
Abstract
Introduction
Oropharyngeal papilloma is an exophytic and painless lesion with a pinkish white color that often develops in the tonsils, palate, uvula, tongue, and other locations. When they are small, most of them are asymptomatic, and patients discover them incidentally. As the lesion grows, symptoms, such as a foreign body sensation or dysphagia, develop. Surgical resection is the most common therapy, and papilloma is usually always easy to remove because of its superficial nature and the clear boundaries between papilloma and healthy tissue. Aside from cold steel surgery, the use of lasers has also been proposed for removing oropharyngeal papilloma.
A variety of laser procedures have been used to treat papilloma. Baeder et al 1 discovered that in comparison to electrocautery, high-power lasers promoted tissue evaporation, carbonization, and vaporization because of high temperatures, resulting in a significant reduction in viral load. Angiero et al 2 discovered that 95.74% of patients with oral papilloma showed complete healing in the first 30 days after treatment with an 810–980 nm diode laser, and the post-surgery pain was well tolerated. Remacle et al 3 also demonstrated the efficacy and reliability of a novel CO2 laser hollow fiber in the treatment of oropharyngeal papilloma.
Over the past decade, numerous studies have confirmed that office-based potassium-titanyl-phosphate (KTP) laser treatment of vocal fold polyps, 4 vocal recurrent respiratory papillomatosis, 5 vocal ectasia/varices, 6 vocal fold leukoplakia, 7 glottic carcinoma, 8 and other conditions is a safe, efficient, and cost-effective procedure. Multiple studies have demonstrated that the KTP laser is effective in treating recurrent respiratory papillomatosis in awake patients. 9 However, the therapeutic effect of the KTP laser on oropharyngeal papilloma should not be neglected. Kim et al 10 reviewed the demographic data and findings of 26 patients with oropharyngeal papillomatosis who had undergone an oral or oropharyngeal examination or a flexible laryngoscopy. Their findings supported the safety and efficacy of the KTP laser in detecting and removing most oropharyngeal papillomas. However, because the use of the KTP laser for oropharyngeal diseases has rarely been reported, there is little information available to assess its efficacy.
Several years ago, our department used the KTP laser to treat oropharyngeal diseases, such as oropharyngeal papilloma, polyps, and cysts, with papilloma being the most common lesion. This study compared the efficacy of KTP laser therapy to that of conventional cold steel surgery in the treatment of oropharyngeal papilloma, evaluating the operative duration, pain level, recovery, and recurrence to provide reference for clinical surgical modality selection.
Methods
Subjects
In this retrospective study, we enrolled patients with oropharyngeal lesions who visited the Department of Otorhinolaryngology at the Eye, Ear, Nose, and Throat Hospital of Fudan University and received in-office KTP laser or cold steel surgery treatment between 2017 and 2020. The main symptoms included pharyngeal foreign body sensation or incidental discovery of lesions. The purpose of the surgery was to remove and perform a biopsy on lesions. Patient charts were reviewed for demographic data (age and gender), pathology, anatomical location of lesions, and operative duration. All the patients were followed-up on for a while, and still photos obtained in the clinic were used to evaluate the postoperative residual lesions and their recurrence. Pain levels of the patients were assessed during and after treatment. This study was conducted under the Institutional Review Board of the Eye, Ear, Nose, and Throat Hospital.
Patients with oropharyngeal papilloma confirmed by pathology after surgery, patients with no abnormalities in the preoperative hematological examination (blood routine and coagulation function test), and patients who signed the written informed consent form were included in the study. Patients with uncontrolled diabetes or cardiovascular diseases, as well as those who were immunocompromised, had a bleeding tendency, or had coagulopathy, were excluded.
Surgical Procedures
All the patients were selected at random selection for treatment. Three doctors were assigned to the laser procedure and three to the cold steel surgery. Each surgeon had more than 5 years of experience in performing KTP laser treatment or cold steel surgery, and they followed the same procedure. When the patients came to our hospital, we did not provide them any subjective guidance; thus, the probability of them accessing the consulting room of each doctor was the same. Patients chose their doctors randomly and received KTP laser treatment or cold steel surgery. Before the operation, all patients were fully informed about the risks of bleeding, scarring, recurrence, and other complications. Thereafter, the informed consent was obtained. For office treatment, patients were seated in an examination chair. The oropharynx of each patient was anesthetized topically with three puffs of tetracaine 1% spray before the KTP laser or cold steel surgery treatment.
A quartz fiber was carefully passed through the working channel of the equipped handle in the KTP laser (532 nm) (IDAS, Erlangen, Germany), and a tongue depressor plate was used to expose the lesions. The parameter was set to 6 W in a continuous wave output mode. The base of the lesion was clamped with vascular forceps, and the lesion was pulled out about 1–2 mm away from the base (Figure 1). The entire soft tissue lesion was excised using a fiber-optic delivery system in contact mode. Since KTP laser has a good hemostatic effect at the same time of removing the lesion, the total time of the procedure was set as the time from the beginning of lesion resection to being allowed to leave by the doctor), and no additional postoperative observation time was required. Removal of uvula papilloma using a KTP laser. The lesion was removed about 1–2 mm away from the base to ensure complete resection. KTP, potassium-titanyl-phosphate.
The cold steel surgery was performed with vascular forceps, scissors, and tongue depressors. The tongue depressor was used to expose the lesions. The lesions were removed with scissors after the base was clamped with vascular forceps. To ensure that the incision was bleeding-free, a postoperative observation (about 20 min) in the consultation room was required in a designated observation area. Hemostasis measures were not performed routinely, but if the bleeding was severe, a cotton ball was used to stop the bleeding. The cold steel surgery procedure included lesion resection (from the beginning of the operation until the lesion was completely removed), intraoperative hemostasis (from lesion resection to leaving the operation area), and postoperative observation (from entering the observation area to being allowed to leave by the doctor).
HPV Genotyping
Human papillomavirus (HPV) detection and genotyping were performed using a 23 HPV genotyping real-time polymerase chain reaction kit (Hybribio, China), which can identify 17 high-risk HPV (HR-HPV) types (16, 18, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68, 73, and 82) and six low-risk HPV (LR-HPV) types (6, 11, 42, 43, 44, and 81).
Outcome Measurement
Based on the results of physical examinations by professional otolaryngologists in the clinic, regression and recurrence of diseases were measured, recorded, and analyzed. Still photos were retained to compare preoperative and postoperative lesions. Each patient was asked to rate their pain on a scale of 0–10 (0 for no pain and 10 for intolerable pain) on a visual analog scale. The pain level was evaluated immediately after surgery. Patients were asked about their pain level at 3 days and 1 month after surgery when they returned for a follow-up appointment after 1 month. Afterward, the patients were followed-up with clinic visits every 3 months for the first year, every 6 months for the second year, and every year thereafter.
Statistical Analysis
The SPSS software (version 20.0) was used for analysis in this study. The data were presented as mean (M) ± standard deviation values. The Mann–Whitney U test was used to compare the clinical charts of the two groups. A P-value of less than .05 was considered as statistically significant.
Results
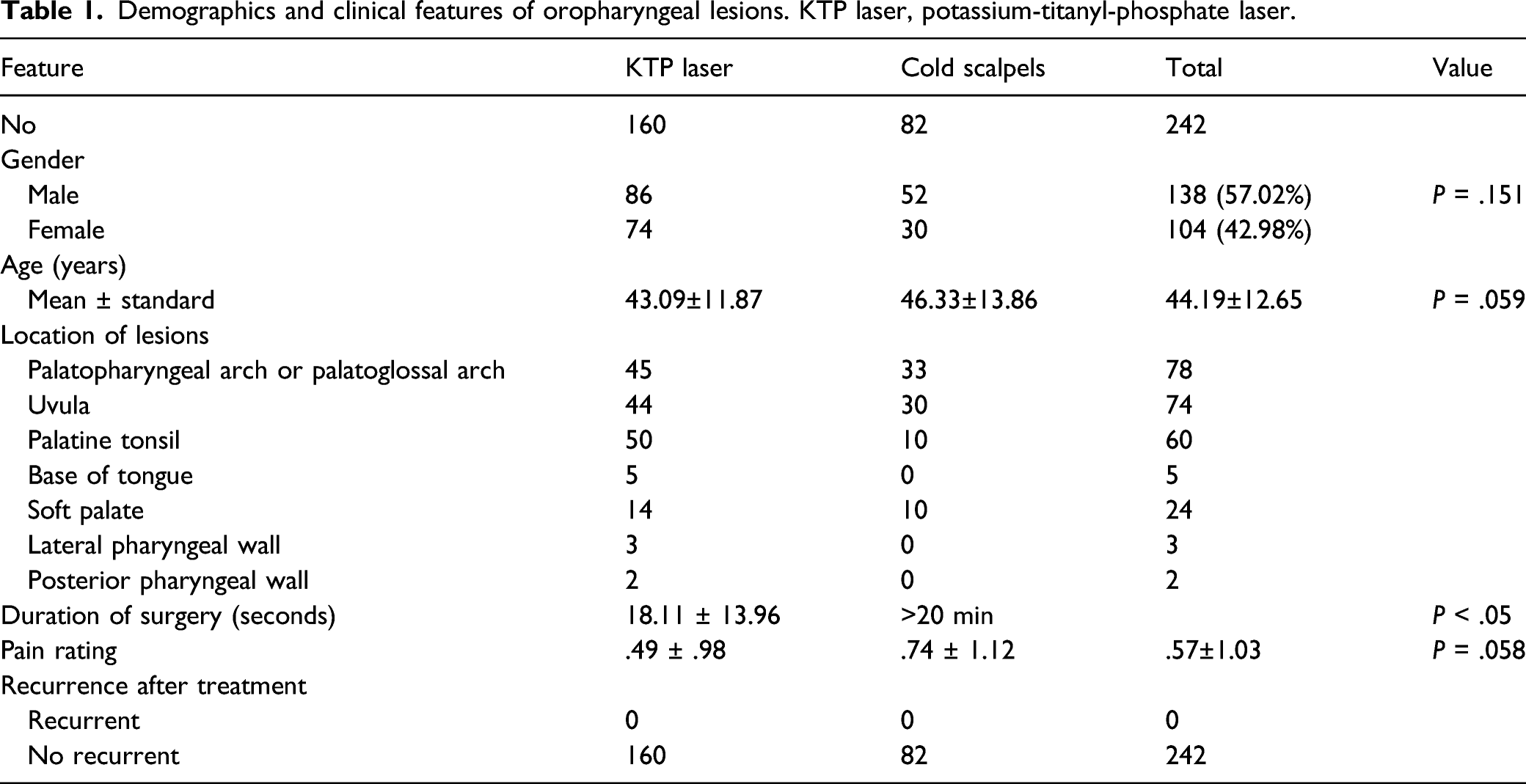
A review of the pathological reports of patients between December 2017 and October 2020 revealed that 242 cases were confirmed to be oropharyngeal papilloma cases. There were 138 men and 104 women, with an average age of 44.19 ± 12.65 (range = 13-78 y old). HPV testing was performed on the lesions of 25 patients, and the results revealed that two patients were positive for HPV strains, one of which was positive for both HPV 6 and 11 strains, and the other for HPV 16.
Demographics and clinical features of oropharyngeal lesions. KTP laser, potassium-titanyl-phosphate laser.

Comparison of pre- and postoperative palatopharyngeal papilloma. A, A 33-year-old male patient with papilloma in the palatopharyngeal arch (as shown by the white arrow) receiving KTP laser treatment. B, 1-month follow-up after the operation. C, 8-month follow-up after the operation.
There was no significant difference in the average time for lesion resection between KTP laser and cold steel group (18.11 ± 13.96 s vs 19.43 ± 16.91 s, P > .05). For the KTP laser procedure, intraoperative hemostasis took almost no time, and no additional postoperative observation time was set, allowing the patients to leave immediately without observation after the operation. Therefore, the effective total procedure time of the KTP laser has not been extended. In contrast, the operative duration of the cold steel surgery included not only the time for lesion resection but also the time of intraoperative hemostasis and postoperative observation because all patients who underwent cold steel surgery experienced bleeding during the operation. Further, 79 of the 82 patients who underwent cold steel surgery experienced minor bleeding (no more than one cotton ball infiltrate), which ceased spontaneously after 20 min of routine observation without any hemostasis measures. The other three cases required 4–5 cotton balls to compress the wound for hemostasis, which took 81.00 ± 17.09 s, and there was no further bleeding during the subsequent 20 min observation period. In these three patients, the total amount of bleeding was approximately 6–7 cotton ball infiltrates. Therefore, the total procedure time of cold steel surgery (>20 min) was significantly longer than that of the KTP laser procedure (18.11 ± 13.96 s). None of the 242 patients experienced unstoppable bleeding after being discharged from the hospital.
The mean pain rating immediately after KTP laser treatment was .49 ± .98, while that after cold steel surgery was .74 ± 1.12. On the third day following surgery, the pain rating of all patients dropped to 0, and none of them experienced any wound pain for at least 1 month of follow-up. There was no statistically significant difference between the pain ratings of the two groups (P = .058). The postoperative diet of all patients was not affected by the operation. Additionally, after a long period of follow-up (M = 15.35 ± 10.79 months; range = 6-39 months), no residual disease or recurrence was observed at the treatment sites.
Discussion
In this study, patients with oropharyngeal papilloma were treated with KTP laser or conventional cold steel surgery. Although both treatments could remove lesions quickly and effectively with good patient tolerance, the KTP laser offered better hemostasis.
In our department, traditional excision via cold steel surgery has been the main treatment for oropharyngeal papilloma for decades. Although it provides the advantages of simple operation and good effects, the inevitable bleeding that occurs after operation is an evident disadvantage. In addition to cold steel surgery, the KTP laser was also chosen for the treatment of oropharyngeal papilloma. The KTP laser is a photoangiolytic laser that can achieve surgical tissue effects, such as cutting, vaporization, and coagulation. 11 Since the wavelength of the KTP laser is close to the oxyhemoglobin absorption peak, it can produce a good thermal coagulation effect to target the microcirculation, making it an ideal tool for removing highly vascular lesions such as papilloma. In this study, KTP laser therapy offered a significant hemostasis advantage without postoperative observation, indicating that it is a safe and time-effective method for office-based treatment of oropharyngeal lesions.
Out of the 242 patients in this study, 238 had lesions in only one site, whereas four had lesions in two sites (two in the palatopharyngeal arch and tongue base, one in the uvula and palatine tonsils, and one in the uvula and soft palate). All patients underwent oropharyngeal anesthesia before operation to reduce pharyngeal reflex and to improve the operation success rate, particularly patients with lesions in the palatine tonsils or tongue base. The surgeon adjusted the position of the tongue depressor, and the patients were asked to hold the tongue depressor during the operation, cooperating with the surgeon to complete the operation. Most patients cooperated well, and their lesions were completely removed; however, one patient’s lesion in the tongue base was not removed because of its location and the patient’s nervous state.
In this study, a continuous mode was adopted in the treatment of oropharyngeal lesions to remove the tissue for biopsy. The base of the lesion was clamped with hemostatic forceps before the laser tip or cold steel was used for excision. The KTP laser procedure (18.11 ± 13.96 s) took less time than the cold steel surgery (>20 min) because intraoperative hemostasis and postoperative observation were not required. Removal of lesions on the tonsils appeared to take more time because the range of these lesions was not as evident as on the uvula; however, the total operative duration did not exceed 3 min. When the correct boundary plane was determined, the total resection time was no more than 10 s. Bleeding occurred in almost all patients who had cold steel surgery (n = 82), with 79 patients experiencing spontaneous hemostasis after 20 min and 3 patients requiring cotton ball compression to achieve hemostasis. There was no evidence of bleeding in the remaining patients, indicating that the KTP laser offers the advantage of preventing intraoperative bleeding. None of the patients experienced unstoppable bleeding after leaving the hospital, indicating that the chosen treatment method may not have an effect on the occurrence of postoperative bleeding.
Previous studies have reported good tolerance to pulsed dye lasers and CO2 lasers via flexible laryngoscopy.12,13 Kim et al 10 reported that KTP lasers were well tolerated under topical anesthesia in the treatment of incidental oropharyngeal papilloma. In this study, we used a pain tolerance scale of 0–10 (with 0 representing no pain and 10 representing intolerable pain) and found no statistical difference between the pain ratings of the KTP lasers and cold steel surgery groups (.49 ± .98 vs .74 ± 1.12, P > .05). However, the laser group appeared to have less pain, and increasing the sample size may result in positive results. Patients showed good tolerance to the KTP laser and cold steel surgery treatments for oropharyngeal papilloma, as postoperative pain was relieved within 3 days with no recurrence.
Oropharyngeal papilloma is mainly caused by HPV infection. In recent decades, epidemiological studies have reported a strong relationship between HPV and a subset of squamous cell carcinomas in the head and neck. 14 HPV is classified as LR-HPV or HR-HPV 15 based on its carcinogenic potential. Both can cause abnormal cell growth, but HR-HPV is usually associated with carcinoma. However, HPV is not detectable in all papilloma tissues. 10 In this study, the lesions in 25 patients were examined, and two patients were discovered to be HPV-positive. The progression from initial HPV infection to malignancy can take decades, and the papilloma may resolve on its own spontaneously. Unfortunately, we have no means of knowing which lesions will regress and which will develop into malignancy. Regular follow-up may aid in observing changes in the disease.
Oropharyngeal papilloma recurrence after resection is uncommon. A complete excision of lesions and HPV-infected cells is believed to be an important factor in preventing recurrence. 16 Nammour et al 17 recently reported that when a gross normal mucosa (≥3 mm) around the oral squamous papilloma was included in the resections, the lowest recurrence rate was observed. The good hemostasis effect of the KTP laser allows for a good surgical field of vision to be maintained during the operation, allowing the lesion boundary to be clearly distinguished and ensuring a safe boundary of 1–2 mm when the lesion is removed. It is difficult to completely excise and maintain the surgical margin via cold steel surgery because the resulting intraoperative bleeding obstructs the surgical field of vision. Therefore, it is important to determine the lesion boundary before cold steel surgery, and the operators may have to spend more time during the operation to ensure that the resection is complete, particularly when the lesion is located on the tonsil, where the boundary is difficult to discern. Thus, lesions excised by cold steel surgery appear to be more prone to recurrence than those excised with the KTP laser. However, no patient experienced recurrence, and there was no significant difference in recurrence between the use of laser and scalpel in our study, which is consistent with previous reports.17,18 To determine whether or not the two treatments would cause a difference in recurrence rates, larger sample sizes and longer follow-up times were required.
Although HPV status assessment of biopsied tissue may aid in the evaluation of disease prognosis, the limitation of this study is that not all tissues were tested for HPV. Furthermore, because this is a retrospective study, certain data were missing or could not be analyzed. Additional follow-up time is required to assess recurrence.
Conclusion
This study demonstrated that KTP laser therapy and cold steel surgery are safe, effective, and well-tolerated treatments for oropharyngeal papilloma. Although there was no significant difference in pain rating, incision recovery, and postoperative recurrence between the two methods, the KTP laser provided a better intraoperative hemostasis effect and a good surgical field of vision during the operation, allowing the operation to be completed in less time.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article..
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: 1. Science and Technology Commission of Shanghai Municipality (CN) (grant number: 19ZR1408100). 2. Science and Technology Commission of Shanghai Municipality (CN) (grant number: 18411965600)
Ethical approval
Ethical approval was obtained from the Institutional Review Board of the EENT Hospital.
Informed consent
Written consent was obtained from all the participants included in the study.