
Abstract
Pulsatile tinnitus constitutes up to 10% of all tinnitus cases. Cerebral venous stenosis is a known etiology of pulsatile tinnitus. Treatment of pulsatile tinnitus secondary to venous stenosis with venous stenting has been reported in the literature but is not performed routinely. We would like to report a case of chronic pulsatile tinnitus treated with venous stent in a patient who previously underwent jugular vein ligation.
Keywords
Introduction
Pulsatile tinnitus (PT) is a form of tinnitus characterized by a synchronized pulse-like sound that is usually noted to be subjectively unilateral. 1 Tinnitus is a common condition affecting 1.2% of the population, 2 and PT constitutes 4% to 10% of all tinnitus cases.2,3 The etiology of PT is often vascular and can be classified based on its location as venous, arterial, or arteriovenous.3,4
The most common venous etiologies are transverse-sigmoid sinus stenosis with or without idiopathic intracranial hypertension (IIH), high jugular bulb,5,6 and sigmoid sinus diverticula or aneurysm (counting up to 20% of PT cases).3,7,8 Transverse sigmoid sinus junction stenosis is a common finding in IIH. Over the last 10 years, venous stenting has become an acceptable treatment option for IIH patients with transverse stenosis with or without tinnitus. Venous stenting for isolated PT has been reported but is not a well-established treatment.9-13
Ligation of jugular bulb as a treatment for PT is also not well established. There are publications available on this topic, some of which report poor outcomes and unpredictable complications.5,6,14 We present here an unusual case of a successful venous stenting as a treatment for chronic PT in a patient who previously underwent jugular vein ligation.
Case Presentation
A woman in her 20s with no significant medical history began suffering from a severe and debilitating PT in her right ear 3 years prior to presenting to our clinic. The patient described the tinnitus as partly alleviated during head tilting to the right or putting pressure on the right side of her neck and worsening while turning the head to the contralateral side. The patient denied headache, hearing loss, and other complaints. The tinnitus prevented proper sleep and was debilitating enough that she was unable to work.
As part of her work up, she underwent computed tomography (CT)/CT angiogram of the head and neck and magnetic resonance (MR) imaging/MR venogram (MV) of the brain and neck with no significant findings. After 2 years of multiple tests and multiple physician visits, the patient was referred to an Ear Nose and Throat (ENT) surgeon who suggested a right jugular vein ligation. The surgery was suggested to the patient due to her suffering and her insistence on trying every possible treatment. A high ride jugular bulb was suspected and therefore the indication for the treatment.
The patient underwent ligation of the right internal jugular vein as a management trial. Although no complications noted, the procedure failed to alleviate symptoms with no improvement to her preprocedural state.
A year later, the patient was referred to our clinic. After reviewing the MRV, we noticed a severe stenosis in both transverse sinuses, worse on the right, accompanied by occlusion of the right jugular vein secondary to her previous operation (Figure 1A). The patient was offered a diagnostic catheter-based venogram to explore the right transverse sinus stenosis as a reason for the tinnitus and potential stenting.
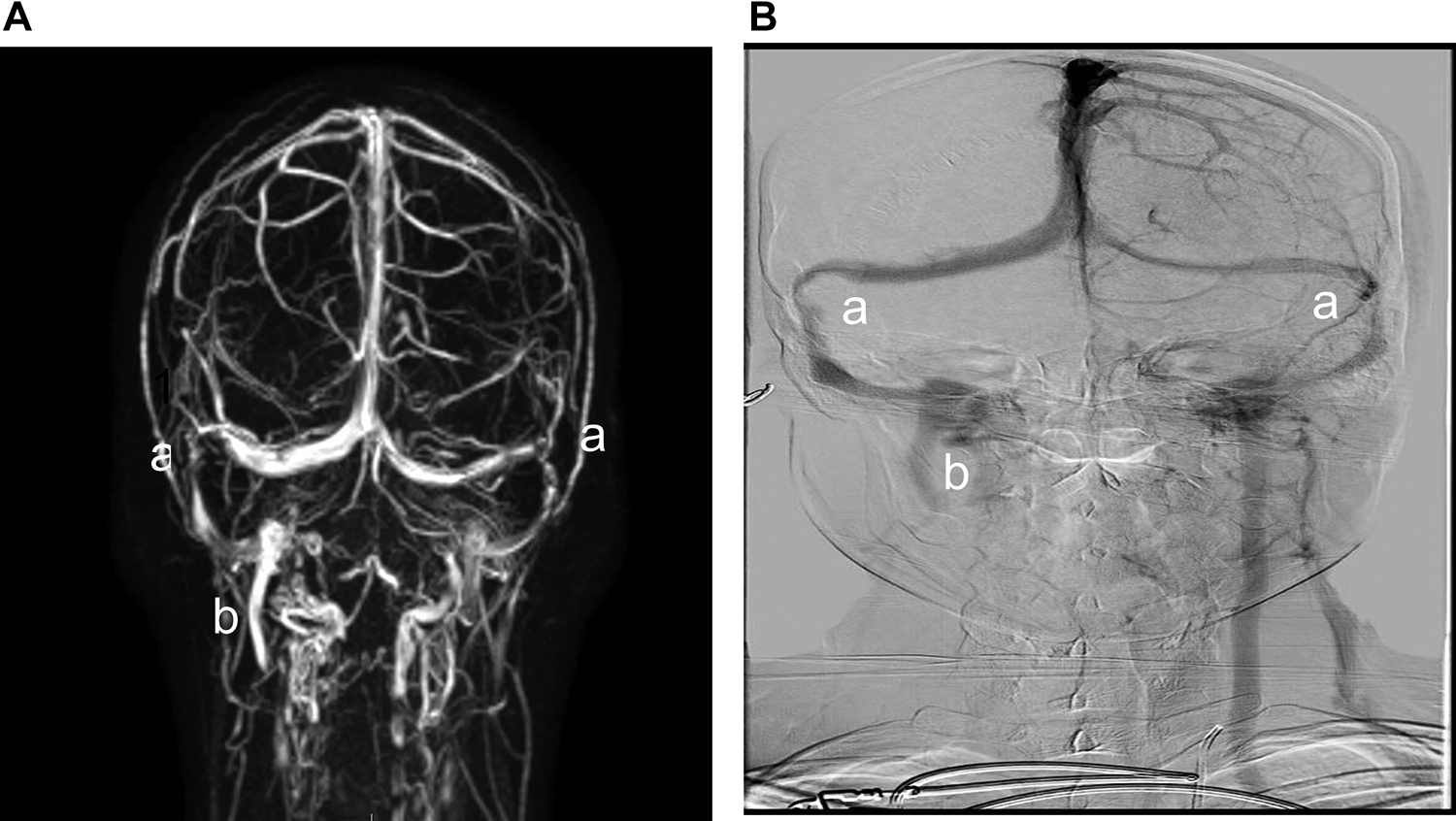
A, magnetic resonance venogram (MRV) showing bilateral transverse sigmoid sinus stenosis (more pronounced on the right) (a) with right jugular stump postprocedure (b) B, Similar finding are shown on venogram.
After taking 1 week of 100 mg Aspirin and 75 mg Plavix, the patient underwent catheterization. Two sheaths were placed, one in the femoral artery and the other in the femoral vein. During the procedure the patient was treated with heparin to keep activated clotting time (ACT ) over 250. A full diagnostic cerebral angiogram was performed in order to rule out other vascular etiology for PT. A run through the right carotid artery was kept in the venous phase in order to assist with venous navigation. This run showed similar findings to MRV (Figure 1B). Neuron MAX 6F (Penumbra Inc) was navigated to the left jugular over a 0.38 guidewire (Terumo IS, Terumo Medical Corporation) inside a vertebral diagnostic catheter 5F (Merit Medical Systems, Inc). Later, a Navien 0.72 (Covidien, Medtronic) was placed over Synchro 0.14 (Stryker Corporation) inside velocity microcatheter (Penumbra Inc) was used to cross the confluence of sinus to the right transverse side. An injection from the Navien demonstrated the exact location of the stenotic area (Figure 2). The velocity was then exchanged with an Aviator 7*40 balloon (Cordis, Cardinal Health) that was located in the stenotic area (Figure 3). Immediately after the balloon inflation, the patient reported a complete resolution of the tinnitus. When the balloon was deflated, she immediately reported a return of the tinnitus. Based on this response, we concluded that the patient would likely benefit from stenting. A Precise 40*7 (Cordis, Cardinal Health) was deployed over the stenotic area (Figure 4). Immediately after stenting, the patient reported complete resolution of the tinnitus. No poststenting angioplasty was performed. The patient remained in the hospital for 3 nights and was discharged home with no tinnitus or other complaints.
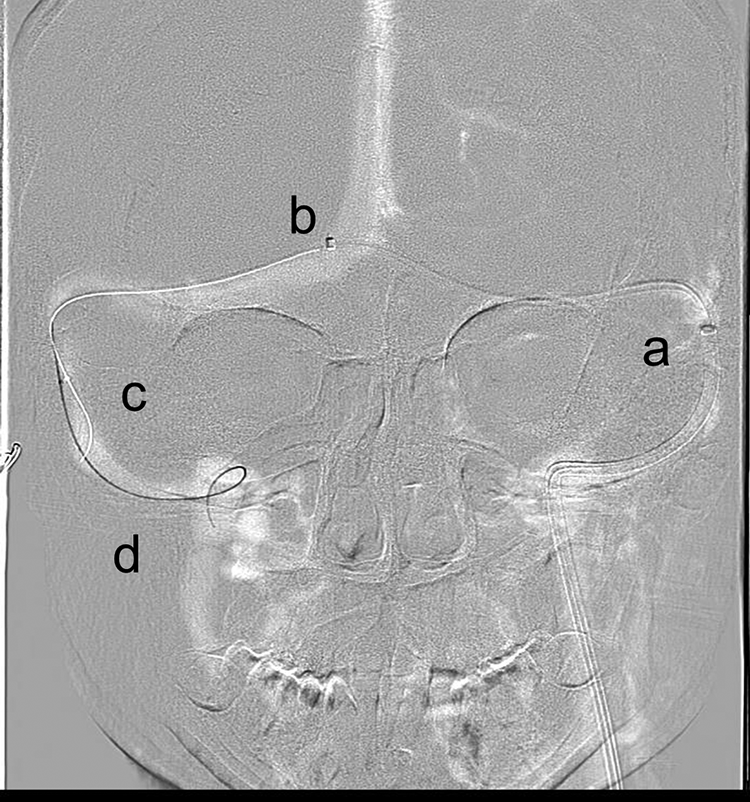
Neuronmax 90 cm positioned on the left sigmoid-jugular sinus (a). Navien 072 115 cm positioned on the right sigmoid sinus just across the confluence (b). Velocity microcatheter positioned across the stenosis on the right transverse-sigmoid junction (c). Synchro wire in the right jugular vein (d).
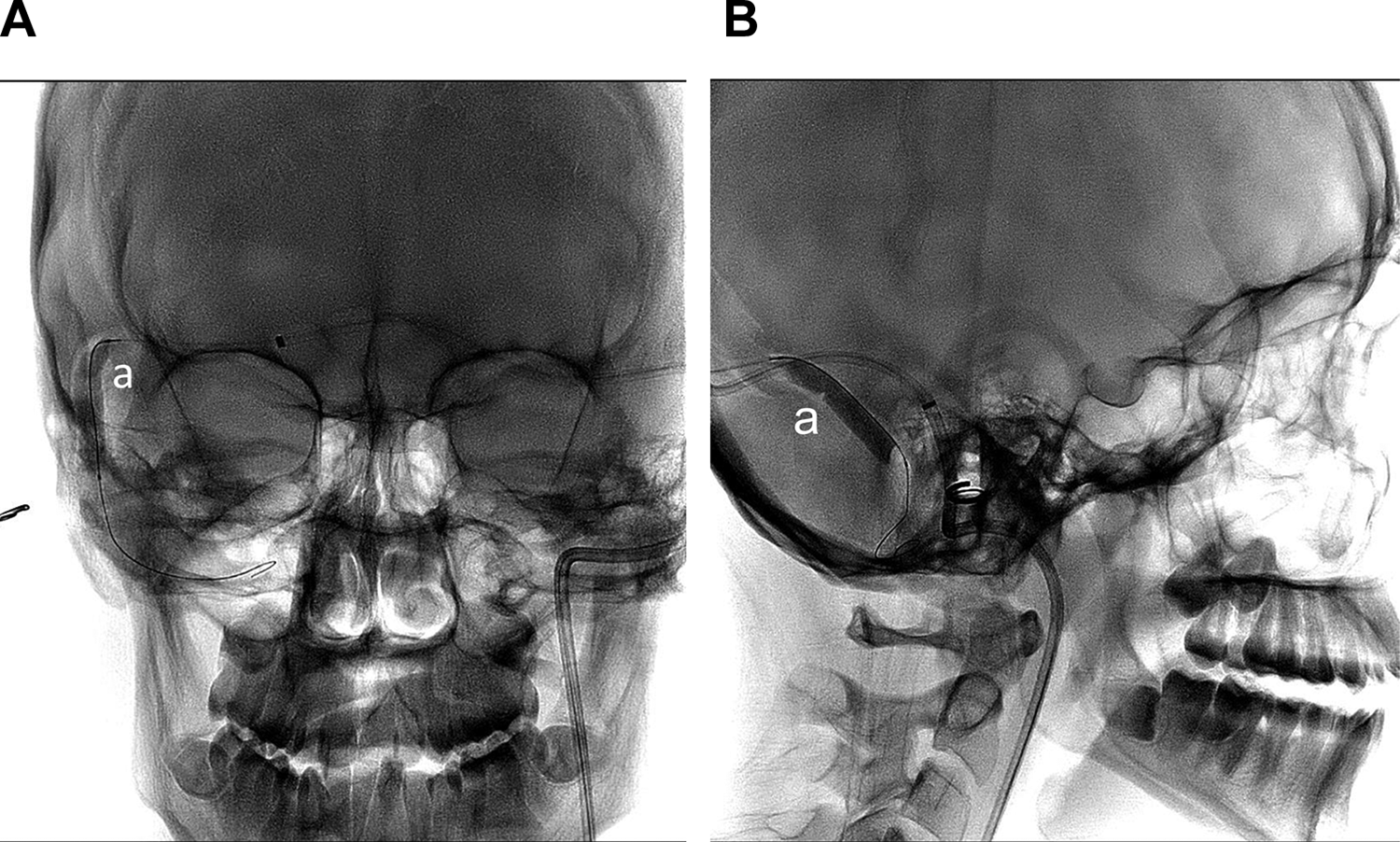
Flouroscopy of balloon inflated in the stenotic area (a) can be seen on AP (A) and lateral (B) views, complete resolution of the tinnitus reported by the patient after inflation.
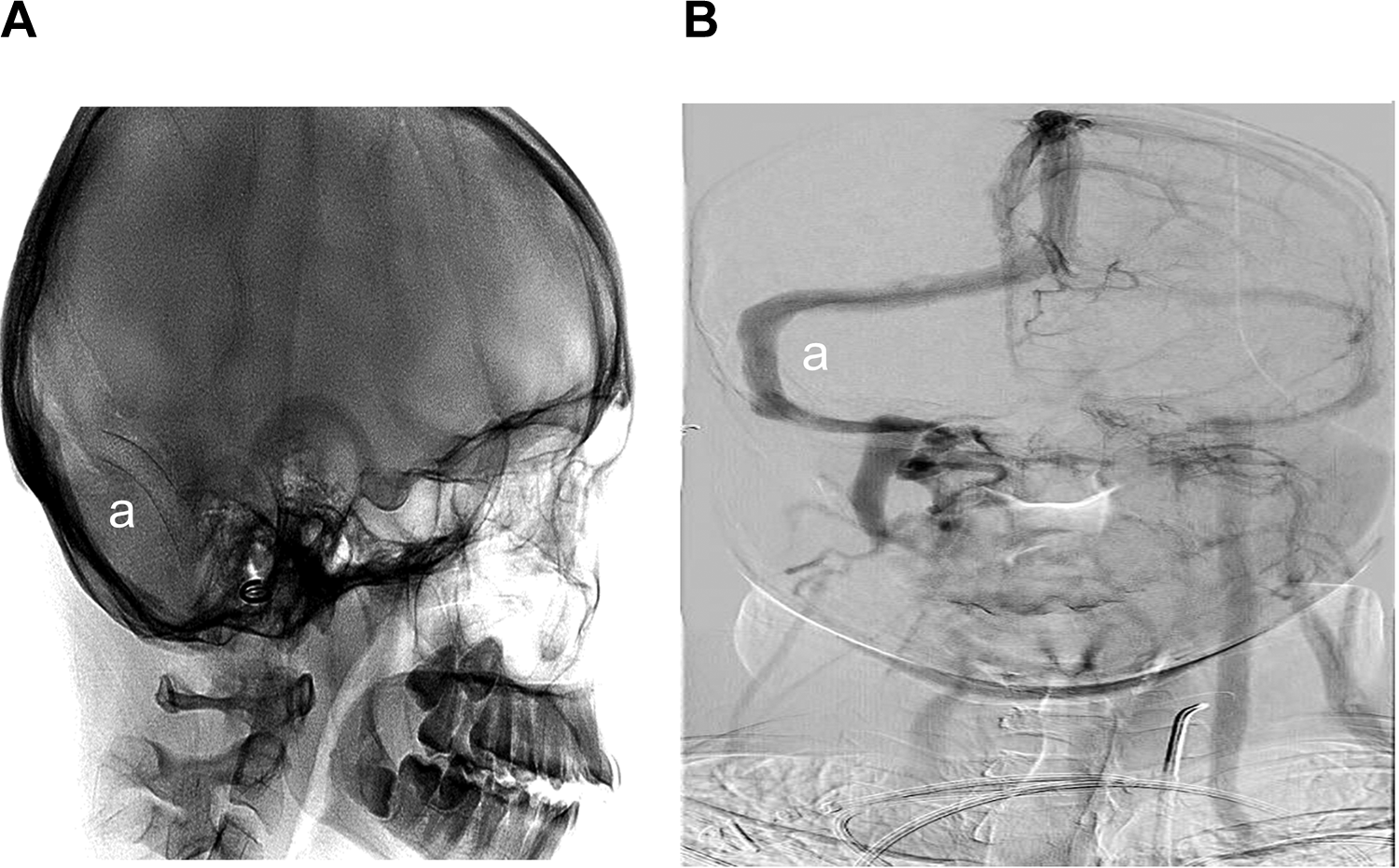
Poststenting the stent (a) is wide open on fluoroscopy (A). Resolution of stenosis post tenting on right carotid run showing the venous phase (B).
A follow-up visit was conducted 4 months later, and another follow-up was performed 1-year postprocedure. The patient reported complete resolution of the tinnitus with return to her previous quality of life. An MRV demonstrated normal laminar flow through the stent segment with ligated internal jugular vein. Treatment with Plavix was stopped 6 months postprocedure, and Aspirin treatment was continued.
Discussion
A few case reports, case series, and literature reviews have been published reporting high safety and good outcome of venous stenting in PT patients.4,7,10,13 Due to its subjective nature, PT is likely underdiagnosed and the diagnostic evaluation of patient with this symptom has proven to be challenging.15,16
It is also worth mentioning that the damage of tinnitus to quality of life can be significant. A clear association was found to moderate-severe depression (33%-41.2%) and severe anxiety (43.1%).5,6
We presented here a case of a young woman who suffered from debilitating PT with severe damage to her quality of life. The patient underwent stent deployment on the right transverse sigmoid junction from a left jugular approach since the right jugular was ligated on previous surgery. The patient reported a complete resolution of the tinnitus poststenting with a return to her previous quality of life. This case is further validation of venous stenting as a safe and effective treatment option for PT cases with ipsilateral transverse sinus stenosis.
Previous to transverse venous stenting, the patient underwent jugular ligation. Some publications describe poor outcome after this procedure,14,17 while others show excellent results.5,6 It is very likely that better patient selection for the procedure explains the differences in the reported outcomes. In our case, although a high jugular bulb was suspected, no consult with an interventional neuroradiologist prior to surgery was performed in order asses the intracranial venous status. In this case, the subtle high jugular bulb was not the explanation for the PT. A diagnostic angiography with venography prior to the ligation would have directed to the most probable etiology. A multidisciplinary team discussion (including radiology, ENT, interventional neuroradiology) prior to jugular ligation would likely have referred the patient directly to venous stenting and the patient could have avoided the unnecessary ligation.
It is likely that many patients with PT could benefit from venous stenting and that their quality of life could be improved significantly with the procedure. Since this condition is probably underdiagnosed, further studies are needed in order to better understand the prevalence of the condition and to improve the diagnostic and treatment options alongside awareness to the illness.
Conclusions
Pulsatile tinnitus is an underdiagnosed and understudied disease that may cause severe damage to the quality of life of many patients. Choosing the right treatment for patients suffering from PT may be challenging and, therefore, a multidisciplinary team discussion may prevent unnecessary procedures. Venous stenting is an effective and safe therapeutic option for selected patients suffering from PT due to venous stenosis. Large studies are needed to establish indications and treatment protocol for patients suffering from PT.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author received funding from a research fund.