
Abstract
Introduction:
Transoral surgery for head and neck cancer provides excellent oncologic outcomes while preserving speech and swallowing function. When neck dissection and resection of oropharynx are performed concomitantly, there is a risk of creating a communication defect or developing a pharyngocutaneous fistula. To prevent pharyngocutaneous fistula, we performed the reconstruction using a posteriorly based lateral tongue flap for communication defect.
Patient:
A 72-year-old male with oropharyngeal cancer (tonsil cancer) T2N1M0 underwent concomitant transoral videolaryngoscopic surgery and neck dissection. The lateral wall of the oropharynx was resected with the pharynx constrictor muscle and parapharyngeal fat due to infiltration of the parapharyngeal space by the tonsil cancer. The posteriorly based lateral tongue flap was used to close the perforation. There was no leakage to the neck postoperatively. The patient had no problem with phonation or oral intake and remained free of disease at 12 months after treatment.
Conclusion:
For a small defect confined to the oropharyngeal lateral wall, the posteriorly based lateral tongue flap should be considered as a useful option for reconstruction of the oropharynx without impairment of posterior function.
Introduction
Driven by the desire to offer a less morbid alternative to chemoradiation, minimally invasive surgical techniques for head and neck squamous cell carcinoma continue to be frequently reported in the head and neck literature. These techniques include transoral laser microsurgery and, more recently, transoral robotic surgery (TORS). 1 In addition, alternative transoral surgery (TOS) methods such as transoral videolaryngoscopic surgery (TOVS) and endoscopic laryngopharyngeal surgery (ELPS) have been developed. These endoscopic transoral procedures provide excellent oncologic outcomes while preserving speech and swallowing function.2-5 One of the advantages in TOS is its superior ability to maintain swallowing function relative to chemotherapy.
Transoral surgery for tonsil cancer is based on the concept of transoral lateral oropharyngectomy. When neck dissection is performed concomitantly, there is a risk of creating a communication defect or developing a pharyngocutaneous fistula. A previous study reported that when neck dissection was performed concomitantly with TORS, the rate of intraoperative pharyngocutaneous fistula was as high as 29%. 6
Several reconstruction methods, such as local flap and free flap, have been reported for oral and pharyngeal defects. Reconstruction methods are selected based on the size and position of the defect. We performed the reconstruction using a posteriorly based lateral tongue flap to correct a communication defect caused by concurrent TOS and neck dissection to treat tonsil cancer.
Patient Report
A 72-year-old male felt discomfort in his pharynx and was diagnosed with tonsil swelling at another hospital. He was referred to our department for diagnosis and treatment. The patient has hypertension, for which he requires medication. His performance status was 0 according to the Eastern Cooperative Oncology Group classification system. Transnasal endoscopic examination revealed a tumor protruding from the tonsil, slightly infiltrating the tongue base. Neck ultrasonography revealed lymph node swelling in the upper neck. Contrast-enhanced T1-weighted magnetic resonance imaging of the neck showed a protruding tumor that had invaded the pharyngeal constrictor muscle with nonhomogenous enhancement, and lymph node swelling in the upper deep neck with suspicion of extranodal infiltration and close contact with the internal carotid artery (Figure 1). Biopsy of the tumor showed squamous cell carcinoma without p16 negativity. Positron emission tomography revealed intense fluorodeoxyglucose (FDG) uptake in the pharynx and right neck, but no uptake at another lesion. The patient was diagnosed with oropharyngeal cancer T2N1M0.
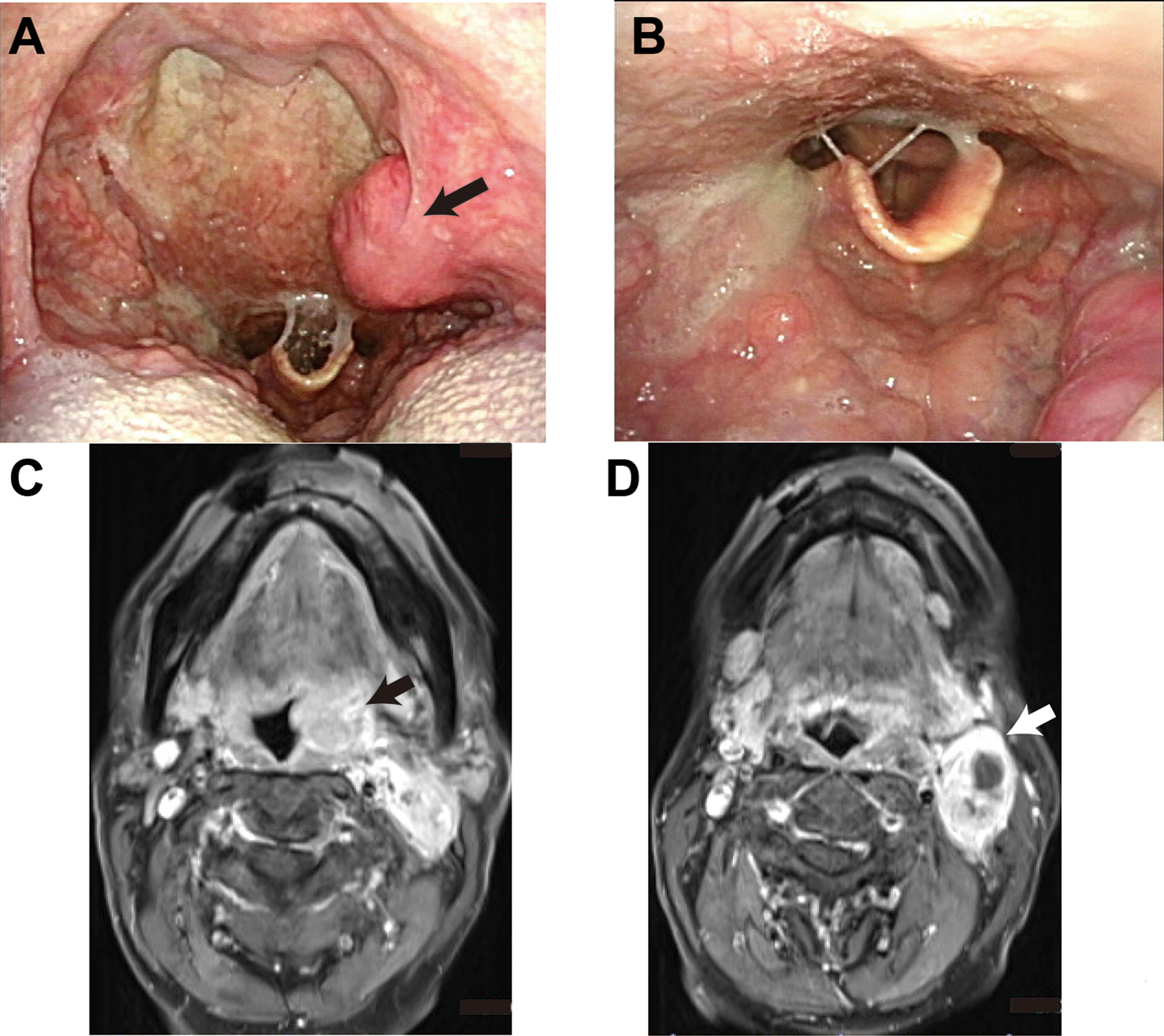
Tonsil cancer findings with transoral endoscopy and contrast-enhanced T1-weighted magnetic resonance imaging of the neck. Transnasal endoscopic examination revealed a tumor protruding from tonsil (black arrow; A), slightly infiltrating the tongue base (B). Contrast-enhanced T1-weighted magnetic resonance imaging of the neck revealed a protruding tumor with invasion of the pharyngeal constrictor muscle with nonhomogenous enhancement (black arrow; C), and lymph node swelling in the upper deep neck with suspicion of extranodal infiltration and close contact with internal carotid artery (white arrow; D).
The patient received 2 cycles of preoperative chemotherapy including docetaxel (60 mg/m2, day 1), cisplatin (60 mg/m2, day 4), and fluorouracil (days 1-5). There were no adverse effects during the chemotherapy. Chemotherapy decreased the tumor volume of both the tonsil cancer and the neck lymph node, creating some distance from the internal carotid artery. The patient underwent TOVS and neck dissection. The TOVS procedure was based on a report by Tomifuji et al. 7 The patient underwent nasotracheal intubation and was placed in the supine position. An FK-WO TORS Laryngo-pharyngoscope retractor (Olympus, Tokyo) was positioned to provide sufficient working space. A flexible endoscope capable of angulation in 4 directions (Visera LTF-type VP, Olympus) was inserted through the oral cavity while an assistant held and manipulated the endoscope for surgical field visualization. The operator employed a single-use electrosurgical knife with radiofrequency alternating current (KD-600, Olympus) to resect the tumor during TOVS. A Swift model (output power 30, effect 4) with a high-frequency surgical system (ERBE VIO300D) was used. Transoral lateral oropharyngectomy was performed according to a previously published surgical method. Because infiltration of the parapharyngeal space by tonsil cancer was suspected based on preoperative findings, the lateral wall of the oropharynx was resected with the pharynx constrictor muscle and parapharyngeal fat. The tumor was resected completely with a sharp margin. Subsequently, the patient underwent selective neck dissection (II-IV). Thus, there was communication between the oropharynx and neck. The perforation was located at the lateral wall, and reconstruction for the primary closure technique was performed transorally. We selected the lateral tongue flap. The incision was performed 1 cm away from the tongue midline. Posteriorly, a basal lateral tongue flap was created by full-thickness incision of the tongue in the anterior to posterior direction. The flap was rotated and sutured to the lateral wall (Figure 2).
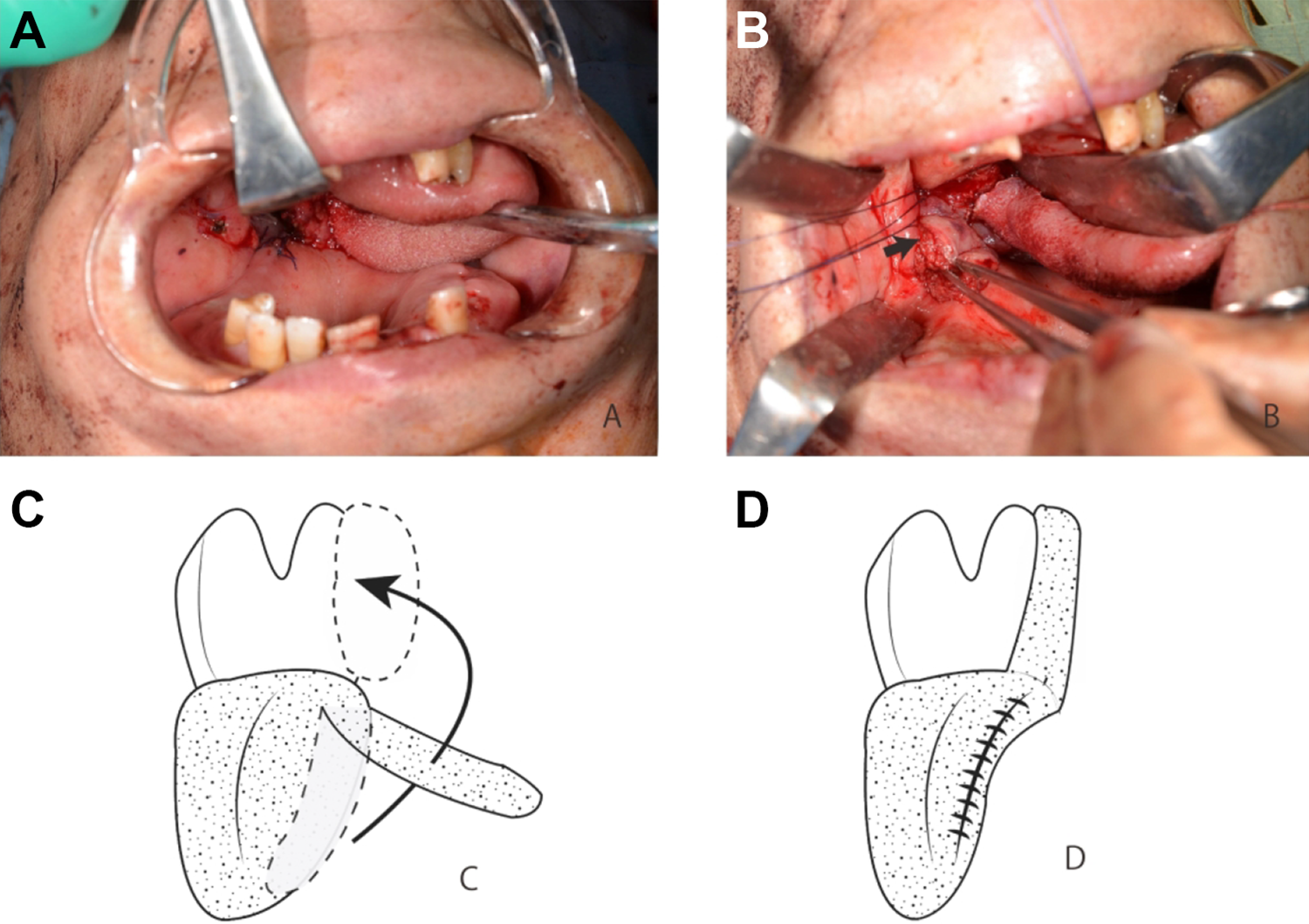
Intraoperative findings. Posteriorly basal lateral tongue flap was created by full-thickness incision of the tongue in the anterior to posterior direction (A). Tongue flap is shown as a black arrow (B). The flap was rotated and sutured to the lateral wall (C and D).
Tracheostomy was performed intraoperatively. No serious adverse events arose requiring further intervention. A nasogastric tube was inserted into the stomach postoperatively for tube feeding. A postoperative videofluoroscopic swallowing study revealed moderate penetration and pharyngeal residue, but no aspiration or leakage into the neck (Figure 3). The duration of nil per os was 7 days. There was no problem with phonation. The patient remained free of disease 12 months after treatment.

Postoperative pharyngeal findings. The tongue base flap was engrafted to the lateral pharyngeal wall, shown as a black arrow. There was no leakage.
Discussion
Transoral robotic surgery has been reported to be a feasible, safe, and effective procedure for the resection of benign and malignant oropharyngeal, supraglottic, and hypopharyngeal tumors. 1 Furthermore, alternative transoral surgical methods have been developed, such as TOVS and ELPS. These endoscopic transoral procedures provide excellent oncologic outcomes while preserving speech and swallowing function.2-5
In particular, TOS is indicated for resection for tonsil cancer. Transoral surgery for tonsil cancer is based on the concept of transoral lateral oropharyngectomy. The lateral oropharynx contains 3 distinct fasciae (from superficial to deep): the capsule of the tonsil; the pharyngobasilar fascia, which covers the first layer of the superior pharyngeal constrictors; and the buccopharyngeal fascia, which provides a deep layer of protection between the superior constrictor muscle and the retrostyloid parapharyngeal space. 8 The resection plane is the submuscular plane, preserving the buccopharyngeal fascia. Accordingly, there are few opportunities to create a communication defect from the pharynx to the neck. However, if the cancer has invaded through the buccopharyngeal fascia to the parapharyngeal space, parapharyngeal fat should be restricted. Thus, when neck dissection is performed concomitantly, there is be a risk of creating a communication defect or developing a pharyngocutaneous fistula. A previous study reported that when neck dissection is performed concomitant with TORS, the rate of intraoperative pharyngocutaneous fistula is as high as 29%. 6
In general, staged neck dissection is followed by TORS to prevent pharyngocutaneous fistula. This approach has several advantages. First, it can decrease tracheostomy. Furthermore, histologic examination can evaluate extracapsular invasion of the neck lymph node and the number of metastatic lymph nodes. Histologic findings can determine the indication for adjuvant therapy. On the other hand, staged neck dissection also has several disadvantages. First, patients require additional general anesthesia and hospitalization. Second, the schedule for adjuvant therapy will be delayed. Third, dissection of the parapharyngeal space will not be adequate. In cases with deep invasion, TOS should be performed concomitantly with neck dissection to dissect the parapharyngeal space; this requires reconstruction of the defect. Our patient underwent neck dissection followed by TOVS to resect the primary tumor and dissect pericarotid fat en bloc, resulting in a communication defect.
Several reports have described reconstruction for communication in oropharyngeal cancer using free flap or local flap. Local flaps such as the palatal flap, submental, buccal mucosal, and tongue flap are used to close small- to moderate-sized defects. Large defects such as total palatal, which is more than 50% of the tongue base, and composite pharyngeal defects may be closed with a regional myocutaneous pedicle flap such as the pectoralis major lower trapezius, or latissimus dorsi pedicle flap and microvascular flap. 9 The defect of this patient was not large and was limited on lateral pharyngeal wall. Therefore, we thought that a local flap would be appropriate for the reconstruction.
Moore et al reported criteria for primary closure reconstruction for communication defect. Defects less than 1 cm in diameter were managed via transoral or transcervical primary closure of the constrictor muscle. Defects greater than 1 cm in diameter were closed primarily and reinforced with muscular coverage using the digastric and mylohyoid muscles. They reported 6 cases of fistula formation out of 42 cases. 6 Nam et al reported on an additional method of reinforcement in addition to that proposed by Moore et al by anchoring the digastric–mylohyoid complex to the mandible. Zero of their 13 patients had a postoperative fistula. 8 In this case study, our patient was elderly individual; thus, preservation of the suprahyoid muscles was important for preserving swallowing function. Accordingly, we selected the transoral flap.
Tongue flaps have been used to close intraoral defects following tumor surgery, severe infection, trauma, and cleft palate fistulas. In addition, tongue flaps are useful after radiation therapy due to good blood flow. 10 Anterior-based tongue flaps are useful for treating defects of the hard palate, anterior buccal mucosa, lips, and anterior floor of the mouth.11,12 Posterior-based flaps are indicated when treating defects of the soft palate, retromolar region, floor of the mouth, and posterior buccal mucosa.13,14
Several reports have described tongue flaps in various formats (setback, anterior-based, posterior-based lateral) for transposition into a variety of defects. 15 The set-back tongue flap method was reported by Schechter et al. However, this procedure was limited to defects of the tongue base and excluded defects involving the floor of the oral cavity or lateral wall of oropharynx.16,17 The defect in this patient was limited to the lateral pharyngeal wall, and the tongue base defect was small. Thus, we selected a local flap such as a posterior lateral tongue flap.
This patient had no problem with postoperative swallowing function or phonation despite his age, and decannulation could be completed early. This procedure might be useful for patients who require adjuvant therapy.
Conclusion
A patient with tonsil cancer T2N1M0 underwent neck dissection and TOVS, resulting in a communication defect by dissecting pericarotid fat en bloc. Reconstruction using a posteriorly based lateral tongue flap was performed concurrently for communication defect.
For a small defect confined to oropharyngeal lateral wall, a posteriorly based lateral tongue flap represents a useful option for reconstruction of the oropharynx without impairment of posterior function.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.