
Abstract
Objectives:
Cochlear implantation (CI) has been successfully used to restore hearing in patients with severe to profound hearing loss. In addition to hearing loss, irradiated patients with nasopharyngeal carcinoma (NPC) also often have chronic otitis media and Eustachian tube (ET) dysfunction. These features may result in difficulties in CI. We conducted this study to review the management options for irradiated patients with NPC undergoing CI. Furthermore, we investigated the results of CI in irradiated patients with NPC with chronic otitis media and obstructive ET dysfunction, accordingly to different treatment strategies.
Methods:
We retrospectively reviewed the data of patients with NPC who underwent CI in our hospital between 2006 and 2020. All subjects were found to be eligible according to the following inclusion criteria: had NPC, received irradiation, underwent cochlear implant surgery, and had chronic otitis media with obstructive ET dysfunction.
Results:
A total of 9 patients with obstructive ET dysfunction and chronic otitis media underwent cochlear implant surgery. Seven patients with an inflamed ETs underwent a 2-stage operation. Two patients with obliterated ETs, we performed a single-stage CI surgery. Only 1 patient had otitis media effusion after the surgery.
Conclusion:
With the proper management of chronic otitis media and ET dysfunction, cochlear implant is an effective treatment for irradiated patients with NPC when conventional hearing aids failed.
Keywords
Introduction
In Southeast Asia, nasopharyngeal carcinoma (NPC) is a common head and neck cancer. 1 Radiotherapy is the mainstay treatment for NPC, and platinum-based chemotherapy is used in nearly all stages of NPC. Sensorineural hearing loss can start soon after radiotherapy. The early changes are reversible. However, the probability of persistent hearing loss continues to increase over time. 2 Following cisplatin chemotherapy, 40% to 80% of adults are left with permanent hearing loss. 3 In Taiwan, approximately 51% of patients with NPC have moderate to severe hearing impairment during cancer-free survival after treatment. 4 Cochlear implantation (CI) is an effective treatment modality for hearing restoration in patients with NPC when conventional hearing aids (HAs) have failed. 5 -7
In addition to hearing loss, irradiated patients with NPC also often have Eustachian tube dysfunction (ETD), otitis media with effusion (OME), and chronic otitis media (COM). These features may result in difficulties during CI in patients with NPC. First, insertion of an electrode is inappropriate in patients with a perforated eardrum or chronic infection because of the risk of meningitis and extrusion of the electrode from the perforated eardrum. Second, chronic inflammation causes the formation of adhesions and granulation in the middle ear and mastoid cavity. This may easily cause bleeding and difficulty in finding the round window niche during CI surgery. Third, obstructive ETD may cause OME and thus increase the risk of device infection. Lastly, electrode array extrusion from fragile bone need to be noticed (especially posterior canal wall) during and after the operation.
We conducted this study to assess the management options for irradiated patients with NPC undergoing CI. Furthermore, we investigated the results of CI in irradiated patients with NPC with COM and obstructive ETD, accordingly to different treatment strategies.
Patients and Methods
Study Design
This retrospective study was conducted in a tertiary referral center. The data of patients with NPC who underwent CI were retrospectively collected from 2006 to 2020 after obtaining the appropriate approval from the ethics research committee (REC 108-30).
Patient Selection and Data Collection
Nine subjects were found to be eligible using the following inclusion criteria: irradiated patients with NPC who had severe to profound hearing loss, underwent CI, and had COM with obstructive ETD. Three patients with NPC with intact drums and good Eustachian tube function (ETF) during the same period were excluded. The clinical history of NPC, including year of diagnosis and stage, treatment received, otoscopic examination results, ETF assessment, and high-resolution computed tomography (HRCT) scans of the temporal bones were collected.
Eustachian Tube Function Assessment
Currently, the diagnosis of obstructive ETD is primarily based on patient symptoms and examination findings. In our study, obstructive ETD was defined when the patient fulfilled all 3 of the following criteria:
Surgical Technique
Two-stage operation
Seven patients with an inflamed ETs underwent a 2-stage operation. We performed tympanoplasty and canal wall up mastoidectomy with or without balloon dilation Eustachian tuboplasty (BET; Spiggle & Theis Medizintechnik GmbH) in the first stage. The pre-CI procedure was intended to improve the ETF and middle ear clearance. At least 3 months later, a healed tympanic membrane and aerated middle ear cleft were achieved, and the second stage of the CI was performed.
Single-stage operation
For the 2 patients with obliterated ETs, we performed a single-stage CI surgery: CI with mastoid obliteration and simultaneous external auditory canal (EAC) blind sac closure. First, a radical tympanomastoidectomy was performed. All of the mucosal lining and skin of the EAC were meticulously removed to prevent iatrogenic cholesteatoma. Then, the EAC was closed. Cochlear implantation was performed at the same time. We then transposed the temporalis muscle to obliterate the mastoid cavity and cover the internal receiver (Figure 1).
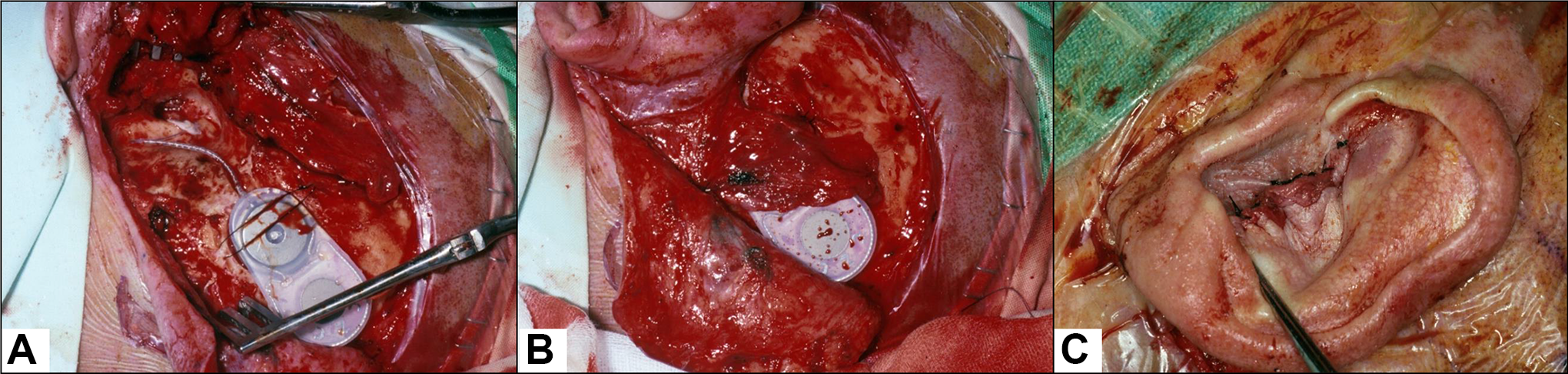
Single stage operation, that is, CI surgery (A) with mastoid obliteration (using temporalis muscle rotation flap, B) and EAC blind sac closure (C). CI indicates cochlear implantation; EAC, external auditory canal.
Outcome Assessment
We collected the ETDQ-7 scores in these patients, including the preoperative (pre-op) and postoperative 1 month (1 M), 3 month (3 M), 6 month (6 M), 1 year (1Y), and 2 years (2Y) data. Adverse effects, such as facial palsy or stimulation (even if temporary), vertigo, tinnitus, dysgeusia, or infections, as reported in the medical record during the follow-up clinical appointments, were compiled.
Data Subgrouping
Three management options were carried out according to the treatment strategies: The T + M + BET group refers to patients who underwent tympanoplasty and mastoidectomy with BET simultaneously during the pre-CI surgery. The T + M group refers to patients who underwent tympanoplasty and mastoidectomy as the pre-CI surgery. The obliterated M + EAC group refers to patients who underwent single-stage operation, that is, CI surgery with mastoid obliteration and EAC blind sac closure.
Results
Demographic Data
A total of 9 patients with NPC was included in our study, including 5 males and 4 females. The mean age at implantation was 52.8 (range 38-65 years) years old. The detailed demographic data are presented in Table 1. All patients received concurrent chemoradiotherapy due to the advanced stage of NPC. Cisplatin-based chemotherapy was administered to all patients. Hearing aids were used before the CI surgery for at least 1 year; however, all patients were unsatisfied with HAs. None of the patients had tumor recurrence during the follow-up period. The HRCT scans of the temporal bones were carefully analyzed, and none of the patients had carotid artery dehiscence.
Patients’ Demographic Data.
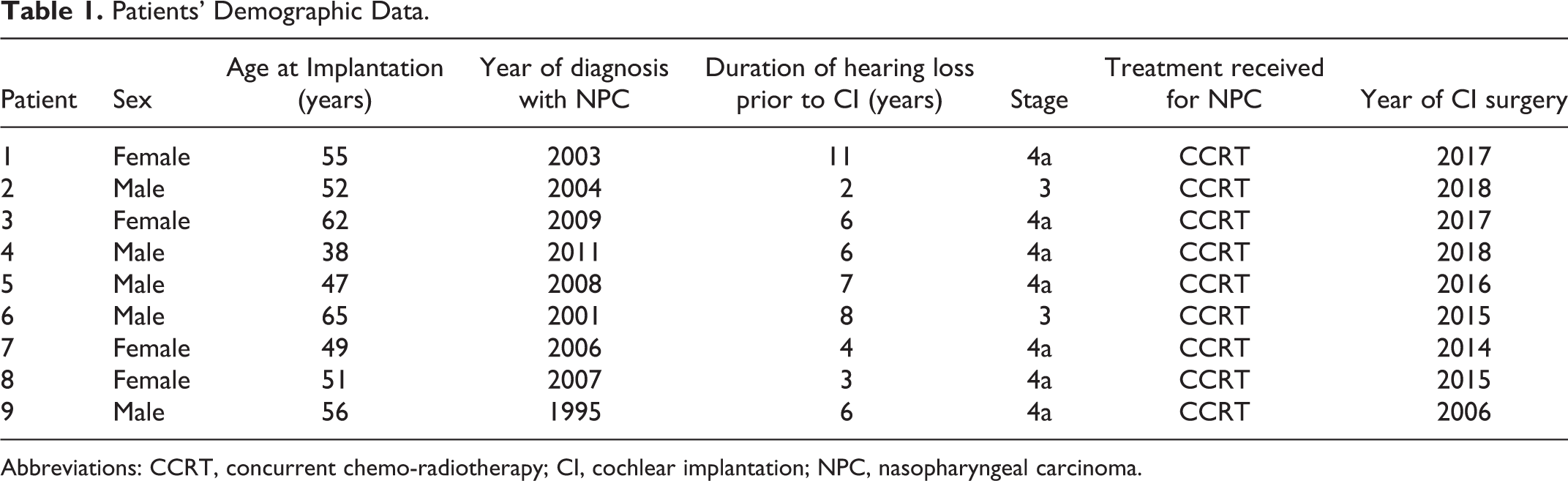
Abbreviations: CCRT, concurrent chemo-radiotherapy; CI, cochlear implantation; NPC, nasopharyngeal carcinoma.
Surgical Data and Outcomes
In our study, 9 patients with NPC had perforated ear drums, and 3 of these patients had otorrhea treated with medication to achieve a dry ear. Seven patients underwent tympanoplasty and mastoidectomy; of these patients, 4 underwent BET simultaneously, which was considered the pre-CI surgery. Cochlear implantation was performed as the second-stage operation when the middle ear cleft had aerated, and the tympanic membrane had healed in patients with NPC. The mean interval between the pre-CI surgery and CI was 3.9 months (range 3-5 months; Table 2). Two patients received a single-stage operation due to an obliterated ET.
Patients’ Surgical Data and CI Device Used.
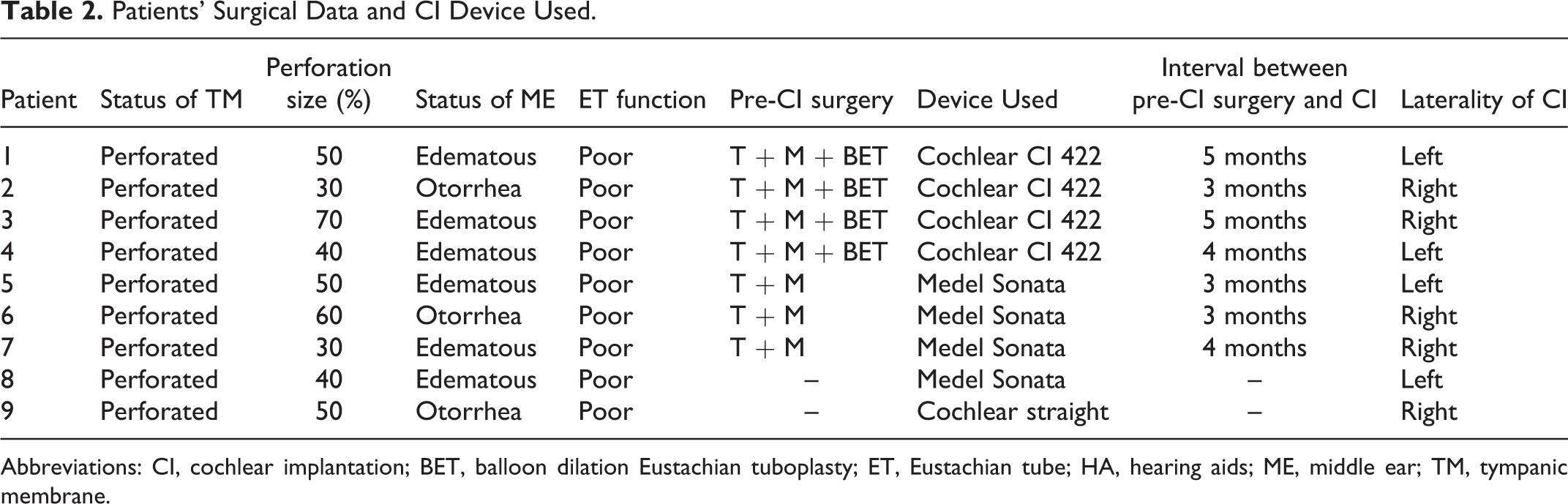
Abbreviations: CI, cochlear implantation; BET, balloon dilation Eustachian tuboplasty; ET, Eustachian tube; HA, hearing aids; ME, middle ear; TM, tympanic membrane.
All the 9 patients subsequently had good hearing and speech outcomes. Eight of 9 patients completed follow-up for at least 2 years, except for patient 4. The mean pre-op ETDQ-7 scores were 29.25, 29, and 28 in the T + M + BET group, T + M group, and obliterated M + EAC group, respectively. The mean postoperative 2Y ETDQ-7 scores were 18.33, 18.67, and 30.5 in the T + M + BET group, T + M group, and obliterated M + EAC group, respectively. Both the T + M + BET group and the T + M group showed improvement in the ETDQ-7 score postoperatively (Figure 2).
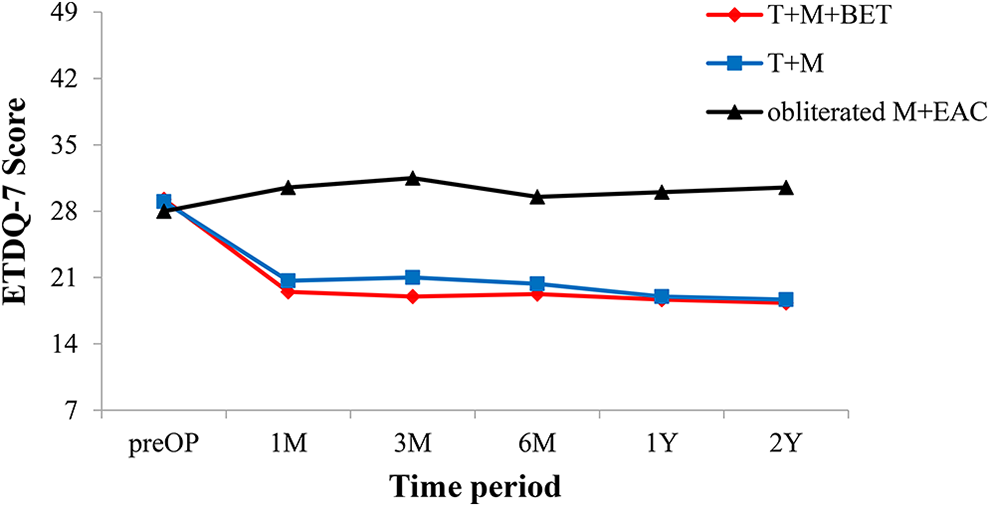
The pre- and postoperative ETDQ-7 score in each group.
Complications
Four patients smoothly underwent BET without any major complications, such as carotid artery blowout or subcutaneous emphysema. During the follow-up period, only patient 6 in the T + M group developed OME after CI surgery. After providing antibiotic medication and inserting a ventilation tube, the OME was resolved. The cochlear implant of this patient still functioned without any impairment. None of our patients had any serious complications, such as otorrhea, facial nerve palsy, vertigo, carotid artery blowout, electrode array extrusion, device infection, or meningitis.
Discussion
Special Considerations in Irradiated Patients With NPC During CI Surgery
Often, OME, COM, and osteonecrosis of the temporal bone occurs in patients with NPC after irradiation. 13 -16 For patients with NPC having intact drums and aerated middle ear clefts, CI surgery can be easily performed in a regular manner. In contrast, for patients with COM and obstructive ETD, CI surgery can be quite challenging. 5 -7 Inflamed middle ear mucosa, a perforated ear drum, an infected mastoid, and poor ETF need to be fully considered during treatment to obtain promising results.
Temporal bone osteonecrosis is a common otologic manifestation in patients with NPC after radiotherapy. The bone is more friable than non-radiated temporal bone. The surgeon must be aware of facial nerves and the dura when drilling the bone. 5 There is also a concern about carotid dehiscence in irradiated patients with NPC. Preoperative HRCT scans of the temporal bone can provide information on the relation between the ET and the bony canal of the internal carotid artery.
Restoration of ETF and Middle Ear Cleft Function
For patients with COM undergoing CI, some studies have proposed treating COM by either tympanoplasty or tympanomastoidectomy as a first-stage procedure followed by CI after 3 to 6 months, 17 while others have suggested a single-stage surgery. 18 Eustachian tube occlusion and mastoid obliteration is an effective procedure for facilitating CI in the presence of COM. 19 Whether the cavity and the ET should be obliterated during these techniques remains an area of debate.
A preoperative assessment of ETF is important to highlight the preoperative state of the ET and guide the decision-making process for patients. Balloon dilation Eustachian tuboplasty has been used as an adjunctive procedure in the treatment of COM with ETD. 20 In our opinion, for patients with NPC having an inflamed ET, BET may provide some benefits in terms of clearing the mucociliary secretions of the middle ear to prevent such sequelae. The 2-stage operation or pre-CI surgery is necessary to achieve a safe and dry ear before CI. For those with obliterated ETs after irradiation, it is impossible to restore middle ear ventilation and preserve the mucociliary clearance function. Therefore, the diseased middle ear and mastoid mucosa are radically eradicated to prevent middle ear and mastoid infections.
Application of BET in Patients With NPC
No studies have examined the utility of BET in patients with NPC (without CI). To the best of our knowledge, this is the first paper to introduce BET in patients with NPC, who then received CI subsequently.
Balloon dilation Eustachian tuboplasty is a safe procedure, even in an irradiated ear. Restoring both the ET and middle ear cleft function might prevent complications such as OME and thus decrease the risk of device infection. It is difficult to delineate the correlation between BET (or the middle ear condition) and the CI outcomes, given that the electrode array was fully inserted into the cochlea. There may be other factors that are more related to the CI outcomes than BET, such as the duration of hearing loss before CI.
We aim to highlight the principles and management options of CI in irradiated patients with NPC with COM and obstructive ETD (Table 3). We should control infection, maintain aerated middle ear cleft, and correct conductive hearing loss to obtain accurate assessment of hearing level before the CI surgery. Extreme caution should also be exercised to prevent iatrogenic cholesteatoma by ensuring that no squamous epithelium is left during obliteration of mastoid and EAC.
Treatment Strategies for Cochlear Implantation in Irradiated Nasopharyngeal Carcinoma Patients With Chronic Otitis Media and Obstructive Eustachian Tube Dysfunction.
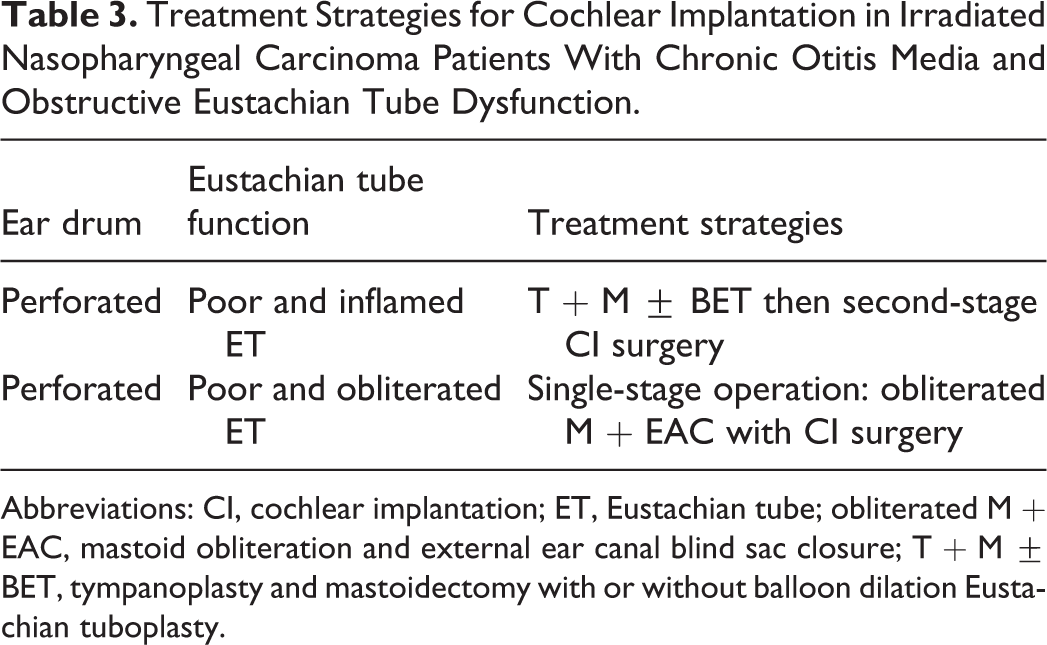
Abbreviations: CI, cochlear implantation; ET, Eustachian tube; obliterated M + EAC, mastoid obliteration and external ear canal blind sac closure; T + M ± BET, tympanoplasty and mastoidectomy with or without balloon dilation Eustachian tuboplasty.
Limitations
This is a retrospective study with a small sample size. Patients with NPC who received a cochlear implant comprised a minority in our study group. Furthermore, we included patients with complications such as COM and ETD.
It is not known whether these 3 treatment strategies resulted in different clinical impacts; a longer follow-up period will be necessary to determine the long-term outcomes and end points. A randomized, large-sample, long-term follow-up study may be warranted to further elucidate the effect of BET in patients with NPC. The assessment of complications such as CI electrode extrusion, cholesteatoma, and CI surgery revision may also require a longer period of observation.
Conclusion
With proper management of COM and ETD, CI offers feasible outcome for irradiated patients with NPC.
Footnotes
Authors’ Note
Exempt of informed consent was approved by Research Ethic Committee of Taichung Tzu Chi Hospital (REC 108-30).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by a Grant (TCMF-MP 108-01-01) from Taichung Tzu Chi Hospital, Buddhist Medical Foundation.