
Abstract
Objective:
We retrospectively analyzed the laryngoscopy results and voice outcomes of patients with vocal polyps who received potassium titanyl phosphate (KTP) laser treatments in a clinician’s office, in order to establish the effectiveness and relative factors affecting the efficacy of this treatment.
Material and Methods:
We enrolled 25 patients with vocal polyps who had undergone KTP laser treatment in the Department of Otorhinolaryngology at our hospital between July 2017 and November 2019. Pre- and postoperative evaluations were measured using laryngovideostroboscopy (LVS), the Voice Handicap Index questionnaire (VHI-30), the GRBAS scale (G hoarseness, R roughness, B breathiness, A asthenia, S strain), and objective acoustic parameters. The reduction rate of lesions was calculated and relative factors affecting efficacy (size, side, location, the position of lesions, type, gender, and occupation) were tested.
Results:
Areas of lesions decreased from 101.95 ± 70.16 before surgery to 30.49 ± 35.80 after surgery (Z = 5.234, P < .001). The LVS data showed that the postoperative proportions of normal to mild conditions were the same or higher than the preoperative data in 3 instances: glottal closure (100% vs 100%), amplitude (90.91% vs 63.64%), and mucosal wave (81.82% vs 54.55%). A significant improvement was observed in VHI-30 scores, GRBAS scores, and acoustic parameters (P < .05). The size of lesions had an effect on the GRBAS scores (P < .001) but not on VHI-30 scores and objective acoustic parameters (P > .05). Other factors we tested did not affect voice outcomes.
Conclusion:
Potassium titanyl phosphate laser treatment can effectively reduce the lesion area of vocal polyps and improve the voice quality. The presence of small lesions seems to predict good subjective assessments of voice quality, but it remains to be seen whether this correlates with true voice quality.
Keywords
Introduction
Vocal fold polyps are a common type of laryngeal lesion that accounts for the majority of clinical voice disorders that interfere with everyday communication and affects the quality of life for the general population. 1 Hoarseness is usually the first symptom of this disease, and conservative management (voice rest and voice therapy) is recommended for all individuals. Removal of lesions under a microlaryngoscope is the primary surgical treatment for vocal polyps. With advancements in endoscopic and laser technologies, office-based laryngeal procedures are gradually being developed. Some of these have become a common strategy for treating vocal polyps in recent years. 2
A potassium titanyl phosphate (KTP) laser is a photoangiolytic laser with a 532 nm wavelength that can be selectively absorbed by oxyhemoglobin. Since Zeitels et al 3 reported its application in laryngeal surgery in 2006, KTP laser—which has demonstrated high patient tolerance and success rates—has emerged as a convenient, cost-effective, and time-saving way to treat laryngeal diseases. The effectiveness of KTP laser in the treatment of vocal polyps has also been investigated. Sheu et al 4 discovered that KTP laser caused significant reductions in the size of laryngeal lesions. Lin et al 5 also found that KTP laser offered significant improvements in patients with vocal polyps, whereas Sridharan et al 6 confirmed that KTP treatment of vocal fold polyps could be safely and successfully performed in a clinician’s office.
Potassium titanyl phosphate laser procedures have been used to treat vocal polyps in our department for several years. This study retrospectively analyzes the laryngoscopy results and voice outcomes for vocal polyp patients treated with KTP in order to examine the effectiveness of the treatment and explore the relative factors that affect efficacy.
Materials and Methods
Participants
The present study reviews 25 patients with vocal polyps who received in-office KTP laser treatments at the Department of Otorhinolaryngology at the Eye, Ear, Nose, and Throat (EENT) Hospital of Fudan University between July 2017 and November 2019. All participants were diagnosed by laryngovideostroboscopy (LVS) or laryngoscopy and their primary symptoms were hoarseness or dysphonia. Patients were fully informed of the recurrence, scarring, and other risks before surgery. Laryngoscopy, LVS, and acoustic assessments were performed for preoperative diagnosis and postoperative follow-up, depending on the patient’s willingness and the progression of their condition. Data on all subjects’ occupations were collected and classified into 3 groups, based on the level of vocal demand that occupation required. These groups were professional, high, and routine, as described in the previous literature. 7 Ethical approval was obtained from the institutional review board of the EENT Hospital.
In-Office KTP Laser Procedures
All KTP laser procedures were performed in a clinic under topical anesthesia administered via the nasal cavity, oropharynx, and larynx. During a KTP (532 nm; IDAS), the quartz fiber is carefully passed through the working channel of the therapeutic flexible laryngoscope (OLYMPUS CV-180; OLYMPUS), while the power is set at 6 W in a continuous wave output mode. The quasi-contact method was used for hemorrhagic polyps, whereas the contact method was primarily used for nonhemorrhagic polyps. Using the quasi-contact method, the fiber is as close as possible to the lesion surface but does not come into contact with it.
Morphological Examination
An LVS and rigid laryngoscopy were performed during postoperative follow-up. The LVS test was conducted by professional laryngoscopy physicians using the KayPentax 9100B apparatus. It was used to subjectively assess the degree of glottal closure, amplitude, and mucosal wave. Each of these factors was evaluated using a 4-level scale. For glottal closure, results were categorized as complete, small gap, moderate gap, or large gap; for amplitude, as normal, mildly, moderately, or severely diminished; and for mucosal wave as normal, mildly restricted, moderately restricted, or completely lacking.
We reviewed still photographs of the vocal fold abduction and used ImageJ software (National Institutes of Health) to circumscribe and quantify the lesion area in terms of pixels. Vocal fold length (from anterior commissure to vocal process) was quantified in pixels using the method described by Mallur et al, 8 and the lesion size was expressed as a ratio of lesion area to true vocal fold length, in order to eliminate variability based on the distance from the laryngoscope (Figure 1). The image was considered sufficient when the anterior commissure angle was greater than 40 degrees. Using this method, lesion size before and after treatment can be standardized as a ratio of lesion area to a fixed length. The lesion reduction rate was calculated using the following formula: reduction rate = (1 − post-lesion area/pre-lesion area) × 100%. The process was performed twice to verify reliability.
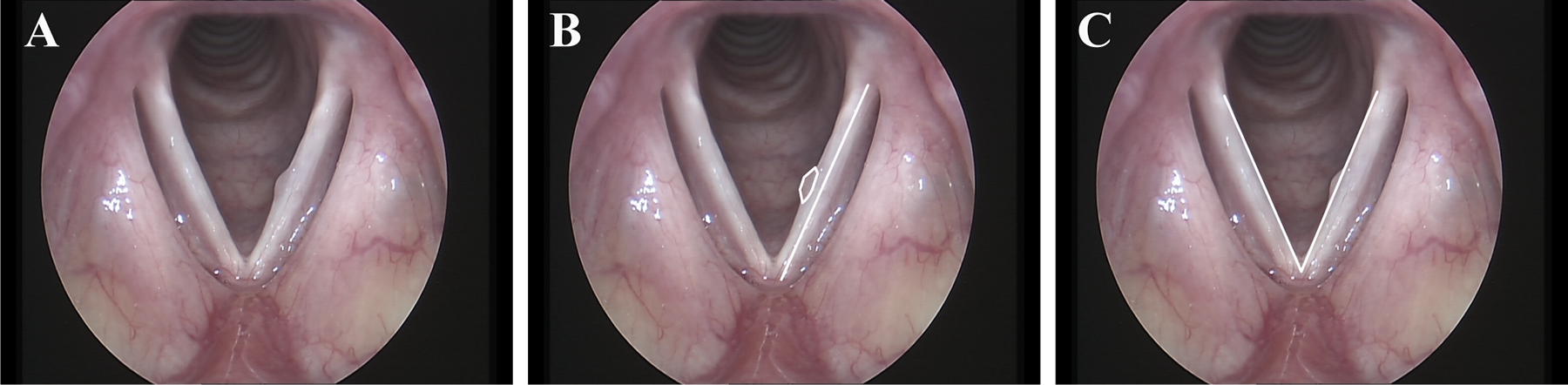
Measurement of vocal lesion size and anterior commissure angle. A, Image of left vocal fold polyp. B, Vocal fold length and lesion area was measured. C, Anterior commissure angle was measured.
The morphologic features were examined, including the type, side, size, location, and position of the lesions. Classification criteria were as follows: (a) side: unilateral or bilateral, left/right; (b) size: small (less than 1/4 of the length of the vocal fold), medium (1/4-1/3), or large (>1/3); (c) location: anterior 1/3, middle 1/3, or the posterior 1/3 of the vocal fold; (d) position: upper surface or free border of the vocal fold; and (e) type: nonhemorrhagic polyps or hemorrhagic polyps.
Measurement of Voice Outcomes
The Mandarin version of the Voice Handicap Index questionnaire (VHI-30) was composed of 30 items divided into 3 categories (function, emotion, and physiology), as described in detail in a previous paper by Xu et al. 9 There is a 5-level scale for each item (ranging from 0 to 4), which represents the subjective feelings of the patients. A total VHI score (ranging from 0 to 120) was calculated. Higher scores indicate higher degrees of voice impairment.
The GRBAS scale was also selected as a means of providing a subjective evaluation of the patients’ pronunciation in terms of 5 aspects: hoarseness (G), roughness (R), breathiness (B), asthenia (A), and strain (S). The patients were asked about their medical history in a soundproof room; then, they were required to answer and continuously produce phonation of an “a” vowel sound at a comfortable tone and volume so that it could be recorded. The 5 parameters were assessed on a 4-point scale (0, normal; 1, mildly abnormal; 2, moderate; and 3, severe) by 3 experienced phoniatrists who listened to the patients’ continuous vocalizations and short speech samples.
An objective acoustic analysis was performed using the multidimensional voice program with instruments produced by KayPentax CSL Company. A professionally mounted microphone (Dr. Voice Company) was used as the recording tool, positioned approximately 20 cm from the patient’s mouth as they sat in the soundproof room. Patients were instructed to pronounce an /α/ vowel for 3 seconds and the voice samples were input into the computer for analysis. Three acoustic parameters were calculated: average fundamental frequency (F0), fundamental frequency perturbation (jitter, J), and amplitude perturbation (shimmer, S). Maximal phonatory time (MPT) was also analyzed as an aerodynamic index. Each patient was asked to take a deep breath and pronounce an /α/ vowel for as long as possible at a regular pitch and loudness. This process was repeated 3 times and the longest sample was selected.
Assessment of Therapeutic Effect
The lesion reduction rate was calculated and we used ImageJ software to group the findings into 4 categories: “1” meant no change or an increased lesion range; “2” represented a decrease in lesion range of ≤50%; “3” meant a reduced lesion range of >50% but <100%; and “4” was complete lesion resolution (100%). The improvement rates in VHI and GRBAS scores were calculated using the following formula: improvement rate = (1 − post-scores/pre-scores) × 100%. The results were then ranked in 1 of 4 categories: “1” meant that the postoperative scores were unchanged or had increased; “2” represented postoperative scores that had decreased ≤50%; “3” referred to postoperative scores that decreased >50% but <100%; and “4” meant that all 3 patterns were completely normal. The 4 objective parameters were used to evaluate that patient in 1 of 2 categories: improvement or no improvement. Indicators that were closer to or within the normal range for before surgery were considered improvements.
Statistical Analysis
SPSS software (version 20.0) was used to compare the pre- and postoperative results. As quantitative data, the VHI scores, GRBAS scores, and acoustic parameters were quantitative data were tested using a Kolmogorov–Smirnov test for normality. A paired t test was used to evaluate whether data conformed to a normal distribution, whereas a Wilcoxon signed-rank test was used for data that did not conform to normal distribution. The results of the LVS, which were hierarchical data, were tested by the marginal homogeneity test. An ordinal logistic regression and binary logistic regression was performed to assess the relative factors affecting efficacy. A P value of less than .05 was considered statistically significant.
Results
Demographic Features
A total of 25 patients (3 male, 22 females; with a mean age of 45.26 ± 8.29 years and a range of 33-60 years) each received 1 KTP laser treatment. We followed up with all patients for an average of 6.04 ± 3.50 months (range: 3-14 months) after each operation. The patients’ occupations were classified as follows: professional (n = 1) and high demand (n = 24), which included sales staff, fruit and vegetable and other street vendors, singers, teachers, trainers, catering staff, psychological consultants, and so on. These patients either received no voice therapy or the effect of voice therapy before surgery had been poor. None of them underwent voice therapy between their surgery and the follow-up appointments they attended as part of this study.
Morphological Examination of Vocal Folds
Twenty-five patients underwent either LVS (n = 11) or rigid laryngoscopy (n = 14) both preoperatively and postoperatively. The lesion area was quantified using ImageJ and the results showed that these areas had decreased from 101.95 ± 70.16 before surgery to 30.49 ± 35.80 after surgery; these results were statistically significant (Z = 5.234, P < .001). After calculating the lesion reduction rate, it was found that 1 patient had an enlarged lesion; 7 patients had a certain degree of lesion reduction, but not more than 50%; 13 patients exhibited lesion reduction of more than 50% but less than 100%; and 4 patients had complete lesion disappearance (100%).
Eleven patients (1 male and 10 female) underwent LVS both preoperatively and postoperatively. When comparing the pre- and postoperative LVS data, we found that there was a higher number of normal and mild conditions postoperatively than preoperatively for the 3 factors that we examined (pre- and postoperative glottal closure, 100% vs 100%; amplitude, 63.64% vs 90.91%; mucosal wave, 54.55% vs 81.82%; Table 1). After analyzing efficacy in general, there was no significant difference in terms of glottal closure and amplitude (P > .05, Table 1); however, there was a statistically significant difference for mucosal wave (marginal homogeneity test = 2.000, P = .046, Table 1).
Comparison of Pre- and Postoperative Assessment of LVS Patterns.
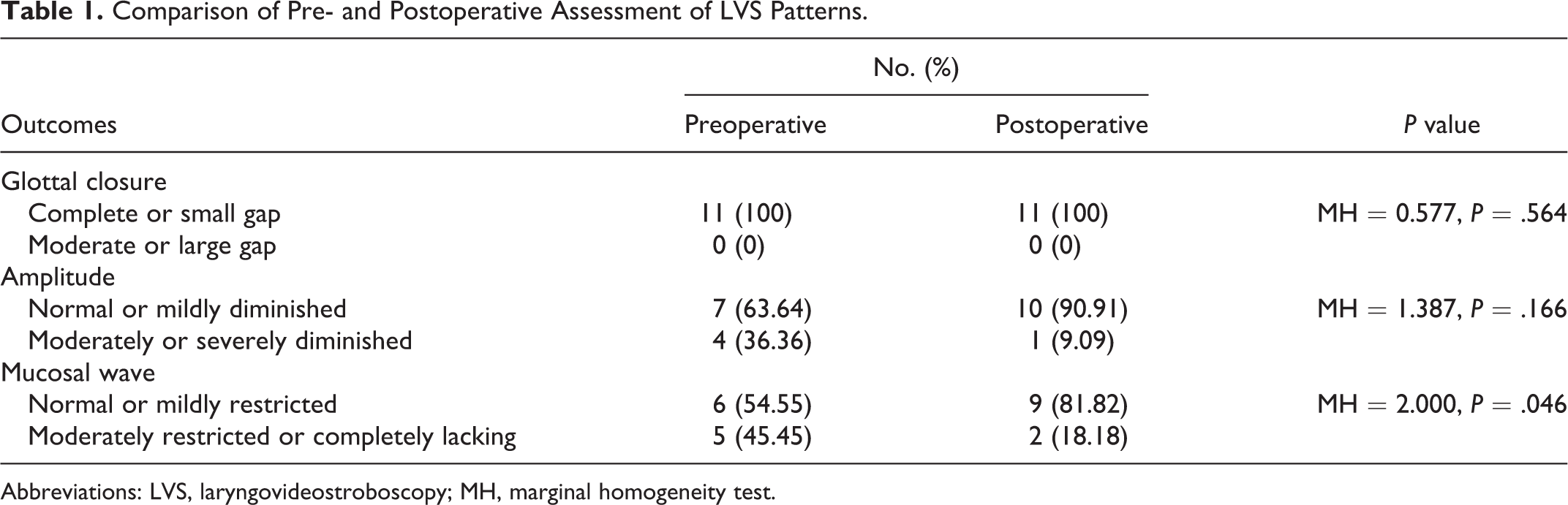
Abbreviations: LVS, laryngovideostroboscopy; MH, marginal homogeneity test.
Figure 2 includes some sample results. The main reason for patients to reject LVS treatment was that their symptoms had improved enough that they were unwilling to undergo another examination.
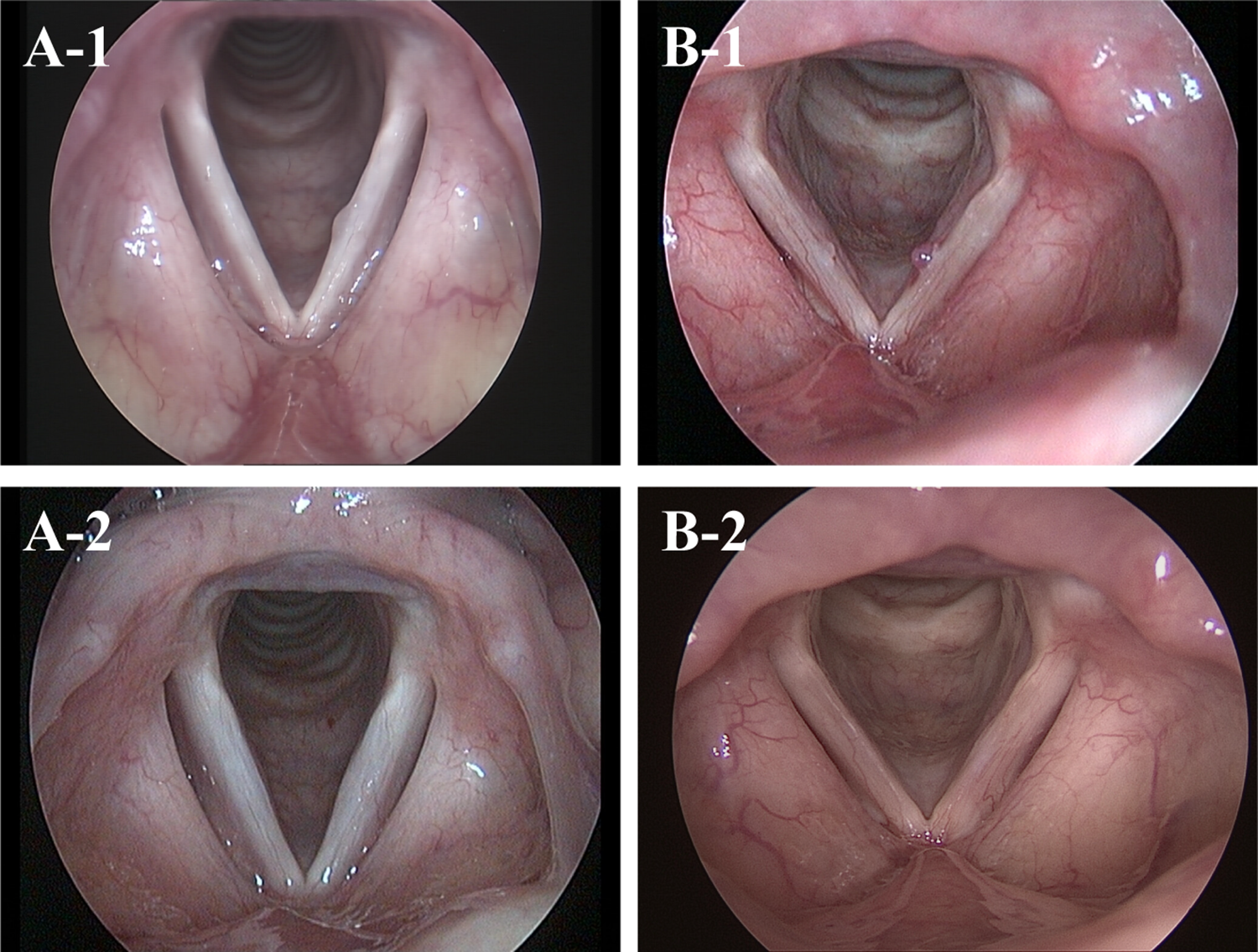
Comparison of pre- and postoperative laryngoscopy findings. A, Patient with non-hemorrhagic polyp. A-1 shows the preoperative lesion. A-2 shows the same area 10 months after KTP laser. B, Patient with hemorrhagic polyp. B-1 shows the preoperative lesion. B-2 shows the same area 4 months after KTP laser. The postoperative lesions of these patients had subsided significantly by comparison with the preoperative ones. KTP indicates potassium titanyl phosphate.
Voice Outcomes
Of the 25 patients who underwent KTP laser treatment, 16 (13 female and 3 males; a mean age of 43.63 ± 8.29 years with a range of 33-60 years) had complete sets of pre- and postoperative acoustic examination results; these 16 were included in our acoustic analysis. The mean follow-up time was 6.69 ± 3.84 months, with a range of 3 to 14 months.
The results of a pre- and postoperative VHI-30 score comparison showed that VHI-30 scores decreased from 45.94 ± 29.63 before the operation to 25.81 ± 20.93 after the operation (P = .030, Table 2). The physical and emotional scores were also lower than before (P < .05, Table 2), indicating that patients’ subjective perceptions of their voices had significantly improved after KTP treatment, even if their functional scores had not significantly changed (P > .05, Table 2).
Comparison of Pre- and Postoperative VHI-30 Scores, GRBAS Scores, and Acoustic Parameters.
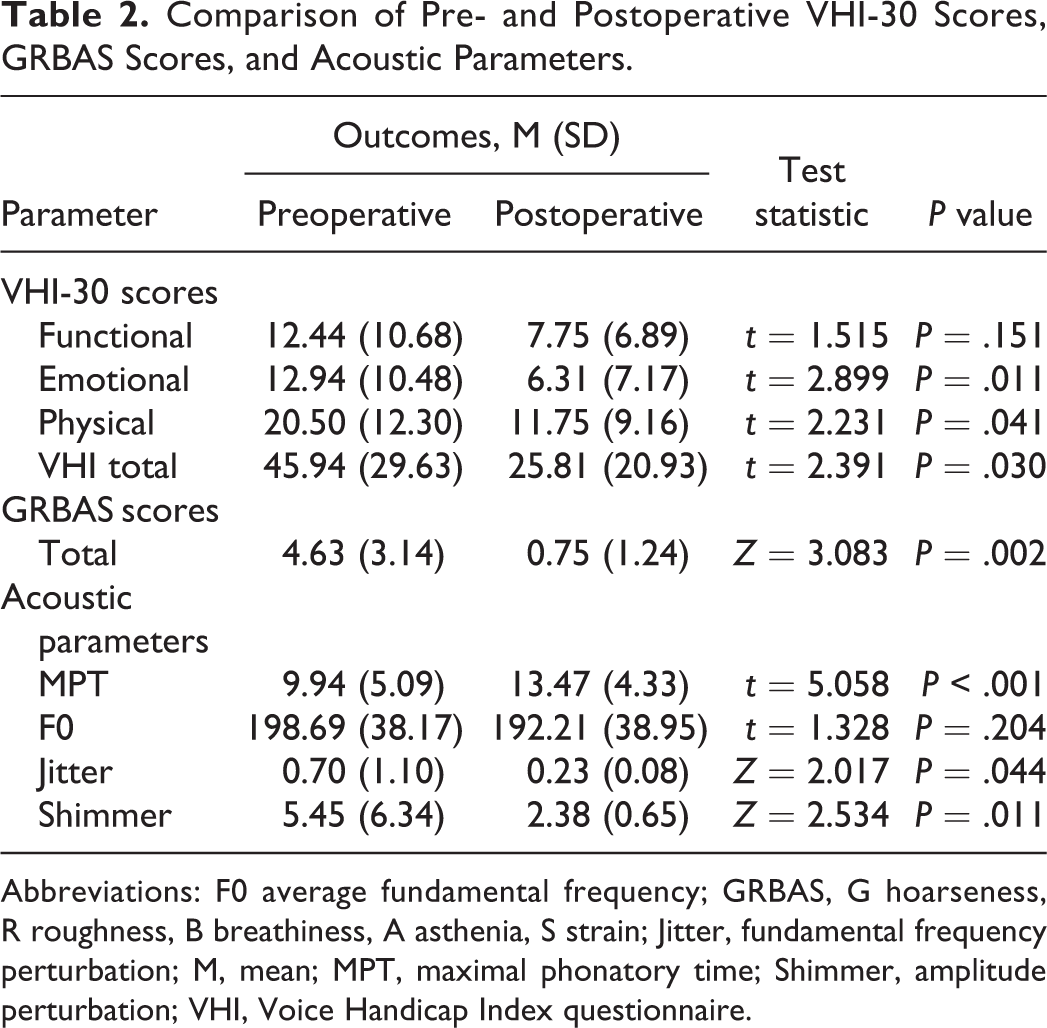
Abbreviations: F0 average fundamental frequency; GRBAS, G hoarseness, R roughness, B breathiness, A asthenia, S strain; Jitter, fundamental frequency perturbation; M, mean; MPT, maximal phonatory time; Shimmer, amplitude perturbation; VHI, Voice Handicap Index questionnaire.
The results of the GRBAS scale evaluation are presented in the form of total scores. When each patient’s “a” vowel vocalization was evaluated, we found that GRBAS scores were significantly lower postoperatively (0.75 ± 1.24) than preoperatively (4.63 ± 3.14) for total scores (P = .002, Table 2).
Our analysis of the objective acoustic parameters that were selected indicated that there were clear statistical improvements in Jitter and Shimmer (P < .05, Table 2) but not in F0 (P > .05, Table 2). Maximal phonatory time also significantly increased after the operation (pre vs post, 9.94 ± 5.09 vs 13.47 ± 4.33, P < .001, Table 2).
Analysis of Related Factors
Size, side, location, position, and lesion type, as well as patients’ gender, occupations, and lesion reduction rates, were examined to investigate the degree to which these factors affected voice quality. This was done using an ordinal logistic regression as well as a binary logistic regression. We found that lesion size had an effect on GRBAS scores (P < .001, Table 3) but not on VHI scores or other objective acoustic parameters (P > .05, Table 3). Other morphological characteristics (type, side, location, and position) and patients’ characteristics (gender and occupation) did not affect voice outcomes (P > .05, Table 3).
The Results of Regression Analysis of the Relative Factors Affecting Efficacy.
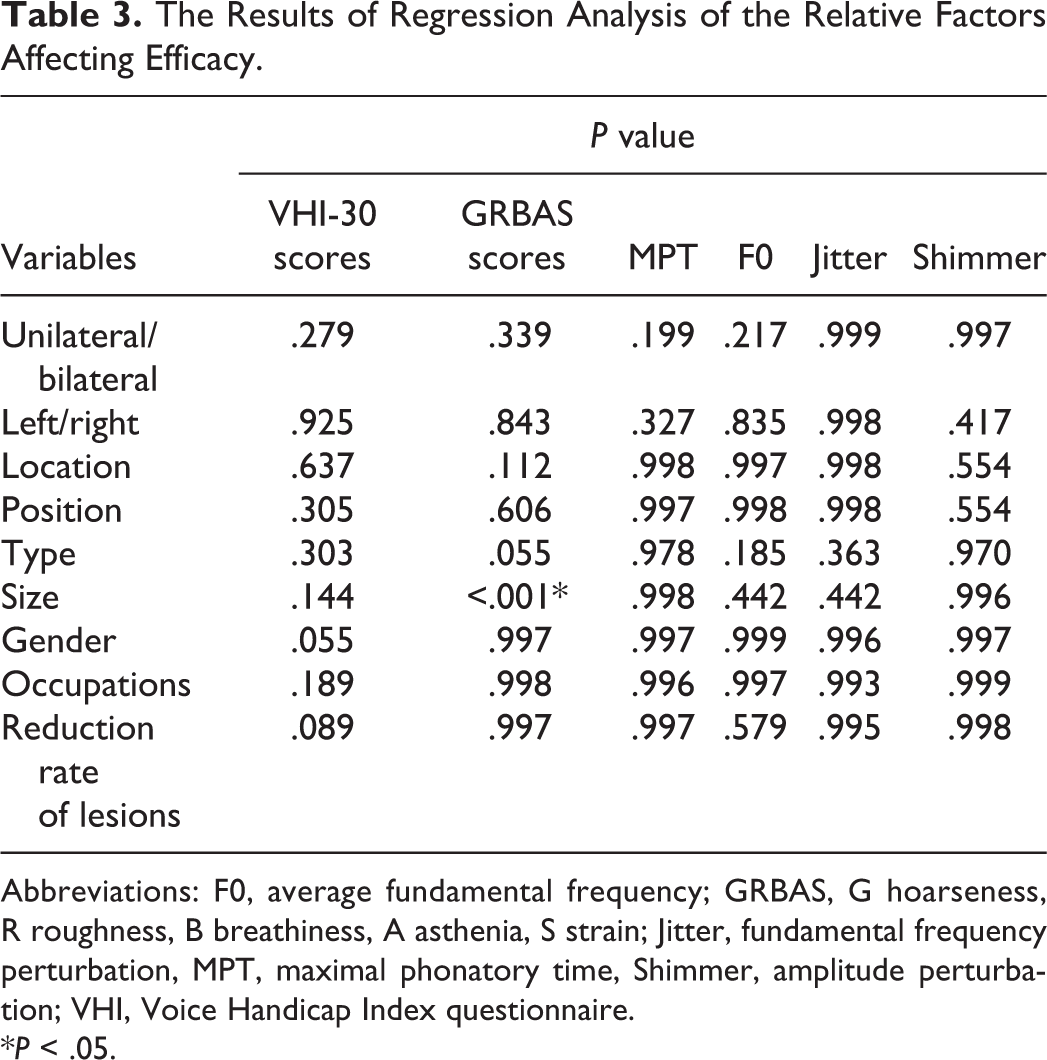
Abbreviations: F0, average fundamental frequency; GRBAS, G hoarseness, R roughness, B breathiness, A asthenia, S strain; Jitter, fundamental frequency perturbation, MPT, maximal phonatory time, Shimmer, amplitude perturbation; VHI, Voice Handicap Index questionnaire.
*P < .05.
Discussion
This study summarizes morphological examination and voice outcomes data for patients with vocal polyps who received KTP laser procedures, with the goal of investigating the therapeutic effect of KTP laser and related influencing factors. After a quantitative analysis of the lesion area, we found that KTP laser can effectively reduce lesions (pre vs post, 101.95 ± 70.16 vs 30.49 ± 35.80, Z = 5.234, P < .001). Subsequent acoustic measurements also found improvements in VHI and GRBAS scores, as well as objective parameters (P < .05, Table 2), indicating that KTP laser improved voice quality for patients with vocal polyps.
In this study, several examinations were selected to analyze the changes of pre- and postoperative conditions. Using the method described by Mallur et al, 8 we quantified total area of vocal fold lesions, which standardizes the pre- and postoperative size of lesions, and noted any reduction in lesion area (Figure 1). However, changes in the size of lesions do not necessarily reflect the state of the vocal folds; for this reason, we used LVS for further examination. This study found that 81.82% of patients had a normal or mildly restricted mucosal wave, a result which is similar to those in a previous study by Wang et al. 10 In addition, normal and mild degrees of glottal closure and amplitude were 100% and 90.91%, respectively (Table 1), revealing that KTP laser improved vocal fold morphology. However, there was no statistical significance in the overall analysis of postoperative differences (P > .05, Table 1). It is possible that more significant differences would be evident when using a larger sample size.
Voice outcomes were assessed using both subjective feelings and objective indicators. The VHI-30 and GRBAS scales were used to evaluate pronunciation disorder and its impact on the quality of life. Four parameters—3 acoustic and 1 aerodynamic—were selected as objective tests for voice outcomes. The results of VHI-30 scores, GRBAS scores, and acoustic parameters showed improvements after surgeries (P < .05, Table 2), supporting the effectiveness of KTP laser in the treatment of vocal polyps; however, F0 showed no change.
We also measured some factors that may influence voice quality. Though the lesion area decreased, this was not related to improvements in voice quality (P < .05, Table 3), indicating that a reduction in lesion area does not affect voice prognosis. Some literature has suggested that patients with small vocal polyps may have a much better chance of voice improvements after treatment. 11,12 Similar results were obtained in this study: lesion size on vocal folds had a significant effect on GRBAS scores (P < .001, Table 3). However, the size of lesions did not affect VHI-30 scores or objective acoustic parameters (P > .05, Table 3), indicating that small lesions seem to predict better subjective assessments of voice quality, even if it is not clear whether they also represent true voice quality. Akbari et al 13 found that patients with hemorrhagic polyps had higher levels of voice abnormality than those with nonhemorrhagic polyps. In our study, the type of polyp seems to have had no effect on voice outcomes after KTP procedures.
Which side of the vocal folds the lesion is on did make some difference, and we found that the lesions on the left vocal fold were processed more smoothly during the operations. With patients in the sitting position, the lesions on the left vocal fold were easier to deal with, while lesions on the right were more difficult to reach, given the angle of the flexible laryngoscope and the fact that the operator had to hold the scope with his left hand. Nevertheless, we found that the side the lesion was on had no significant effect on lesion clearance or voice quality, regardless of whether it was unilateral or bilateral, left or right (P > .05, Table 3). Furthermore, the location and position of lesions did not affect voice outcomes (P > .05, Table 3). In a finding that is inconsistent with previous studies, 14,15 the patient’s occupation seems to have had no effect on treatment efficacy, primarily because all subjects in our study were engaged in occupations with professional or significant voice requirements. This may indicate that there is no appreciable difference in voice prognosis between vocally high-demanding occupations and professional vocal occupations. The prevalence of voice disorders for females has been reported to be twice as high as that for males, and female patients seem to be a positive indicator for voice therapy. 16,17 However, gender did not affect vocal fold morphology or sound quality, according to our results (P > .05, Table 3). Larger sample sizes will be required to validate our results. Voice training was also recommended for patients who needed to correct pronunciation patterns after surgery. In order to exclude the influence of voice training from our results, we selected only patients who did not receive voice training during the follow-up period.
No adverse events or significant side effects were observed during patient follow-up. One limitation of this study is that it is retrospective in design, meaning that there are incomplete patient data and a small sample size. Some patients were not followed consistently or regularly. Since the follow-up time was short, further studies with longer follow-up periods are needed if we wish to observe long-term voice outcomes and monitor disease recurrence.
Conclusion
This study reveals that office-based KTP laser treatment can be an effective means of reducing vocal polyp lesion area and improving voice quality. The presence of small lesions seems to predict good subjective assessments of voice quality, but it remains to be seen whether this correlates with true voice quality.
Footnotes
Authors’ Note
Chunsheng Wei and Peijie He contributed equally as co-corresponding authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by (1) Science and Technology Commission of Shanghai Municipality (CN) [grant number 18411965600] and (2) Science and Technology Commission of Shanghai Municipality (CN) [grant number 19ZR1408100].