
Abstract
A 45-year-old female who had undergone Nissen fundoplication for long-standing laryngopharyngeal reflux (LPR) developed episodes of coughing and throat clearing. Strobovideolaryngoscopy demonstrated evidence of LPR with a reflux finding score of 11. A cough workup including a chest X-ray and pulmonology consultation was negative. Consultation with a nutritionist revealed Histamine intolerance. Histamine-free diet resulted in marked improvement in patient’s symptoms and examination.
Introduction
The most common symptoms in patients with laryngopharyngeal reflux (LPR) are hoarseness, dysphagia, cough, chronic throat clearing, and sore throat. 1 There are many conditions that may cause, aggravate, or mimic LPR; there has been skepticism about the role of food sensitivities in both LPR and gastroesophageal reflux disease (GERD). The following case suggests that uncommon food sensitivities, such as to Histamine containing food, may aggravate or mimic LPR.
The patient was a 45-year-old female with a 3-year history of LPR and with right superior laryngeal nerve paresis, 3-year status post right vocal fold fat injection. Medical history included Hashimoto thyroiditis, migraines, and she was a carrier for the methylenetetrahydrofolate reductase mutation. The patient underwent Nissen fundoplication prior to our initial evaluation. A 24-hour double-probe pH impedance testing on reflux medications before surgery demonstrated 219 reflux events (119 acidic and 100 weakly acidic; 146 events occurring while the patient was upright. Sixty-six reflux events reached the proximal esophagus, 46 of which occurred while the patient was upright; 17 were acidic and 51 were weakly acidic. The patient was seen 6 months after the surgery and was off all reflux medication. She complained of persistent cough and episodes of throat clearing. No other symptoms were reported. Strobovideolaryngoscopy revealed signs of LPR with a reflux finding score (RFS) of 11 (Figure 1). A 24-hour double-probe pH impedance study post Nissen fundoplication revealed a total of 28 reflux events, 6 reflux events reached the proximal esophagus (5 weekly acidic and 1 nonacidic), none of which occurred while the patient was supine. No intraesophageal reflux was seen. Symptoms index was positive for cough. Cough workup, including a chest X-ray, pulmonology consultation, mycoplasma levels, pertussis evaluation, and other assessments, was negative.
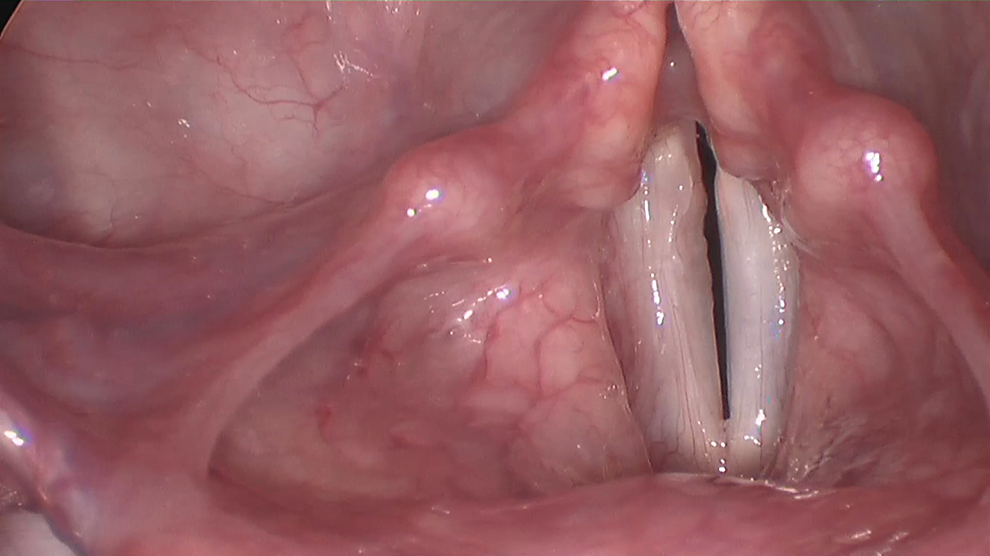
Rigid video stroboscopic examination 6 months following Nissen Fundoplication showing arytenoid erythema and mild laryngeal edema.
The patient was sent for a nutritionist for consultation, and Histamine intolerance was discovered. Once a histamine-free diet was implemented, the patient’s RFS improved to 6 (Figure 2), and the patient reported substantial improvements in cough and throat clearing. The patient was followed up for 6 months with the same outcomes.

Rigid video stroboscopic examination following Histamine-free diet showing significant improvement in erythema.
Discussion
Laryngopharyngeal reflux is an expensive, high-prevalence disease that affects at least half of patients with laryngeal and voice disorders. 2 Several factors contribute to this disorder including ineffective lower esophageal sphincter and esophageal dysmotility. Food sensitivities have been addressed as possible cofactors that might cause irritation of the GI system and increased acid production, 3 but the importance of food sensitivities remains controversial.
There are limited data on specific food sensitivities. However, it seems possible that the prevalence has increased, as food allergies have been documented increased, and has been regarded by some investigators as the “second wave” of the allergy epidemic with an associated increase in public health burden. 4 However, the prevalence of food allergies has been difficult to measure definitively. Confirming an allergy via food challenge test is resource-intensive and still somewhat controversial. Among the data that are available, most have relied on self-reporting which tends to overestimate the prevalence of a food allergy. 5 In the United States, the prevalence of self-reported food allergies was 8.0% (95% CI: 7.6-8.3) among children 18 years of age or under. 6 However, other countries have shown a 10% prevalence of a challenge-proven food allergy among infants using a food challenge test as the gold standard. 7
Food sensitivities, to be distinguished from a food allergies, are thought to be a non-IgE innate immune-mediated responses to food antigens. They have been associated with numerous etiologies, many of which are involved absence of a particular enzyme needed to fully digest a specific food. Common symptoms associated with food sensitivities include abdominal pain, bloating, headache, fatigue, joint pain, and depression. However, many patients live a lifetime without recognizing the existence of a food sensitivity due to delayed and vague symptoms that may mirror other common ailments. While gluten sensitivity is one example that has been of particular research interest, sensitivity to histamine has been studied increasingly.
Foods rich in histamine include pickled and canned foods, matured cheeses, smoked meat products, shellfish, walnuts, beans, chocolate and other cocoa-based products, and alcohol. Histamine is recognized as a biologically active substance that leads to inflammatory and immune responses. It plays a regulatory role in the gut and acts as a neurotransmitter. 8 Antihistamines inhibit these effects by targeting histamine receptors, either H1 or H2. H1 receptors are targeted typically in treating allergic reactions and mast cell–mediated disorders. H2 antihistamines are used to treat GERD and LPR because they reduce stomach acid by blocking H2 receptors in parietal cells of the gastric mucosa. It has been suggested that lack of diamine oxidase cause diminished histamine degradation and leads to the development of histamine sensitivity. 9
The benefits of a histamine-free diet have been explored among patients with food intolerance or allergic disease. Improvements in various symptoms have been reported including bronchial asthma, headache, and in patients previously symptomatic with atopic eczema, urticaria reaction occurred with ingestion of foods rich in histamine. Another study found similar results, with a majority of patients reporting significant improvement in headache frequency, duration, and intensity. 10 Diagnosis of food sensitivity usually relies on symptoms before and after a diet change, blood tests, and exclusion of other diseases. However, diagnostic testing involving study of patients’ fecal samples has been proposed. 11
Twenty-four pH monitoring is the most important study to quantify esophageal reflux and determine whether symptoms are related to LPR. In this study, manometry was performed first in order to place the pH catheter appropriately. An antimony catheter (VersaFlex LPR ZNID15 + 8R; Given imaging Ltd, model number FGS-9000-17, dual pH channel 15 cm apart, 8 impedance rings at −3, −1, 1, 3, 5, 12, 14, and 16 cm from distal pH channel, 6.0F, 10/pkg) was then placed transnasally into the esophagus. The lower probe was placed 5 cm above the LES in accordance with the standard of care in the gastroenterological literature. Impedance manometry study revealed that the length of esophagus in this patient was 25 cm (UES location 19.0 cm from nares, LES location 44.0 cm from nares). This means that the proximal sensor was high in the esophagus, approximately 5 cm below the UES. Thus, it could have overestimated the number of gastric events reaching the pharynx but not missed events. The patient was instructed on how to use the 24-hour patient diary and the Digitrapper. After approximately 24 hours of recording, the patient returned to the office and verified the written diary and the probe was removed. Our patient had confirmed severe LPR, a good result from Nissen fundoplication, and persistent symptoms. The discrepancy troublesome symptoms and favorable reflux measure lead to the search for another cause. Discovering of histamine sensitivity and related treatment leads to improvements in symptoms and signs. No other cause was identified for this improvement.
Conclusion
Implementation of a histamine-free diet in selecting patients with LPR appears to have beneficial effects. Therefore, the relationship between LPR and food sensitivity should be considered, especially in patients who do not respond as expected to typical treatment. Additional information on the prevalence of food sensitivities and their impact on reflux disease is required. Further evidence supports reduced reflux symptoms with diet modifications related to food sensitivities, if that information could change to diagnosing and treating LPR potentially decreasing medication use for some patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.