
Abstract
A lordotic curve of the cervical spine in the aged is a physiological curvature of the cervical spine. The swallowing disorder precipitated by lordosis of the cervical spine in the aged, the swallowing function and intervention were reported on. An 86-year-old woman complained of swallowing difficulty for a few months. A lordotic curve (physiological curvature) of the cervical spine was observed. In the neutral neck position, the cervical lordotic angle was 29° using the Cobb C2-C7 method. When the lordotic curve of the cervical spine was intentionally straightened, the lordotic angle became 0°, the laryngeal elevation changed from 0.5 times the height of a cervical vertebra to 1.75 times, the laryngeal elevation delay time changed from 0.5 seconds to 0.23, the percent laryngeal elevation changed from 50% to 72% and pharyngeal transit time changed from 0.83 seconds to 0.75. Lordosis of the cervical spine inhibited laryngeal elevation and influenced the swallowing function. In cases in which lordotic curvature of the cervical spine adversely influences the swallowing function in the aged, rehabilitation to manage the lordosis of the cervical spine is useful. For the purpose of effective intervention, not only diagnostic but also therapeutic videofluorographic examination of swallowing is very important.
Introduction
Cervical spine disorders which can precipitate swallowing difficulties or swallowing disorders are called cervicogenic dysphagia. Pathophysiology of the cervicogenic dysphagia includes changes in physiological curvature of the cervical spine, dysfunction of the cervical spine, degenerative changes (anterior osteophytes, osteoarthritis, osteochondrosis), inflammatory disease (rheumatic disease), diffuse idiopathic skeletal hyperostosis (Forestier disease), complications from cervical spine surgery, injuries, congenital malformations, and tumors.
Due to the complexity of swallowing processes in the aged, not only diseases but also adverse health and physiological conditions can influence swallowing functions. Lordotic curve of the cervical spine in the aged is a physiological curvature of the cervical spine. Since the cervical spine has close proximity to the oropharynx and esophagus, presence of any structural changes and functional dimensions adversely affecting the dimensions of the pharynx and cervical esophagus can possibly disturb the normal swallowing process, especially in the aged with physiological swallowing difficulties. The lordosis of the cervical spine is not a rare physiological structural change in the aged; therefore, assessment and treatment for physiological cervical lordosis should be more focused on in daily practice when treating swallowing disorders.
In the present case, the swallowing disorder precipitated by lordosis of the cervical spine in the aged, the swallowing function and intervention were reported.
Case Report
This study has been carried out in accordance with “The Code of Ethics of the World Medical Association (Declaration of Helsinki)” for experiments involving humans.
An 86-year-old Japanese woman complained of globus pharyngeus and swallowing difficulty for a few months. Any diseases such as cerebrovascular diseases or neck trauma that could possibly affect globus pharyngeus and swallowing were not observed.
Videolaryngoscopy
Salivary retention in the vallecula and bilateral piriform sinuses were observed. Bilateral vocal fold movement was good.
Plain Radiography of the Neck
Lordotic curve of the cervical spine (physiological curvature of the cervical spine) was observed. No other cervical spine disorders which could cause a swallowing disorder were observed.
Cervical Lordotic Angle and Angle Between Airway and Food Passage Way
Presence of lordosis (physiological curvature) of the cervical spine was determined as follows: On plain radiographs taken with the patient in the neutral neck position, lordosis was measured with the widely used Cobb C2-C7 method (Figure 1).1,2 Cervical lordotic angle α (α in Figure 1A) was measured by joining perpendiculars to lines drawn parallel to the lower end plates of C2 and C7. In cases in which cervical lordotic angle is greater than 10° are assessed as a lordosis of the cervical spine. 1
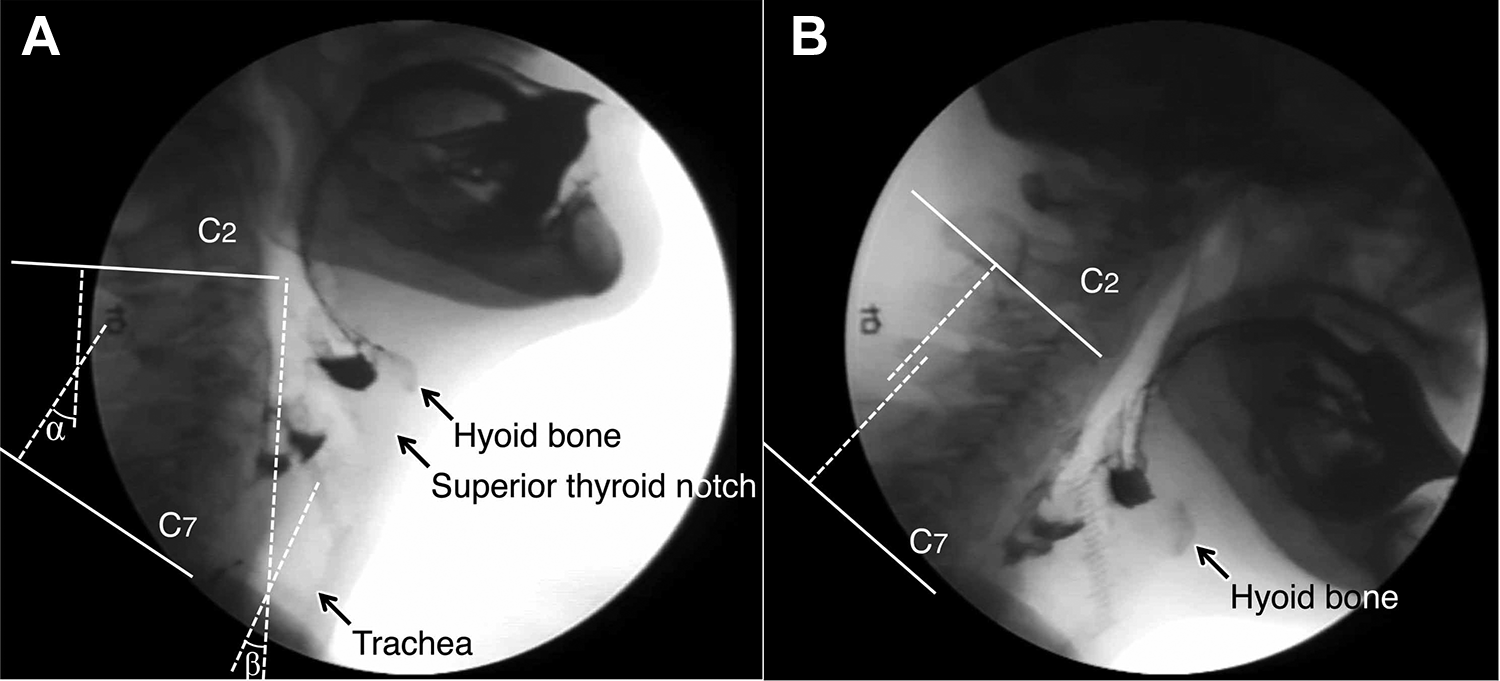
Measurement of sagittal alignment of the cervical spine (Cobb C2-C7 method) and angle between airway and food passage way. A, View in the neutral position, B, View when the lordotic curve of the cervical spine is intentionally straightened. α: cervical lordotic angle, β: angle between airway and food passage way.
In the neutral neck position, the cervical lordotic angle was 29°, resulting in a judgment of cervical lordosis (Figure 1A). When the lordotic curve of the cervical spine was intentionally straightened, the lordotic angle became 0° (Figure 1B).
Evaluation of the angle between the airway and food passage way was analyzed as follows: On plain radiographs taken with the patient in the neutral neck position, angle β (β in Figure 1A) between the airway and food passage way were measured by joining lines between a perpendiculars line drawn parallel to the lower end plate of C2 and a line parallel to the axis of the upper airway (larynx and trachea).
In the neutral position of the neck, the angle between the airway and food passage way was 24° (Figure 1A). When the lordotic curve of the cervical spine was intentionally straightened, this angle became 0° (Figure 1B).
Videofluorographic Examination of Swallowing and Swallowing Function Test
Barium sulfate (160 wt/vol%) was used as a contrast medium. The amount for each deglutition was 5 mL. Videofluorographic examination of swallowing revealed that the swallowing difficulty improved when the lordotic curve of the cervical spine (physiological curvature of the cervical spine) was intentionally straightened (see Figure 2).
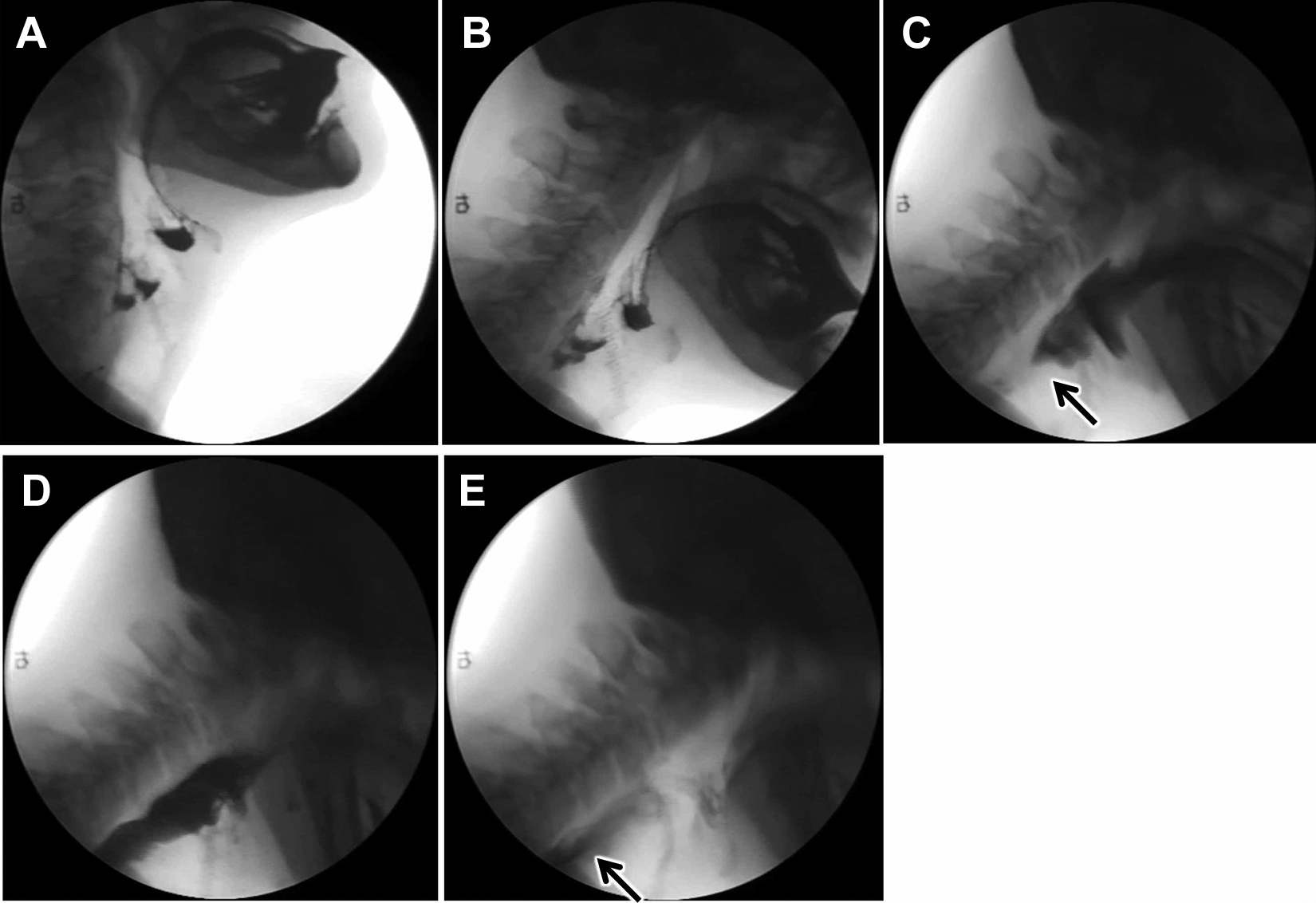
Videofluorographic examination of swallowing. Swallowing difficulty improved when the lordotic curve of the cervical spine was intentionally straightened. A, View in the neutral position, B, View when the lordotic curve of the cervical spine was intentionally straightened, C, Bolus head (arrow) arrived at the bottom of either side of the piriform sinus, D, Larynx elevated maximally, E, Bolus tail (arrow) reached the cricopharyngeal region.
Laryngeal elevation was measured by comparing the height of a cervical vertebra. Laryngoptosis, aspiration, and other swallowing disorders were also evaluated on videofluorogram.
Swallowing function was assessed using videofluorographic examination of swallowing. Laryngeal elevation delay time (the delay time from arrival of the bolus head at the bottom of either side of the piriform sinus until the maximum laryngeal elevation), Percent laryngeal elevation (the percentage of laryngeal elevation movement when the bolus head arrives at the bottom of either side of the piriform sinus) and pharyngeal transit time (the time from arrival of the bolus head at the bottom of either side of the piriform sinus until the bolus tail reachs the cricopharyngeal region) were measured on videofluorogram. 3
Comparison of Swallowing Function Between the Neutral Neck Position (With Lordosis) and the Intentionally Straightened Neck Position (Without Lordosis)
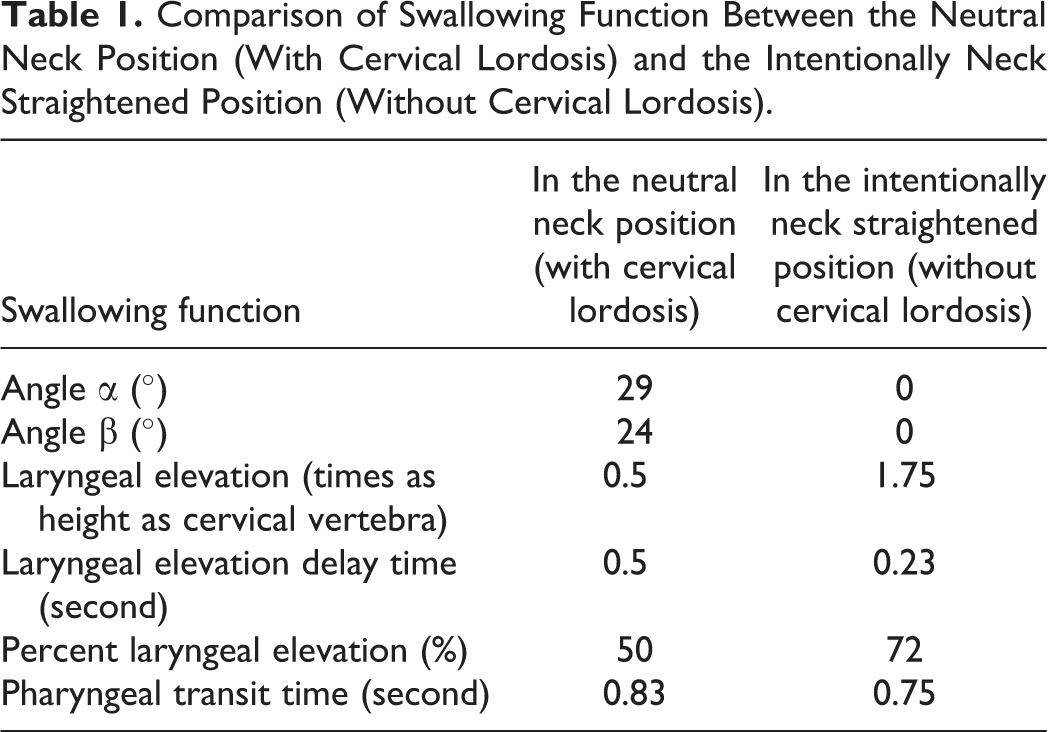
Laryngeal elevation was 0.5 times the height of a cervical vertebra in the neutral neck position. When the lordotic curve of the cervical spine was intentionally straightened, laryngeal elevation became 1.75 times the height of a cervical vertebra. Laryngeal elevation was inhibited by cervical lordosis and was improved when the lordotic curve of the cervical spine was intentionally straightened (Table 1).
Comparison of Swallowing Function Between the Neutral Neck Position (With Cervical Lordosis) and the Intentionally Neck Straightened Position (Without Cervical Lordosis).
The level of the hyoid bone was C3 in the neutral position of the neck. When the lordotic curve of the cervical spine was intentionally straightened, the level of the hyoid bone became C4. Laryngoptosis appeared when the lordotic curve of the cervical spine was intentionally straightened.
Aspiration and laryngeal penetration were not observed in either the neutral neck position or the intentionally straightened neck position.
Laryngeal elevation delay time was 0.5 seconds in the neutral neck position. The time shortened to 0.23 seconds when the lordotic curve of the cervical spine was intentionally straightened.
The percent laryngeal elevation was 50% in the neutral neck position. The percentage increased to 72% when the lordotic curve of the cervical spine was intentionally straightened.
Pharyngeal transit time was 0.83 seconds in the neutral neck position. The time shortened to 0.75 seconds when the lordotic curve of the cervical spine was intentionally straightened.
Discussion
The lordosis of the cervical spine is a common physiological structural change in the aged. Furthermore, the cervicothoracic spinal curvature undergoes progressive change through the life span. 4 Consequently, assessment of physiological lordosis of the cervical spine should be required and its interventions are necessary in daily practice for swallowing disorders in the aged. This case study provides circumstantial evidence of an association between dysphagia and lordosis of the cervical spine in the aged.
Evaluation of Lordosis of the Cervical Spine
There are various methods to evaluate lordosis (physiological curvature) of the cervical spine. In the present case, lordosis was measured with the widely used Cobb C2-C7 method.1,2 On plain radiographs taken with the patient in the neutral neck position, cervical lordotic angle can be measured by joining perpendiculars to lines drawn parallel to the lower end plates of C2 and C7. Greater than 10°, 0° to 10°, and less than 0° are judged as lordotic, straight, and kyphotic, respectively. 1
Evaluation of Angle Between Airway and Food Passage Way
In the present case, the angle between the airway and food passage way was measured. On plain radiographs taken with the patient in the neutral neck position, the angle between the airway and food passage way was measured by joining lines between a perpendicular line drawn parallel to the lower end plate of C2 and a line parallel to the axis of the upper airway (larynx and trachea).
In the neutral position of the neck, when lordosis (physiological curvature) of the cervical spine exists, the angle between the airway and food passage way increased. Consequently, both vectors cross resulting in adverse influence on aspiration. When the lordotic curve of the cervical spine is intentionally straightened, the angle between them decreases or becomes parallel. In this case, both vectors became approximately parallel resulting in a favorable influence on aspiration.
Swallowing Function Test
Since the cervical spine has close proximity to the oropharynx and esophagus, presence of lordosis (physiological curvature) of the cervical spine changes and functional dimensions adversely affecting the dimensions of the pharynx and cervical esophagus can possibly disturb the normal swallowing process, especially in the aged with physiological swallowing difficulties.
Previous reports showed that cervical lordosis precipitated dysphagia5,6; however, cervical lordosis is supposed to adversely affect the anatomical dimensional change in the pharynx and cervical esophagus resulting in dysphagia.
In the present case, the swallowing function was thoroughly investigated. Swallowing difficulty improved when the lordotic curve of the cervical spine was intentionally straightened. The most characteristic phenomenon was that lordosis of the cervical spine inhibited the laryngeal elevation during swallowing and influenced the swallowing function. When the lordotic curve of the cervical spine was intentionally straightened, the laryngeal elevation improved from 0.5 to 1.75 times the height of a cervical vertebra.
Shin reported that laryngeal elevation delay time is 0.243 ± 0.054 seconds, percent laryngeal elevation is 65.7% ± 12.6%, and pharyngeal transit time is 0.55 ± 0.126 seconds in normal Japanese adults. 3
In the present case, lordosis of the cervical spine increased the laryngeal elevation delay time, decreased the percent laryngeal elevation, and increased the pharyngeal transit time. When the lordotic curve of the cervical spine was intentionally straightened, the laryngeal elevation delay time and the percent laryngeal elevation became normalized. However, even though the pharyngeal transit time decreased, it did not become normalized.
Laxity of tissues surrounding the larynx and trachea leads to laryngoptosis, which is an abnormally low position of the larynx seen especially in the aged male and adversely influences the swallowing function.
In the present case, laryngoptosis was not observed when the patient was in the neutral neck position. However, laryngoptosis was observed when the lordotic curve of the cervical spine was intentionally straightened.
Intervention for Lordosis of the Cervical Spine in the Aged
The therapeutic options in aged patients with cervical lordosis precipitating dysphagia are few. Since the lordotic curve of the cervical spine in the aged is a physiological curvature of the cervical spine, intervention is not necessary when the aged has no symptoms. In cases in which lordotic curve of the cervical spine adversely influences the swallowing function in the aged, rehabilitation to manage the lordosis of the cervical spine is useful.
In the present case, videofluorographic examination of swallowing revealed that the laryngeal elevation during swallowing and dysphagia improved when the lordotic curve of the cervical spine was intentionally straightened. Improvements in the lordotic curve of the cervical spine and dysphagia are different in each patient. For the purpose of effective intervention, not only diagnostic but also therapeutic videofluorographic examination of swallowing is very important.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.