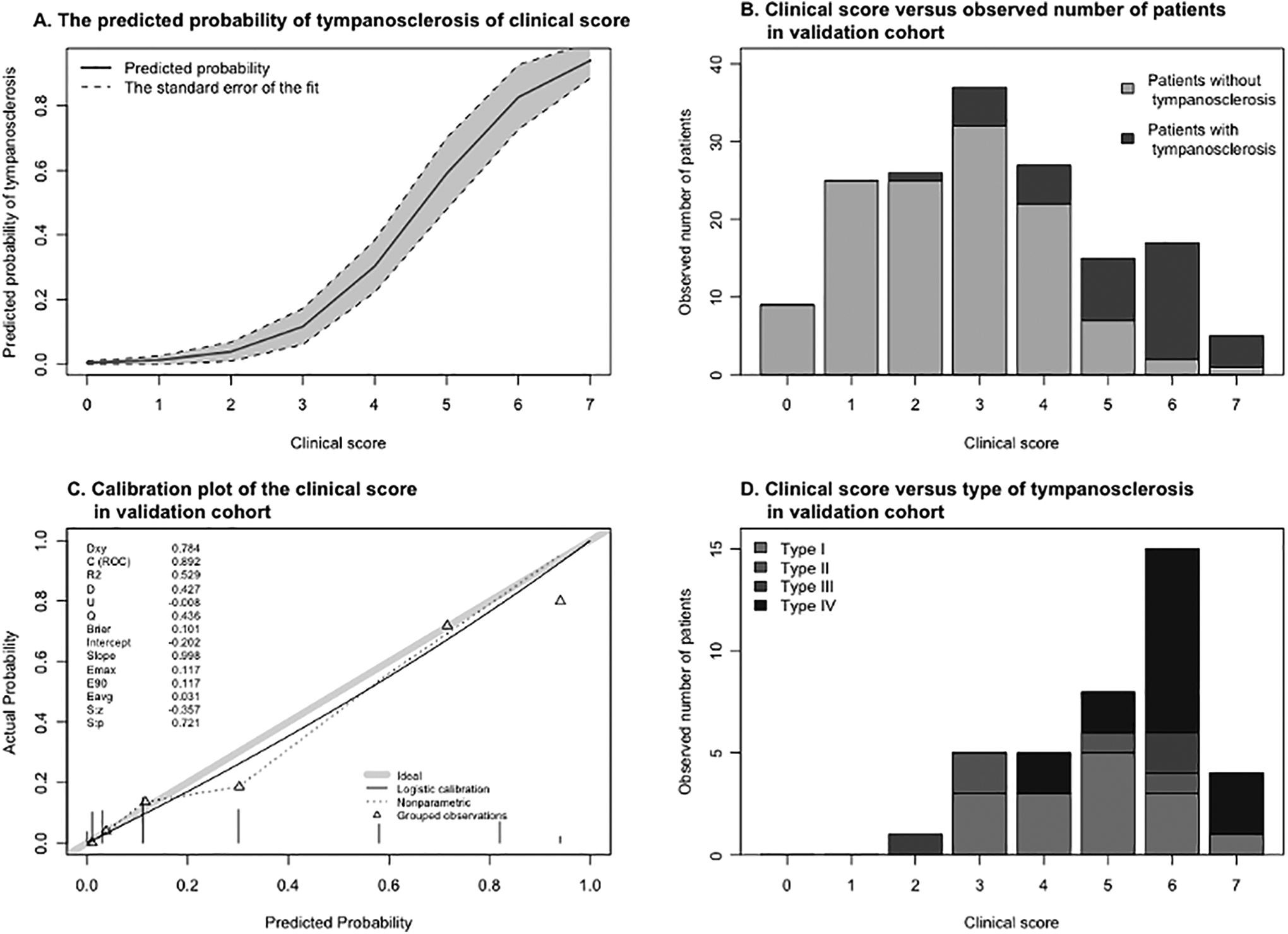
A, The corresponding probabilities of complicating tympanosclerosis of the clinical score. The solid line shows the sum score determined by the clinical score tool compared with the corresponding probabilities of tympanosclerosis. The shaded area is the 95% CI of the corresponding probabilities. B, The observed number of patients with or without tympanosclerosis stratified by the clinical scores in the validation cohort. C, Calibration plot of the clinical score in the validation cohort. The solid line is a smoothed curve that represents an estimate of the relationship between the predicted and observed probabilities of tympanosclerosis. A variety of statistics are displayed on the top left. D. The observed number of patients with different types of tympanosclerosis stratified by the clinical scores in the validation cohort.
Model Accuracy
The AUC of the multivariate logistic regression model was 0.9 (95% CI: 0.85-0.94) in the training cohort and 0.89 (95% CI: 0.84-0.95) in the validation cohort. The AUC of the clinical score tool was 0.89 (95% CI: 0.85-0.93) in the training cohort and 0.89 (95% CI: 0.84-0.95) in the validation cohort. There was no significant difference in the ROC curve between the multivariate logistic regression model and the clinical score tool.
For clinical use of the score tool, we suggest using 4 as the optimum cutoff value. Patients with a clinical score of 4 or more are at a high risk of tympanosclerosis, with a diagnostic sensitivity of 88.52% and specificity of 73.63%. The risk score and type of tympanosclerosis appeared to be positively correlated. As the risk score increased, the likelihood of a high-level type of tympanosclerosis gradually increased (Figure 2D).
The calibration plots graphically showed good agreement between the predicted probabilities and the observed probabilities of the validation cohort (Figure 2C).
Discussion
Tympanosclerosis is a nonspecific result of chronic inflammation in the middle ear, and unless we perform surgical exploration, there is currently a lack of specific diagnostic indicators. Therefore, the clinical score was developed and validated as an effective and easy-to-use scoring instrument to meet the clinical need.
We found that the location of eardrum calcification can reflect the extent to which the ossicular chain is affected. The probability that the ossicular chain is affected by calcification is substantially increased, with an OR of 18.14 (7.49-48.30, P < .001), if calcification is observed on both sides of the malleus handle, which we classified as type I eardrum calcification. Calcification that occurs in other quadrants may have less of an impact on ossicular chain activity. Some of them may be just myringosclerosis, and this type of calcification does not have to be removed during surgery. 9 Although it is time consuming and somewhat difficult to clean up calcification on both sides of the malleolus, in our opinion, it is worthwhile to loosen the ossicular chain and obtain better postoperative hearing improvement. 9
In clinical practice, the mean ABG is used to assess the degree of hearing loss, but we found that patients with chronic otitis media, especially those with tympanosclerosis, have a greater ABG at low frequencies (Figure 3). This finding is very similar to the study by Kikkawa et al, who observed frequency-dependent hearing loss in patients with an immobile ossicular chain, which is more significant at lower frequencies and preserved better at 2000 Hz. 22 Therefore, we used frequency-specific ABGs as candidate variables because they are easy to assess and therefore easy to apply. We found that the variable of frequency-specific ABG at 250 Hz had the highest OR for tympanosclerosis, and we included it in the final model instead of the mean ABG.
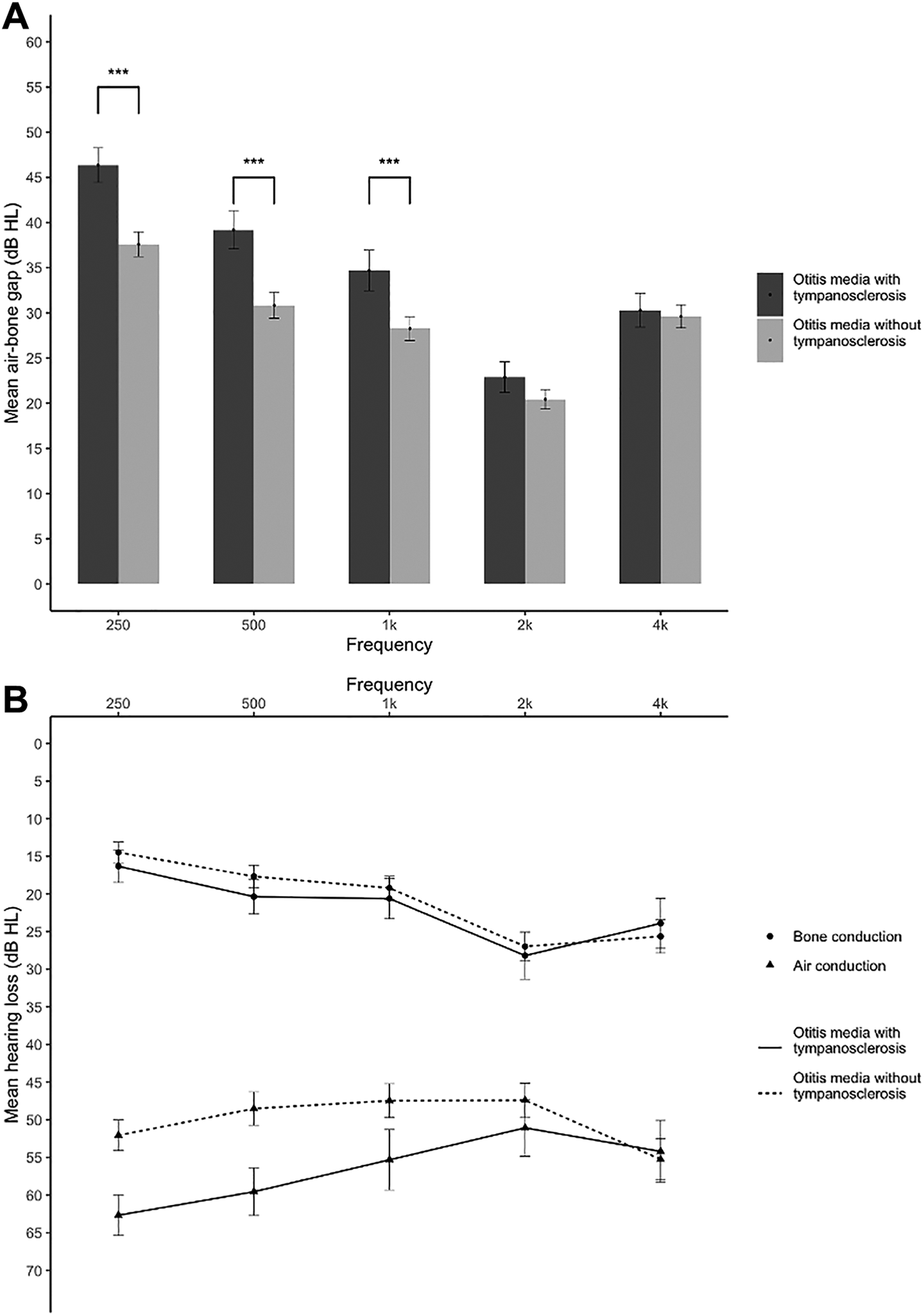
A, Mean frequency-specific ABGs with 95% CIs between otitis media patients with and without tympanosclerosis. ***P < .001. B, Mean pure tone audiometry with 95% CIs between otitis media patients with and without tympanosclerosis. ABG indicates air-bone gap.
In addition, the history of otitis media was found to be a risk factor for tympanosclerosis in our study. Patients with a history of otitis media ≥10 years were more likely to have tympanosclerosis, with an OR of 6.61 (3.03-16.64, P < .001). From this, we can infer that the occurrence of tympanosclerosis is a long-term gradual process. The replacement of loose connective tissue with fibrous connective tissue and subsequent accumulation of calcium deposits in the middle ear is a lengthy process. 18 However, Dinç and Kumbul did not observe a difference in disease duration between patients with or without tympanosclerosis. 1 We postulate that this difference in the findings may be related to the method used to collect the medical history. The history of otitis media we use is from the very time that patients are aware of having otitis media. Meanwhile, the disease duration used by Dinç and Kumbul was determined as the time patients recently experienced symptoms, such as ear discharge and hearing loss. Most patients with tympanosclerosis had experienced dry ears for a long time and did not notice a significant hearing loss until the ossicular chain was affected. Thus, the disease duration with symptoms would be shorter than the history of otitis media, which might explain the differences in the results between our study and the previous report.
Our study found that patients with tympanosclerosis tend to have dry ears. This could be caused by the middle ear mucosa being extensively involved in tympanosclerosis, resulting in suppressed mucus secretion.1,9 The OR of dry ear was 3.45 (1.67-7.88, P = .002) in our univariate regression analysis. However, it was not significant on multivariate regression analysis, possibly because of the correlation between variables.
Aditus ad antrum blockage in preoperative CT images was found to be significantly associated with tympanosclerosis in our study. Kikkawa et al used the pneumatization status of tympanic mastoid cavities as a prognostic indicator in patients with tympanosclerosis and decided whether to perform staged surgery based on these findings. 22 We postulate that the CT value of the shadows around the ossicular chain in patients with tympanosclerosis would be higher than in patients without tympanosclerosis. However, the structure of the ossicular chain is too fine to segment, and we have not yet found a suitable and convenient measurement method for this analysis that can be used in clinical practice to do it. Therefore, we chose aditus ad antrum blockage as our second-best choice.
According to our observations, the presence of calcification pearls on the promontorium tympani is a strong predictor of tympanosclerosis with stapes fixation. Patients with tympanosclerosis presenting with stapes fixation typically have the highest surgical risk and the poorest hearing restoration outcomes.7,23 Most of those patients no longer experience ear discharge, so their motivation for surgery is improving their hearing, which is difficult to achieve. Therefore, the surgeon needs to thoughtfully consider the necessity of surgery and communicate the pros and cons of surgery with the patients. We did not include this variable in our final model because the incidence of tympanic calcification pearls was only 2.97% in our study, which means that only a few patients would benefit from this predictive variable. However, tympanic calcification pearls still should be considered seriously when they appear.
The clinical score is the result of balancing the precision and simplification. Although rounding of the coefficients leads to less-accurate predictions than the original model, the advantage is that it is possible to remember such prediction rules by heart and calculate within a few seconds, in contrast to more refined rules. 21 Moreover, our results show that the predictive accuracy of the multivariate logistic regression model was not greatly reduced by use instead of the clinical score.
In general, the higher the type of tympanosclerosis, the wider the range of lesions that are involved, and therefore surgery and the restoration of hearing after surgery are more difficult to achieve. In addition to the value of predicting tympanosclerosis, the risk score appeared to exhibit a positive correlation with the type of tympanosclerosis in the present study; therefore, it is potentially useful as a reference for preoperative evaluations. Furthermore, the relationship between the clinical score and postoperative hearing improvement can be investigated in the future.
There are some limitations to our study. It is possible that our study has sampling bias. Some studies have reported that some patients with tympanosclerosis do not have perforation of the eardrum. We might have encountered similar cases, but none of these patients underwent surgery, and thus they were not enrolled in our study.15,20 Some reports of cases of with coexisting cholesteatoma and tympanosclerosis have also been published.2,6,7 We also treated similar cases in our clinical practice, but the incidence was quite low, and thus we excluded such cases. Our estimate of the perforated eardrum area was imprecise; hence, the effect of the variable might have been weakened. We have only internally validated our model, and external validation in further research is needed.
Conclusion
To the best of our knowledge, we are the first to develop a diagnostic model and introduce several novel variables to predict the individual probability of tympanosclerosis. The female sex (OR: 3.83; 95% CI: 1.66-9.37), the frequency-specific ABG at 250 Hz ≥ 45 dB HL (OR: 3.68; 95% CI: 1.68-8.57), aditus ad antrum blockage (OR: 3.29; 95% CI: 1.38-8.43), type I eardrum calcification (OR: 25.37; 95% CI: 8.41-88.91) or type II eardrum calcification (OR: 18.86; 95% CI: 6.89-58.77), and a history of otitis media ≥10 years (OR: 4.10; 95% CI: 1.58-11.83) were risk factors for otitis media complicated with tympanosclerosis. The appearance of tympanic calcification pearls merits special attention upon observation, and there is a great possibility that the tympanic mucosa is intensively affected by tympanosclerosis. In such cases, the indications for surgery need to be carefully considered.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Medical Health Science and Technology Project of ZhejiangProvincial Health Commission Grant (No.2019336033) and Medical HealthScience and Technology Project of Hangzhou municipal Health Commission (No. OO20190775).