
Abstract
Objective:
To evaluate the effectiveness of balloon dilation (tuboplasty) of the Eustachian tube (BET) in active duty military personnel working in hyper- and hypobaric environments suffering from baro-challenge-induced ETD using functional outcomes.
Methods:
Military divers and aviators diagnosed with persistent baro-challenge-induced ETD resulting in disqualification from performing flight and dive duties and who elected for treatment with BET were included for analysis. Posttreatment follow-up assessments were undertaken at 1, 6, and 12 months. Outcome measures included successful hyperbaric chamber testing or return to the hyper- or hypobaric environment without significant baro-challenge-induced ETD symptoms and pre- and postdilation Eustachian Tube Dysfunction Questionnaire (ETDQ-7) scores.
Results:
Mean pretreatment duration of symptoms was 48 months (range: 3-120 months). Following treatment, 92% (12/13) of patients successfully returned to operational duties with resolution of limiting symptoms. Average return to duty time was 8.5 weeks (range: 6-24 weeks). The ETDQ-7 scores improved from a mean of 4.33 (2.57-6.57) predilation to 2.19 (1.00-4.43) postdilation (Z = 2.73, W = 70, P = .0063). Mean duration of follow-up was 38 weeks (range: 13-70 weeks).
Conclusion:
Eustachian tube balloon dilation appears to be a safe and highly effective treatment option for baro-challenge-induced ETD in affected military divers and aviators who work in hyper- and hypobaric environments. Further study is needed to determine whether similar results can be achieved in more diverse subject populations and to assess long-term effectiveness.
Keywords
Introduction
Eustachian tube dysfunction (ETD) is common, and while symptoms may range from mild ear discomfort to more significant symptoms associated with chronic ear disease requiring extensive surgical management, the condition is rarely life threatening in normal circumstances. 1 -3 This may not be the case with military aviators and divers who perform high-risk operations in barometrically diverse environments. Even during gradual pressure changes, episodes of acute pain and disequilibrium can significantly impact mission safety and accomplishment and can lead to fatal operational errors. While rigorous medical and performance testing generally screens out those candidates with existing dilatory ETD, occasionally some aviators and divers may still develop this condition. This may result in retraction or atelectasis of the tympanic membrane, or chronic otitis media, with associated findings evident through otoscopy, audiometry, and tympanometry. However, for others, symptoms of aural fullness, discomfort/pain, and even alternobaric vertigo may only arise in case of significant ambient pressure changes where baseline otoscopic examination and tympanometry are normal. This subtype has been classified as baro-challenge-induced ETD. 4 Although significant high-pressure alterations in such patients may cause temporary barotrauma resulting in middle ear effusion, hemotympanum, or even tympanic membrane perforation, these patients typically experience no symptoms in ambient pressure conditions. However, even in the absence of symptoms or abnormal objective findings during ambient pressure conditions, limiting symptoms leading to a diagnosis of baro-challenge-induced ETD is generally disqualifying for continued military aviation and dive-related duties.
The natural history of ETD is poorly understood, and evidence for common treatments methods is limited. There continues to be no Food and Drug Administration–approved medical therapy for dilatory ETD. Nasal steroid sprays, antihistamines, and decongestant therapies are often used as first-line treatments, although there is limited evidence to support efficacy. A randomized controlled trial failed to show any benefit of topical steroids over placebo. 5 Furthermore, a recent systematic review concluded the evidence of effectiveness for the treatment of ETD was limited for any intervention, to include observation, pharmacologic therapies, or various surgical techniques. 6
Historically, the standard surgical treatment for refractory ETD is myringotomy with tympanostomy tube insertion. This allows for equalization of middle ear pressure by effectively bypassing the dysfunctional Eustachian tube. However, tympanostomy tubes do not treat the underlying pathology and are disqualifying for duties involving diving and flying in the military population. Waivers for return to duty can be obtained for aviators as long as their tympanostomy tubes are functional and not in danger of extrusion prior to a deployment. Determination of long-term tube stability is fraught with error, and if ETD persists, tympanostomy tubes will often need to be replaced. Unforeseen tube plugging or tube extrusion in these individuals working in austere environments risks performance impairment and operational safety. For divers, tympanostomy tubes are contraindicated due to water entry into the middle ear and subsequent risk for otitis media and caloric vertigo.
Alternative surgical therapies have been investigated for select patients with endoscopic evidence of redundant or inflamed mucosa at the medial Eustachian tube orifice. Removal of this inflamed tissue using lasers or microdebriders has shown modest improvements in small, noncontrolled trials. 7,8 However, these interventions are not appropriate for all patients.
Although relatively new in the United States, balloon dilation (tuboplasty) of the Eustachian tube (BET) has proven to be safe and modestly effective in the treatment of chronic dilatory ETD. 9 -14 The objective of this retrospective cohort study was to examine our effective outcomes in utilizing BET in the treatment of military divers and aviators with baro-challenge-induced ETD. Primary outcome measures included successful hyperbaric chamber testing or return to their applicable hyper- or hypobaric environments without significant baro-challenge-induced ETD symptoms and pre- and postdilation Eustachian Tube Dysfunction Questionnaire (ETDQ-7) scores.
Patients and Methods
The study protocol was approved by the Naval Medical Center San Diego Institutional Review Board in compliance with all applicable Federal regulations governing the protection of human subjects. Military divers and aviators diagnosed with baro-challenge-induced ETD resulting in disqualification from performing flight or dive duties and who had undergone unilateral or bilateral BET from March 2017 through July 2018 at the Naval Medical Center San Diego were included for analysis. Exclusion criteria included tympanic membrane retraction or perforation, middle ear effusion, the presence or history of cholesteatoma, history of chronic ear surgery, computed tomography (CT) imaging revealing significant temporal bone or skull base abnormality which might preclude safe or effective Eustachian tube balloon dilation (to include internal carotid artery dehiscence), conductive hearing loss, asymmetric sensorineural hearing loss, Meniere disease, chronic rhinosinusitis, failure to adhere to recommended clinical follow-up, and failure to adequately undergo postdilation baro-challenge.
All patient information was retrieved from an institutional review board–approved research registry database. Relevant electronic medical record encounters were additionally reviewed. All patients reported one or more otologic symptoms of pressure, pain, vertigo, recurrent tympanic membrane perforations, or inability to equalize middle ear pressure solely and persistently during atmospheric pressure changes during diving or flying duties. All had failed a trial of medical management before dilation, which was defined as a minimum of either 4 weeks of daily intranasal steroid spray or 1 completed course of oral steroids. Baseline assessment for all patients included otomicroscopy, pneumatic otoscopy, and nasopharyngoscopy with Eustachian Tube Mucosal Inflammation Scale (ETMIS) rating. The ETMIS is a validated instrument for rating Eustachian tube mucosal inflammation using a 4-point grading scale. 15 Predilation data also included ETDQ-7 score, a validated, standardized, 7-item patient-reported questionnaire to assess symptom severity associated with ETD. 16 As patients were typically symptom-free in ambient pressure conditions, they were asked to frame their ETDQ-7 responses while in the hyper- or hypobaric environments. Audiometry, tympanometry, standardized allergy serum RAST screen, and dedicated sinus or temporal bone CT scan were also completed.
Posttreatment follow-up assessments were scheduled per protocol at 1, 6, and 12 months, where otoscopy, ETDQ-7, audiometry, and tympanometry assessments were repeated. Additional follow-ups were performed ad hoc, often via telephone consultation as needed. These additional encounters were arranged in part to ensure completeness of the database, to accommodate patient deployment schedules, to assist unit medical officers in medical fitness for duty assessments, and to allow for ongoing study assessments for determining long-term treatment efficacy. Dilations were performed using the Acclarent Aera Eustachian Tube Balloon Dilation System. All procedures were performed endoscopically under general anesthesia, with the balloon inflated to 12 Atm for 2 minutes per Eustachian tube. In cases where only 1 ear was deemed to be dysfunctional, balloon dilation was only performed for that ear. Limited septoplasty and turbinate outfracture were performed as needed for adequate access to the Eustachian tube. Patients were asked to coordinate a standard hyperbaric chamber test to 60 ft of seawater (fsw) after 5 weeks postdilation. If formal chamber testing was not feasible, patients were asked to return to flying or diving duties with appropriate and coordinated oversight for safety purposes. Return to duty status was evaluated based on a successful hyperbaric chamber test run and/or successful return to their usual hyper- or hypobaric environments with improvement or resolution of ETD symptoms which had previously precluded continuation of duties. Primary outcome measures included return to duty status, as well as pre- and postdilation ETDQ-7 scores. Secondary outcome measures included changes in audiometry or tympanometry data.
Statistical analysis was performed using a Wilcoxon signed rank test for the ETDQ-7, 2-sample t test for the audiometric data, and a McNemar test for tympanometric data. Return to duty was reported as a percentage of patients able to return to diving or flying.
Results
The first 15 military divers and aviators who met the inclusion criteria and who completed BET were included in the study. Pertinent information is given in Table 1. Eleven divers and 4 aviators were represented in our cohort. All patients were men, with a mean age of 31 years (range: 20-63 years). The average duration of symptoms predilation was 48 months (range: 3-120 months). Baro-challenge-induced symptoms most commonly included aural fullness and pain/discomfort with an inability to ascend or descend in altitude or depth. All patients reported difficulties in their ability to perform customary modified Valsalva maneuvers at the onset of symptoms with barometric challenge. Two patients presented with recurrent barotrauma manifesting as pain and recurrent tympanic membrane perforations. The perforations had healed spontaneously at the time of BET. Three divers presented with recurrent aural fullness and disabling vertigo lasting seconds to minutes following rapid ascents in the water column. Following extensive evaluations, all were determined to be due to alternobaric vertigo. An additional diver presented with recurrent complete facial paralysis with pain and aural fullness after rapid water ascents, with facial function gradually returning to normal within minutes of returning to ambient pressure conditions. Following an extensive workup, this patient was ultimately diagnosed with recurrent facial baroparesis. A total of 4 patients presented with predominantly unilateral baro-challenge-induced ETD complaints (all right ears).
Cohort Details and Outcomes.a
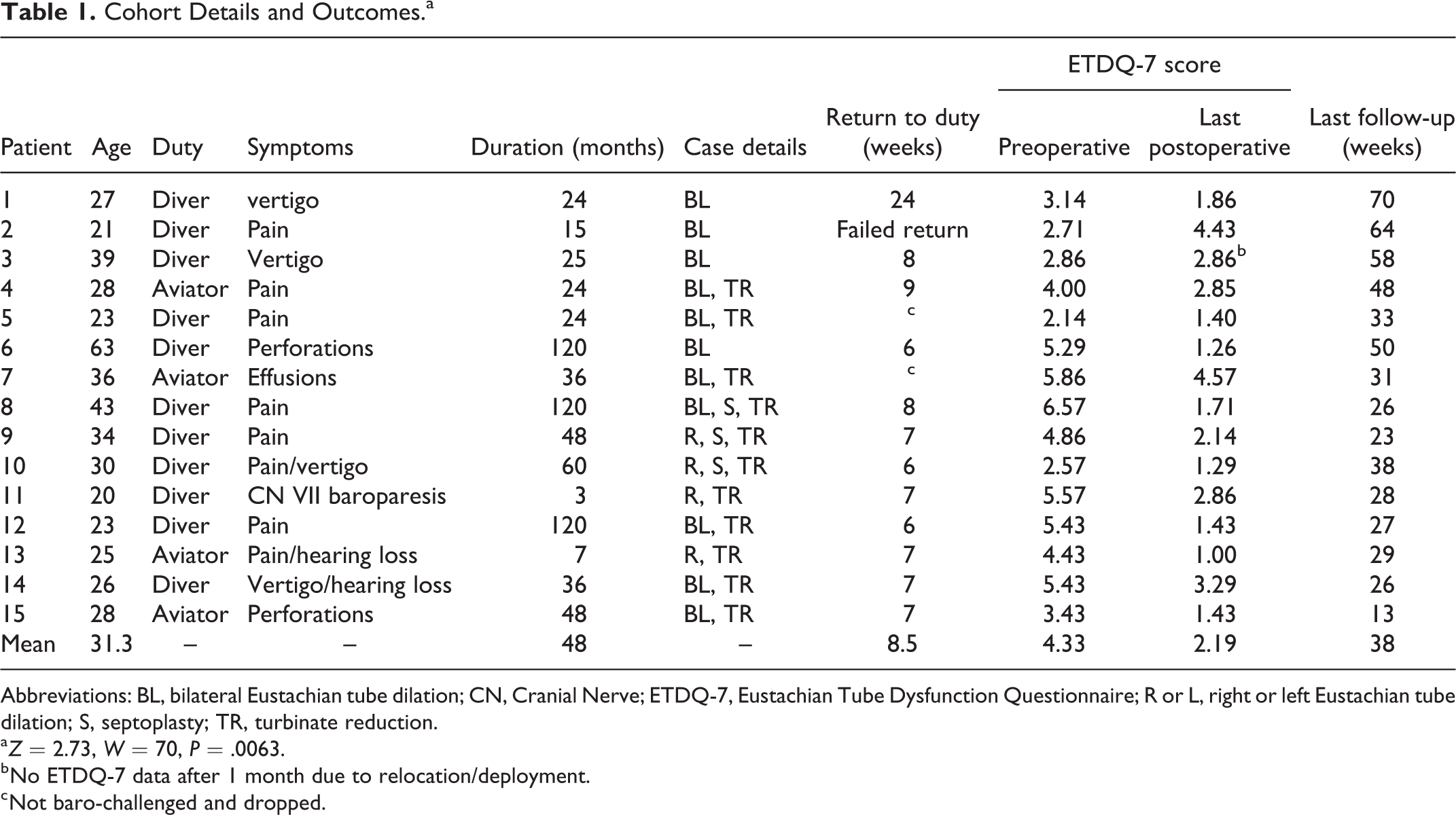
Abbreviations: BL, bilateral Eustachian tube dilation; CN, Cranial Nerve; ETDQ-7, Eustachian Tube Dysfunction Questionnaire; R or L, right or left Eustachian tube dilation; S, septoplasty; TR, turbinate reduction.
a Z = 2.73, W = 70, P = .0063.
b No ETDQ-7 data after 1 month due to relocation/deployment.
c Not baro-challenged and dropped.
Four subjects had a distant history of myringotomy with tympanostomy tube placement as infants, one with a concurrent adenoidectomy, but none had otherwise undergone any other head or neck surgery. All patients were nonsmokers. None reported a history of significant head trauma. No patients reported symptoms suggestive of gastroesophageal or laryngopharyngeal reflux, and none presented with symptoms or signs congruent with chronic rhinosinusitis. All patients denied any significant allergy history, but 7 patients exhibited evidence of occult allergies via allergy testing. All 15 patients exhibited at least a grade 2 inflammation on the ETMIS rating, indicative of mildly inflamed mucosa at the Eustachian tube orifice and torus tubarius, with no gross compromise of dilation of the cartilaginous Eustachian tube. All patients exhibited normal otoscopy and tympanometry on pretreatment evaluation.
Twenty-two Eustachian tubes, corresponding to unilateral or bilateral symptoms in 13 patients, underwent BET. There were no noted intraoperative or postoperative complications following treatment. Two patients required a very limited septoplasty to remove obstructing septal spurs for improved endoscopic Eustachian tube access. Turbinate outfracture facilitated exposure in 9 of 15 patients. Mean duration of follow-up was 38 weeks (range: 13-70 weeks). Six patients successfully completed postdilation chamber tests. Six patients were not able to formally complete postdilation chamber tests but were nonetheless functionally successful in their ability to return to dive and flight operations with resolution of limiting symptoms postdilation and were included in the primary outcomes analysis. Two patients, 1 aviator and 1 diver, were excluded from the analysis due to failing to undergo a postdilation baro-challenge. The aviator (patient 7) was medically separated from the military before returning to duties consequent to other concurrent medical issues not felt to be related to his ETD. The excluded diver (patient 5) reported a subjective improvement in his ability to perform modified Valsalva, but as of the time of this writing, he had not returned to diving operations due to other duty obligations. Since we could not confirm postdilation performance in these 2 patients, we elected to remove them from the primary outcomes analysis.
Our oldest patient (63 years old) was actually a retired Navy veteran who was disqualified from military diving operations in his 40s while active duty but continued intermittently diving as a recreational diving instructor despite recurrent tympanic membrane perforations due to ETD. Following BET, he resumed full-time diving without limiting symptoms or recurrent perforations out to 50 weeks as of the time of this report. Because his job as an instructor involves hyperbaric exposure in essentially the same environment as an active military diver, we retained him in the cohort.
One patient (patient 2) reported no significant benefit from BET and ultimately failed his return to diving. He was still symptomatic at 64 weeks postdilation with an increase in his ETDQ-7 score from 2.71 to 4.43. Despite our recommendation of no baro-challenge until after 5 weeks postdilation, he reported attempting to dive after about 2 weeks. It is unclear if this early baro-challenge contributed to his ultimate failure.
Dilation of the Eustachian tube(s) was effective in returning 92% (12/13) of patients to duty in the hyper- or hypobaric environment, with an average return to duty time of 8.5 weeks. Due to relocation and deployments, we were unable to collect ETDQ-7 data on 1 of 13 patients past the 6-month postdilation period. Of the remaining patients, mean ETDQ-7 scores improved from an average of 4.33 (2.57-6.57) predilation to 2.19 (1.00-4.43) postdilation (Z = 2.73, W = 70, P = .0063). Seven out of 13 patients scored ≤2.00 on follow-up visits, which is considered normal. 17
There was no significant change observed with audiometry or tympanometry recordings. All tympanograms were normal “type A” for pre- and postdilation measurements and did not change. Pre- versus postdilation air and bone conduction pure-tone averages (500, 1000, 2000, 4000 Hz) were not significantly different (P > .05).
Discussion
Eustachian tube dysfunction can be classified into 3 categories: dilatory, baro-challenge-induced, and patulous. 4 As our understanding of middle ear disease and ETD increases, it is important to delineate types of dysfunction as we look at treatment results. While defined in the literature as a unique subtype, 4 the prevalence and the natural history of baro-challenge-induced ETD is lacking likely due to limited testing and low exposure of the general public to activities that produce rapid atmospheric pressure changes. For those with baro-challenge-induced ETD that do attempt diving or flying and find that they cannot tolerate the otologic symptoms, it is likely that many simply disengage from such activities leading to underreporting and thus an inaccurately low prevalence. One could therefore postulate that the natural history of this condition is one which becomes extinct due to avoidance.
The military population, specifically those working in the hyper- and hypobaric environments, is uniquely suited to provide data regarding baro-challenge-induced ETD. For example, Navy divers routinely perform hyperbaric challenge tests to determine their ability to equalize middle ear pressures prior to diving. The standard recompression chamber test required by all Navy divers consists of a baro-challenge equal to descending to a depth of 60 fsw at maximum descent and ascent rates of 75 fsw/min and 30 fsw/min, respectively. These “chamber dives” provide a regulated and uniform way to safely test Eustachian tube pressure equalization function in patients with ETD, and these same tests that flag an individual with baro-challenge-induced ETD can be used to track postprocedure health of the Eustachian tube as a functional metric. 18 Six of our patients were able to successfully complete postdilation chamber tests, whereas they were not able to functionally pass such testing prior to treatment. Six other patients, unable to formally participate in chamber dives consequent to logistical hurdles, were ultimately returned to ocean diving or aviation duties posttreatment based upon their real-world operational performance with resolution of their limiting otologic symptoms while working in austere environments involving marked ambient pressure fluctuations.
The contribution of limited septoplasty and turbinate outfracture to improvement in ETD in our patients is unclear. A handful of studies in the literature showed mixed to no benefit from nasal surgery for otologic symptoms related to dilatory ETD. 19 -25 Theoretically, surgical changes from spur removal and turbinate outfracture that reduce nasal airflow turbulence or increase cross-sectional area of the nasal passages should not have an effect on the ability to increase nasopharyngeal ambient pressure during Valsalva since the movement of higher pressure air is from the lungs against pinched nares and a closed mouth. Venting of higher middle ear pressure via dilation of the Eustachian tube via palatal muscles should similarly not be affected by small alterations in nasal septum and turbinate anatomy.
It should be recognized that although our study has revealed overall favorable results within a small subset of the military population, such findings may understandably not reflect expectations within a larger, similarly affected civilian community. Our cohort primarily consists of young male participants which, while representative of many navy divers and aviators, may lack the diversity needed to be considered generalizable to the public. More diverse patients are therefore needed in future research in assessing the effectiveness of BET for patients with baro-challenge-induced ETD. In addition, our cohort is relatively small and our inability to obtain ETDQ-7 data on all of the patients past the 6-month period certainly affected our outcomes.
Our surgical success rate of 92% with normalization of ETD symptoms is high compared to previous studies assessing BET for chronic non-baro-challenge ETD. 5 -10 This high rate of resolution may be due to a variety of factors. Rigorous prescreening of candidates for the dive and aviation communities effectively imparts a selection bias as those with any prior history of chronic ear disease or significant dilatory ETD are rendered medically disqualified from this type of military service. All of our patients at one point had a sustained period of normal Eustachian tube physiology which allowed them to be selected for and perform flight or dive duties prior to becoming symptomatic. Due to the occurrence of symptoms experienced only with military diving and high-performance flight operations in highly austere environments, we presume that our cohort’s baseline ETD was mild and only became apparent during high-pressure alterations where the patients “couldn’t keep up” by modified Valsalva or other maneuvers. We must also recognize that these populations are generally stereotyped as highly motivated and above average performers. Faced with the prospect of “permanent medical disqualification” for future dive or flight related duties, it may not be hard to conjecture that such individuals could skew posttreatment results, especially with reliance on self-reported outcome measures as in this study. That being said, it is worth noting that the average duration of baro-challenge-induced symptoms in this group of patients was 48 months. Although some were often able to “power through” their limiting symptoms, others were quite restricted and had consistently failed multiple chamber runs and performance checks for prolonged periods of time prior to referral for specialty consultation. Additionally, personal and unit safety are typically significant cultural priorities in these high-functioning communities, and individuals in these groups are usually rewarded for acknowledging personal limitations that could risk the lives or safety of themselves or their teammates. Such realities may argue against the prospect that our results may have been favorably skewed.
Conclusion
Eustachian tube balloon dilation appears to be a safe and highly effective treatment option for persistent baro-challenge-induced ETD in affected military divers and aviators who work in hyper- and hypobaric environments. Further study is needed to determine whether similar results can be achieved in more diverse and larger patient populations and to assess long-term effectiveness of treatment.
Footnotes
Authors’ Note
The authors are military service members. This work was prepared as part of our official duties. Title 17, U.S.C. §105 provides that copyright protection under this title is not available for any work of the US Government. Title 17, U.S.C., §101 defines a US Government work as a work prepared by a military service member or employee of the US Government as part of that person’s official duties. No funding was obtained for this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.