
Abstract

A 79-year-old male presented to the head and neck surgical clinic with globus sensation and no other significant head and neck symptoms. He was a nonsmoker and had minimal alcohol intake. His background was notable for metastatic melanoma initially resected in the right forearm 8 years previously with current disease sites in bilateral adrenal glands (that had remained stable) alongside a progressive lesion in the sacrum, for which he had undergone radiotherapy. He was currently stable on single agent immunotherapy (nivolumab). Positron emission tomography demonstrated an intensely fluorodeoxyglucose avid lesion in his right vallecula/tongue base region (Figure 1) alongside his stable sacral and adrenal disease (Figure 2). Full head and neck examination including flexible nasopharyngolaryngoscopy elucidated a large mucosal lesion in the right glossotonsillar sulcus encroaching upon his supraglottic airway but no other upper aerodigestive lesions and no neck nodes on palpation.
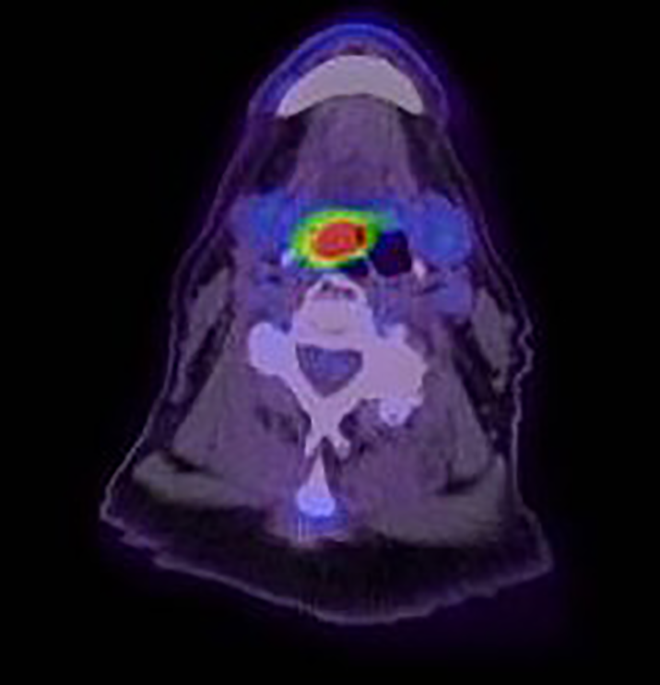
Positron emission tomography (PET) scan showing fluorodeoxyglucose (FDG) avidity in the right base of tongue/glossotonsillar region.

Positron emission tomography (PET) scan showing fluorodeoxyglucose (FDG) avidity in the adrenal glands (left) and sacrum (right).
Examination under general anaesthesia was performed to gain a tissue diagnosis but also for debulking in order to protect his airway; this confirmed a vascular exophytic mass in the right glossotonsillar sulcus/tongue base region that was debulked (Figure 3). Histopathology demonstrated sheets of tumour cells within the lamina propria and submucosa without overlying melanoma in situ in the squamous epithelium. The tumour cells are epithelioid, with enlarged pleomorphic nuclei, prominent nucleoli, and abundant cytoplasm. There are frequent mitotic figures and no pigment, keratin, or glands were seen. Immunostaining confirmed expression of S100, SOX10, melan-A, and BRAF V6000E in the tumour, in keeping with a diagnosis of metastatic melanoma. high-molecular weight cytokeratin (HMWCK) was negative (Figure 4). The expression for BRAF V600E on immunohistochemistry is in keeping with the molecular findings of mutation in BRAF Exon 15 (BRAF p.Val600Glu), which results in constitutive activation of mitogen activated protein kinase (MAPK) signaling, predicting clinical response to selective BRAF inhibitors. The constellation of features in this case, that is, prior history of cutaneous melanoma, lack of in situ change in the overlying squamous mucosa, and presence of BRAF mutation is consistent with metastatic melanoma rather than primary mucosal melanoma. The genomic landscape of melanoma show that mucosal melanomas to have low mutation burden, with predominance of KIT and NRAS aberrations. BRAF mutations are only rarely seen in mucosal cases, in contrast to cutaneous melanomas. 1

Intraoperative endoscopic images demonstrating right glossotonsillar/tongue base mucosal lesion pre biopsy.
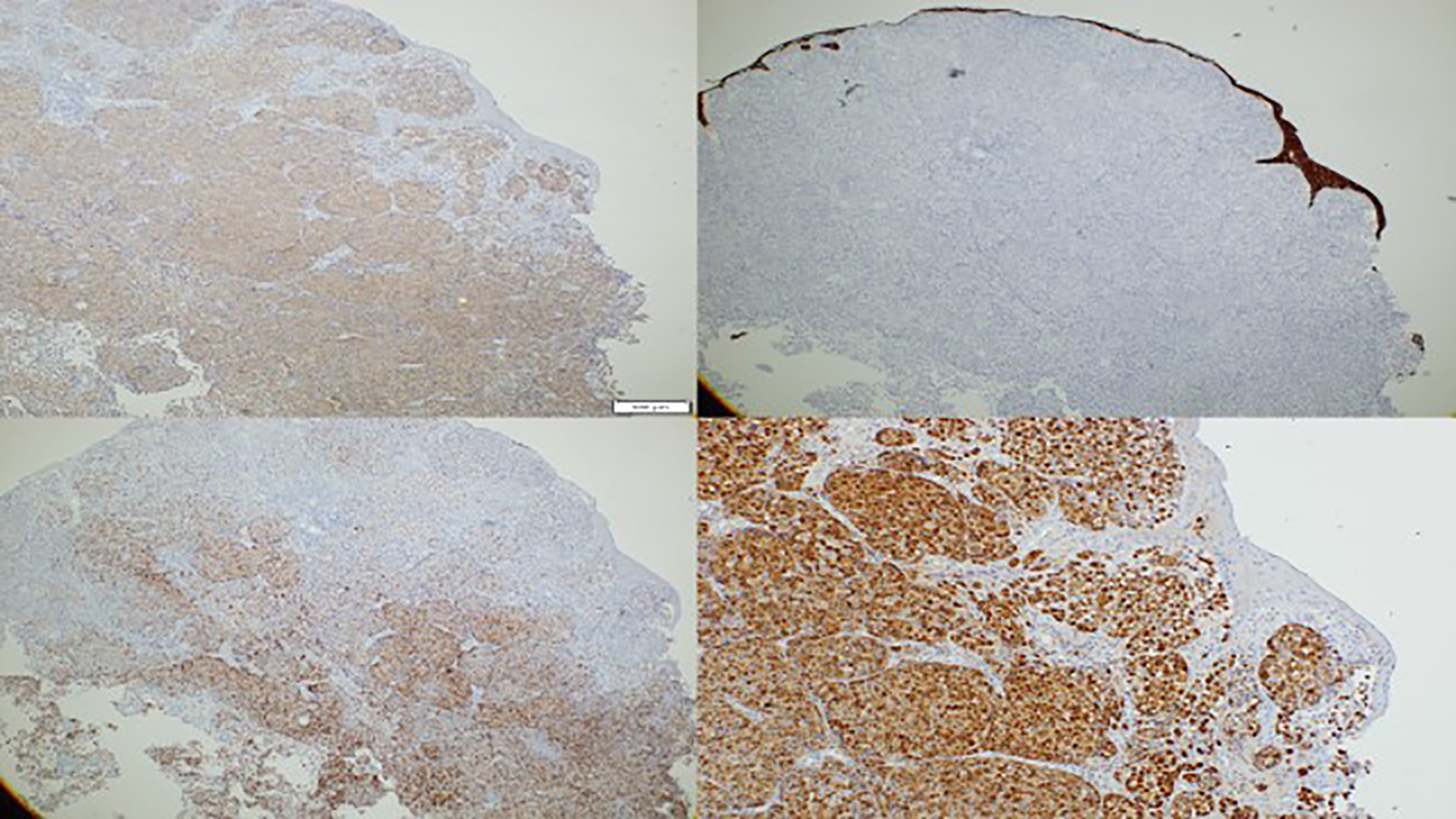
Pathology slides showing immunostaining: Left top BRAF V600E, Right top HMWCK, Left bottom Melan-A, Right bottom S100.
He was discussed at both head and neck and melanoma multidisciplinary meeting. Given his overall disease burden, location of the tumour in the tongue base and the patient’s wishes, he underwent palliative radiotherapy which led to local control at time of last review.
The head and neck region can be affected by both cutaneous melanoma and mucosal melanoma.2,3 Cutaneous malignant melanoma has a high potential of both lymphatic and hematogenous spread, as is demonstrated by this case. However, metastases to the upper aerodigestive tract are rare. 4 It is worth reinforcing that, as in this case, such lesions in the head and neck are not necessarily pigmented, and can also be submucosal. 5 Both pharyngeal tonsil and tongue metastases have been reported in the literature but there is no previous report of metastatic disease in the tongue base or vallecula.4-9 It is thought that head and neck metastases typically represent advanced stage disease and as such, surgical procedures are often limited to biopsy only but commonly extend to debulking for local disease control and quality of life (such as relief of obstruction or bleeding) alongside, in some rare instances, curative intent extensive resections such as laryngectomy. Prognosis remains poor however for those presenting with head and neck mucosal metastases, but with the advent of novel immunotherapy agents, this is potentially changing.4,5
Given the increasing worldwide incidence of melanoma and that 20% will develop distant metastases, otolaryngologists need to be cognisant of this differential, take a thorough history and physical examination alongside ensuring patients are discussed in appropriate multidisciplinary meetings. 4
Footnotes
Authors’ Note
Informed consent was obtained prior to writing this report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.