
Abstract
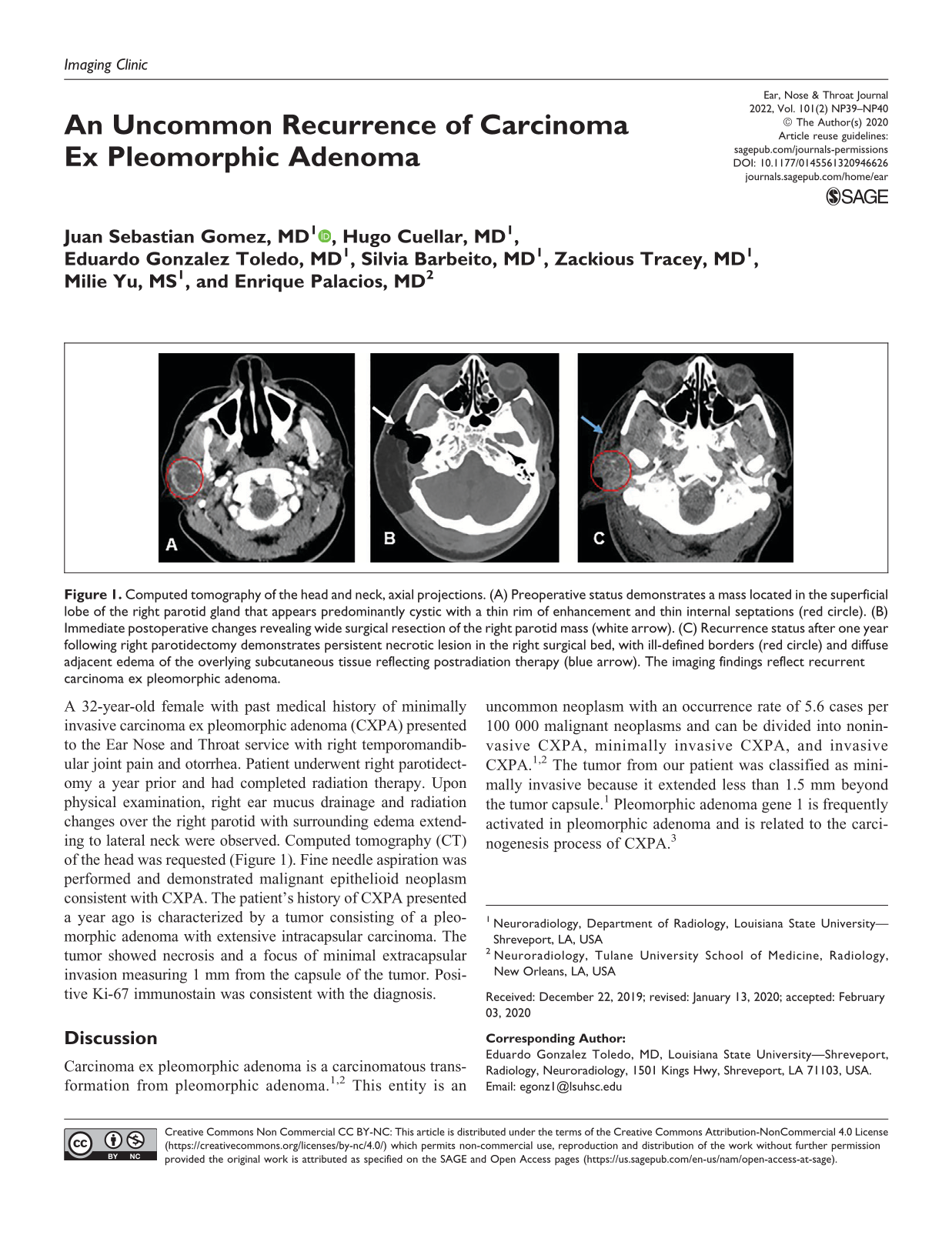
A 32-year-old female with past medical history of minimally invasive carcinoma ex pleomorphic adenoma (CXPA) presented to the Ear Nose and Throat service with right temporomandibular joint pain and otorrhea. Patient underwent right parotidectomy a year prior and had completed radiation therapy. Upon physical examination, right ear mucus drainage and radiation changes over the right parotid with surrounding edema extending to lateral neck were observed. Computed tomography (CT) of the head was requested (Figure 1). Fine needle aspiration was performed and demonstrated malignant epithelioid neoplasm consistent with CXPA. The patient’s history of CXPA presented a year ago is characterized by a tumor consisting of a pleomorphic adenoma with extensive intracapsular carcinoma. The tumor showed necrosis and a focus of minimal extracapsular invasion measuring 1 mm from the capsule of the tumor. Positive Ki-67 immunostain was consistent with the diagnosis.
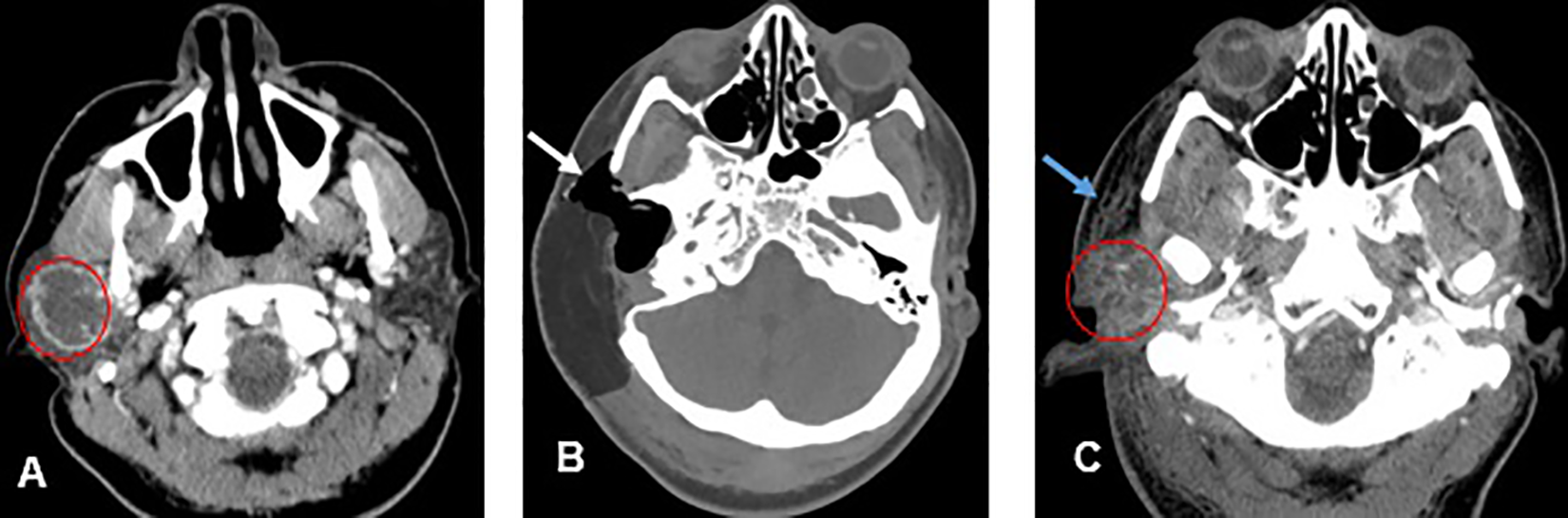
Computed tomography of the head and neck, axial projections. (A) Preoperative status demonstrates a mass located in the superficial lobe of the right parotid gland that appears predominantly cystic with a thin rim of enhancement and thin internal septations (red circle). (B) Immediate postoperative changes revealing wide surgical resection of the right parotid mass (white arrow). (C) Recurrence status after one year following right parotidectomy demonstrates persistent necrotic lesion in the right surgical bed, with ill-defined borders (red circle) and diffuse adjacent edema of the overlying subcutaneous tissue reflecting postradiation therapy (blue arrow). The imaging findings reflect recurrent carcinoma ex pleomorphic adenoma.
Discussion
Carcinoma ex pleomorphic adenoma is a carcinomatous transformation from pleomorphic adenoma.1,2 This entity is an uncommon neoplasm with an occurrence rate of 5.6 cases per 100 000 malignant neoplasms and can be divided into noninvasive CXPA, minimally invasive CXPA, and invasive CXPA.1,2 The tumor from our patient was classified as minimally invasive because it extended less than 1.5 mm beyond the tumor capsule. 1 Pleomorphic adenoma gene 1 is frequently activated in pleomorphic adenoma and is related to the carcinogenesis process of CXPA. 3
Preoperative diagnostic tests include fine needle aspiration cytology, CT, and magnetic resonance imaging. Magnetic resonance imaging findings of salivary gland tumors include an irregular tumor margin, heterogeneous intensity, tumor infiltration into surrounding tissue, and low signal intensity on T2-weighted images. 4 Positive immunostain with Ki-67 marker is correlated with high mitotic activity resulting in a high rate of cell proliferation in CXPA. 5
Treatment for CXPA involves surgical resection of the tumor plus radiation therapy. Superficial parotidectomy is used for intracapsular or minimally invasive CXPA localized to the superficial lobe of the parotid gland, while radical parotidectomy is indicated for invasive CXPA. Postoperative radiotherapy is used in certain cases such as high-grade carcinomatous components, questionable resection adequacy, and metastasis into lymph node and perineural invasion. 2 Patients treated with radiotherapy in combination with surgery demonstrated lower risk of recurrence in comparison to those treated with surgery alone. 1 Of note in our case, the patient underwent right parotidectomy and completed radiation therapy a year ago resulting in an uncommon case of recurrent CXPA.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.