
Abstract
Objective:
The main aim is to discuss the effect of nasal septal deviation on the postoperative hearing results of patients with tympanosclerosis.
Material and Methods:
We analyzed the hearing results of patients with tympanosclerosis who were operated on in a tertiary center. Pure tone audiometric results were compared according to the existence of nasal septal deviation.
Results:
This study included 48 patients with unilateral tympanosclerosis disease. Moderate or severe septal deviation had no significant effect on postoperative hearing results.
Conclusion:
The nasal septal deviation as the only pathologic factor in patients with tympanosclerosis did not have a deteriorating effect after surgery.
Introduction
Tympanosclerosis is a progressive disease that infiltrates the middle ear and ossicles, causing hearing loss over time. No treatment apart from surgery is clinically available. Surgery does result in a significant improvement, but hearing results can worsen nonsignificantly in the postoperative long-term. 1
We aim to compare the effect of nasal septal deviation (NSD) on postoperative hearing loss in patients with unilateral tympanosclerosis.
Patients and Methods
We retrospectively analyzed patients with unilateral tympanosclerosis who were operated on between 2010 and 2016 in a tertiary center. This study was approved by the local ethics committee (KOU-GAEK 2018/254) and informed consent was obtained from all patients. Patients were evaluated by 2 otolaryngologists with the existence of NSD and by the localization and angle of the NSD.
Preoperative computed tomography (CT) images were evaluated. All nasal pathologies were noted. Evaluation was undertaken using multislice CT (Aquilion 64; Toshiba, Japan) in a supine position.
The measurement of the images was performed with a Sectra Workstation IDS 7 (V18.2.22.4113,2017; Sectra AB, Linköping, Sweden). The coronal CT was evaluated to measure the angle of the NSD as the angle formed by the intersection of a line running from the nasal septal insertion in the maxillary crest to the superior insertion at the crista galli with a line running from the apex of the septal deviation to the superior insertion at the crista galli (Figure 1).
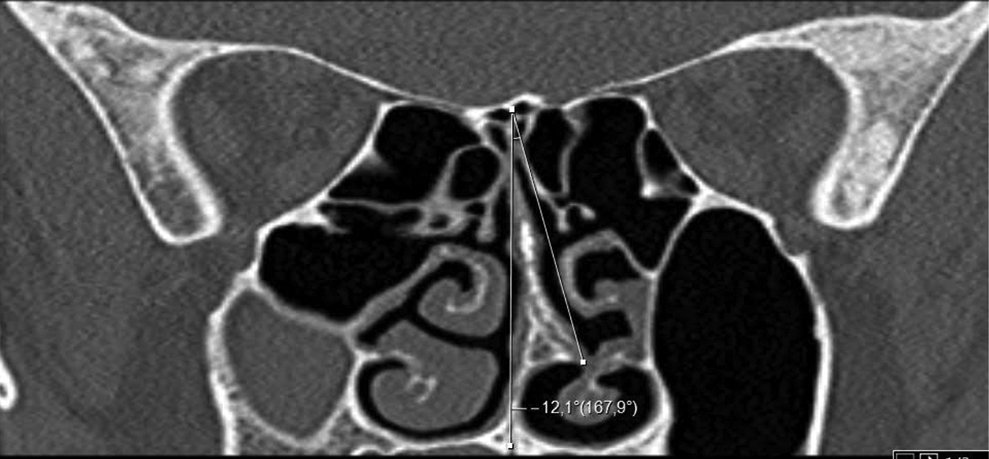
Measurement of nasal septal deviation angle.
Audiometric evaluations were undertaken according to the International Organization for Standardization standards at a maximum of 1 month before surgery and during the last visit after surgery (6-98 months). All groups were compared, first by hearing thresholds and then by success. For success, the criteria of the Otological Society of Japan defined in 2000 were considered. If one of the following criteria was achieved, success was mentioned: a postoperative air-bone gap (ABG) of less than 15 dB, a hearing gain of more than 15 dB, or a threshold of postoperative air conduction of less than 30 dB.
All statistical analyses were performed using IBM SPSS for Windows version 20.0 (IBM Corp, Armonk, New York). Kolmogorov-Smirnov tests were used to test the normality of the data distribution. Continuous variables were expressed as median (25th-75th percentiles) and categorical variables were expressed as counts (percentages). Comparisons of non-normally distributed continuous variables between the times were performed using the Wilcoxon t test and the χ2 test. P < .05 was considered statistically significant for significance.
Results
Between 2010 and 2016, 174 patients with any stage of unilateral tympanosclerosis were operated on at a tertiary center. Patients with bilateral disease, patients who had had no CT before the operation, patients with more pathology than NSD in the nasal passage, patients with an NSD angle of less than 9°, and patients who had had no follow-up for more than 6 months were excluded. The remaining 48 patients who had available paranasal CT before the operation were included in this study.
The average age of all patients included in the study was 33.8 ± 13.7 years. There were 34 (71%) female and 14 (29%) male patients with a follow-up period of 31.4 ± 22.3 (6-98) months. The graft take rate was 93.8%.
All sclerotic plaques were found around the tympanic membrane or ossicles. Only 9 patients had tympanoplasty; 30 had intact canal mastoidectomy and tympanoplasty; and 9 had open cavity mastoidectomy and tympanoplasty. Hearing reconstructions were performed in 27 (56%) patients with ossicular prosthesis and in 21 (44%) patients with mobilization.
Seventeen (35%) patients had deviation and 31 (65%) patients had no deviation. Inferior deviations were observed in 8 patients and superior deviations in 10 patients (1 had both inferior and superior) on the ipsilateral side of tympanosclerosis. Patients with moderate (8 patients: an NSD angle of between 9° and 15°) and severe (9 patients: an NSD angle more than 15°) deviation according to Elahi et al were included. 2
Table 1 shows the preoperative and postoperative pure tone audiometry scores of patients with or without NSD. When compared to preoperative scores, the postoperative scores of the air-conduction threshold average and ABG showed significant improvement (P < .05). No significant difference was found between preoperative and postoperative bone-conduction threshold averages (P > .05).
Pure Tone Audiometry Threshold Averages.a
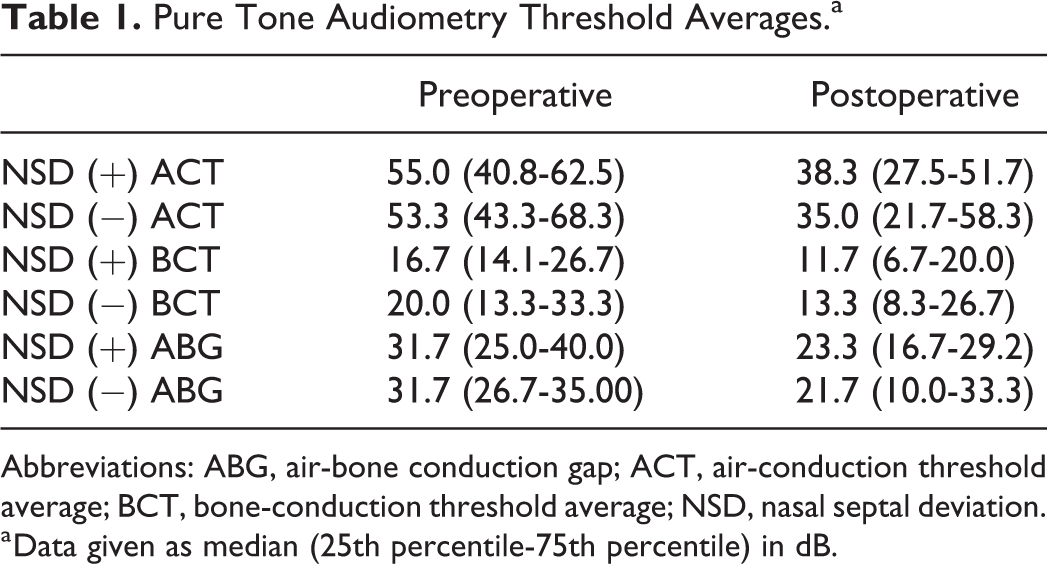
Abbreviations: ABG, air-bone conduction gap; ACT, air-conduction threshold average; BCT, bone-conduction threshold average; NSD, nasal septal deviation.
a Data given as median (25th percentile-75th percentile) in dB.
Functional success was compared according to the criteria of the Otological Society of Japan (2000). Table 2 shows the number of successes for both groups and their percentage of the total number of patients. We noticed success in 14 (45%) patients without deviation and in 9 (53%) patients with deviation. There was no significant difference (P = .606).
Assessment of Postoperative Hearing Results According to the Criteria of the Otological Society of Japan (2000).
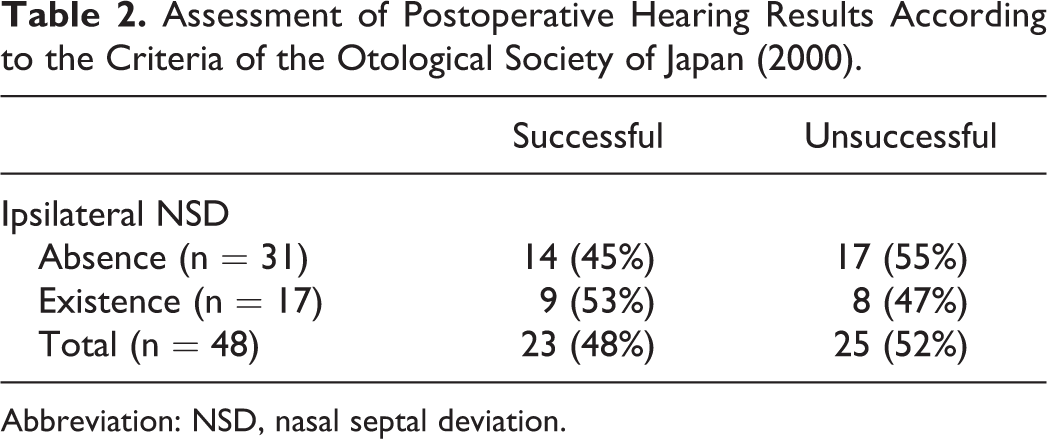
Abbreviation: NSD, nasal septal deviation.
Discussion
Sinonasal structures and the middle ear space have similarities in terms of both embryologic development and histological structure. 3 This similarity and togetherness also applies to postnatal life. It has been reported that NSD decreases mastoid bone volume 4 and that reductions in the nasal airflow increases otologic pathologies like otitis media. 5
Surgery in tympanosclerosis is controversial for some authors 6 because of the long-term deterioration. Our previous study showed no significant deterioration but it did show worsening scores over time. There are many explanations for this worsening situation.
Yeolekar noticed that 82% of ear pathologies improved after correcting the nasal pathology. 7 As Akyıldız has pointed out, when we retrospectively observed patients with NSD and without any intervention to the nose, there are significant differences in the otologic surgery results. 8 In contrast, Maier and Krebs suggested not operating on all septal deviations before tympanoplasty. 9 Along with Maier and Krebs, therefore, we suggest that only NSD has no effect on eustachian tube dysfunction or hearing deterioration. Inflammatory situations may have a bigger role by affecting the eustachian tube mucosa, but we excluded the patients with mucosal diseases.
Taking into consideration the limited number of patients and our retrospective observations, we suggest that an intervention comprising only of NSD as only pathology had no meaningful effect on ear surgery. However, prospective studies with more patients should offer more certain information.
Footnotes
Authors’ Note
Some data in this study have been presented by Fatih Mutlu in 40th Turkish National ENT&HN Specialists Congress, November 7 to 11, 2018, Antalya, Turkey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.