
Abstract
Pituitary carcinomas are rare tumors with only 170 cases reported in the literature.1 They form a very small proportion of pituitary tumors, which are commonly benign adenomas. Metastatic disease diagnosed by fine needle aspiration cytology is extremely rare and has only been reported in 6 patients,2-5 3 of whom had cervical nodal metastases, with other sites of metastases being the liver and cervical vertebra. We report a case of cervical metastatic pituitary carcinoma diagnosed by core needle biopsy.
Case Report
A 63-year-old female presented to the head and neck surgical clinic with a 2-month history of an asymptomatic left level II cervical nodal mass. She had a history of a left intracavernous pituitary somatotrophic adenoma, presenting with acromegaly in 2011. This was treated with surgical resection and postoperative radiotherapy. Residual disease was treated with the somatostatin analogue, lanreotide, and further recurrence required surgery and radiotherapy.
Core biopsy of the left level II mass demonstrated sheets of monotonous cells with mildly hyperchromatic nuclei and abundant eosinophilic and ill-defined cytoplasm. Ki-67 was 36.8% and immunostaining showed an absence of cytokeratins AE1/AE3 and of S100, with diffuse positive staining for chromogranin A and synaptophysin. The differential diagnoses included metastatic pituitary carcinoma, metastatic visceral neuroendocrine tumor, and paraganglioma. Given her prior history of recurrent pituitary adenoma and the lack of other radiological abnormalities on GaTate and fluorodeoxyglucose positron emission tomography (PET) scans, a diagnosis of metastatic pituitary carcinoma was made.
The patient underwent left level Ib, II, III, and Va neck dissection. Histopathology demonstrated a lymph node replaced by tumor cells arranged in sheets and vague nests with a delicate interwoven vasculature, and containing round to ovoid nuclei with granular chromatin and eosinophilic granular cytoplasm (Figure 1). Immunohistochemistry demonstrated diffuse and strong expression of synaptophysin (Figure 2A), succinate dehydrogenase (SDH) A, SDHB, and somatostatin receptor 2, with scattered tumor cells demonstrating growth hormone positivity (Figure 2B). Staining was negative for cytokeratin AE1/3 (Figure 2C). Ki67 was 31% (Figure 3). Nine additional lymph nodes in the ipsilateral neck showed evidence of metastatic pituitary carcinoma. The patient was reviewed at the head and neck multidisciplinary meeting with the plan to consider further radiotherapy and/or chemotherapy. Despite the paucity of evidence base, she was offered postoperative radiotherapy to the neck on the basis of first principles in the treatment of squamous cell carcinoma; she however declined radiotherapy and, 9 months later, developed progressive local disease of her pituitary tumor resulting in raised intracranial pressure, local involvement of cranial nerves II, III, V. At this stage, she underwent further extensive transsphenoidal surgical debulking. Postoperative imaging recently demonstrated distant metastases, and following discussion at neuroendocrine tumor board, she has been referred for peptide receptor radionuclide therapy due to commence shortly.
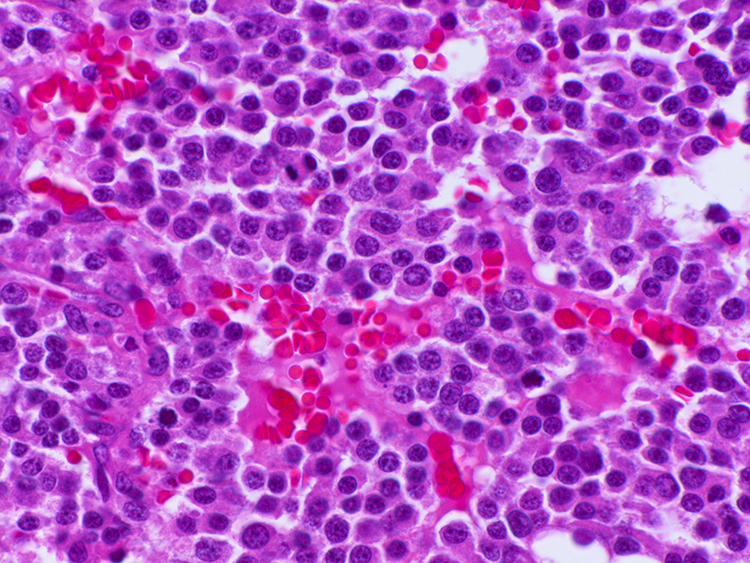
Hematoxylin and eosin staining (400× magnification).
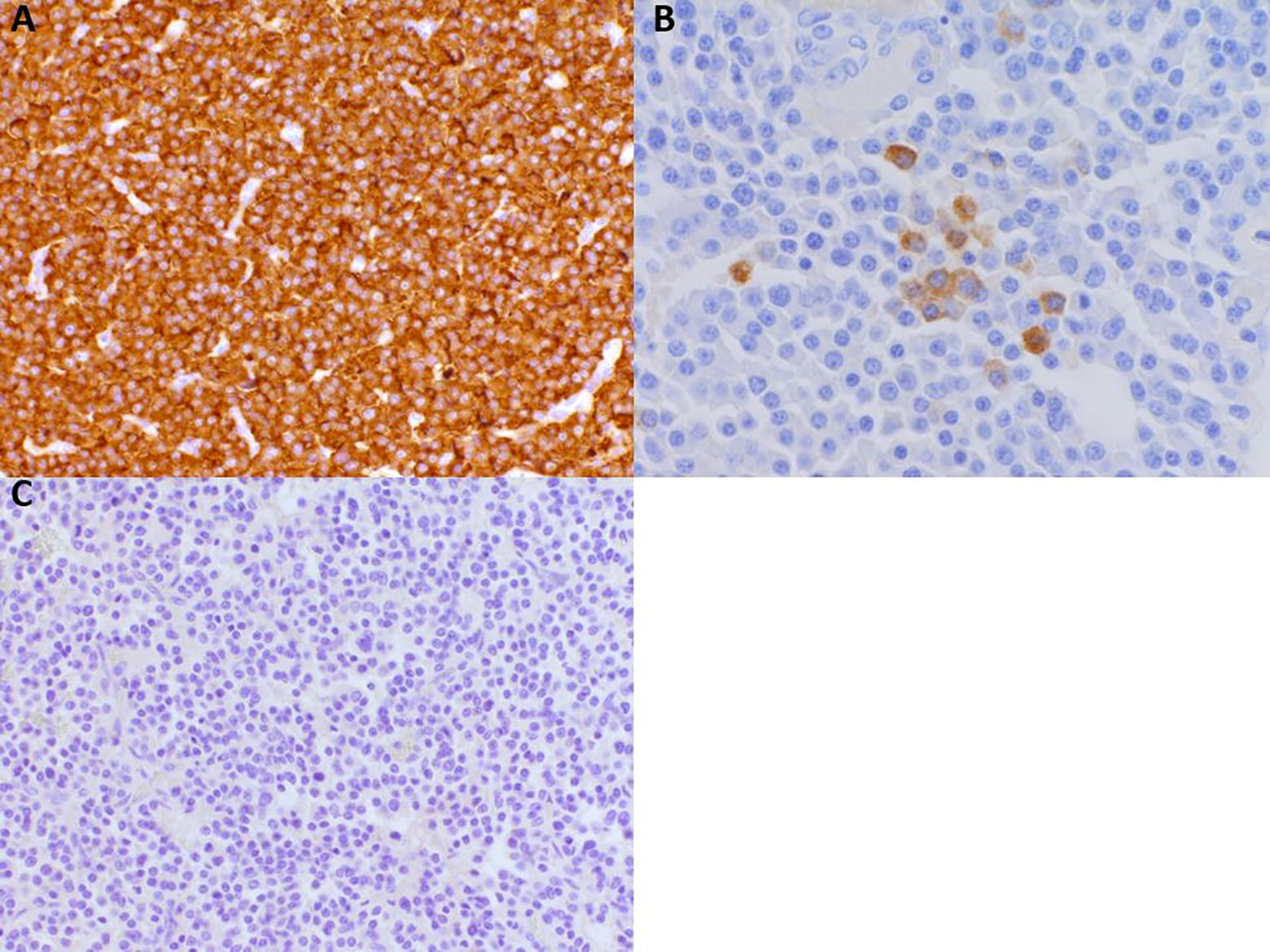
A, Synaptophysin immunohistochemical staining (200x magnification). B, Growth hormone immunohistochemical staining (400× magnification). C, Cytokeratin AE1/3 immunohistochemical staining (200× magnification).
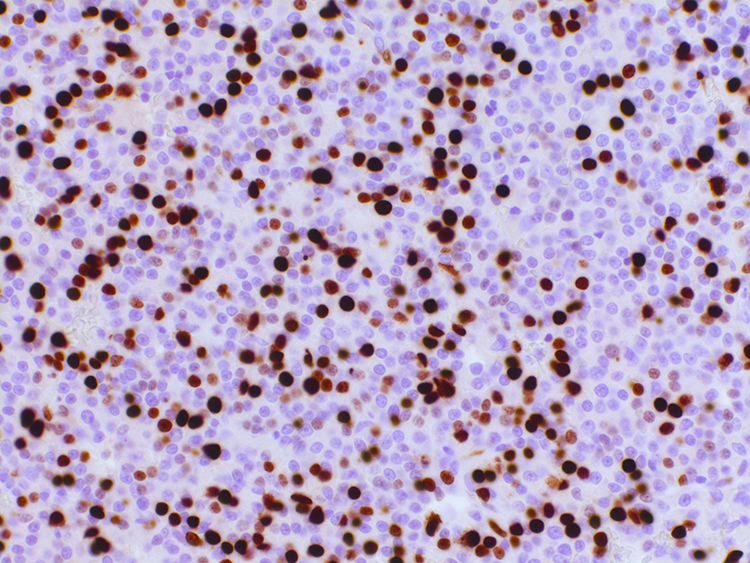
Ki67 immunohistochemical staining (200× magnification).
Discussion
Pituitary carcinomas are defined by a metastasis of a tumor of adenohypophyseal (anterior pituitary) cells, independent of the histological appearance. 6 Cervical nodal metastatic pituitary carcinomas are extremely rare and often present with symptoms related to sites of metastases, as primary pituitary carcinomas have been shown to be nonfunctioning in over 20% of cases. 7 Pituitary carcinomas are rare tumors with only 170 cases reported in the literature. 1 They form a very small proportion of pituitary tumors, which are commonly benign adenomas. Metastatic disease diagnosed by needle aspiration or needle biopsy are extremely rare and have only been reported in 6 patients,2-5,7,8 3 of whom had cervical nodal metastases, with other sites of metastases being the liver and cervical vertebra. We report an unusual case of cervical metastatic pituitary carcinoma diagnosed by core needle biopsy.
Due to the rarity of these tumors, pathological diagnosis from needle aspiration or biopsy is difficult, as a sufficient tissue sample is required for immunohistochemistry. Imaging can be helpful in the form of PET and computed tomography/magnetic resonance imaging (Figure 4). Histopathological findings may not be specific and include round to oval plasmacytoid cells with a moderate amount of cytoplasm arranged in small groups and variable nuclear features. 8 Immunohistochemistry is vital in the diagnosis of pituitary carcinomas and Ki-67 is a valuable prognostic marker, with a level of over 3% reported to prognosticate more aggressive behavior in primary pituitary tumours9,10 and more abnormal histological features including higher mitotic index often observed in metastases. 6 In our reported case, the Ki67 proliferative index was 10% in the pituitary tumor biopsy in 2011 and 31% in the metastatic carcinoma. In addition, p53 expression had been shown to correlate with invasiveness in pituitary carcinomas. 11 Although our case showed scattered positive pituitary hormone expression, as over 20% of pituitary carcinomas are nonfunctioning, pituitary hormone expression may not be helpful in the diagnosis of these tumors.
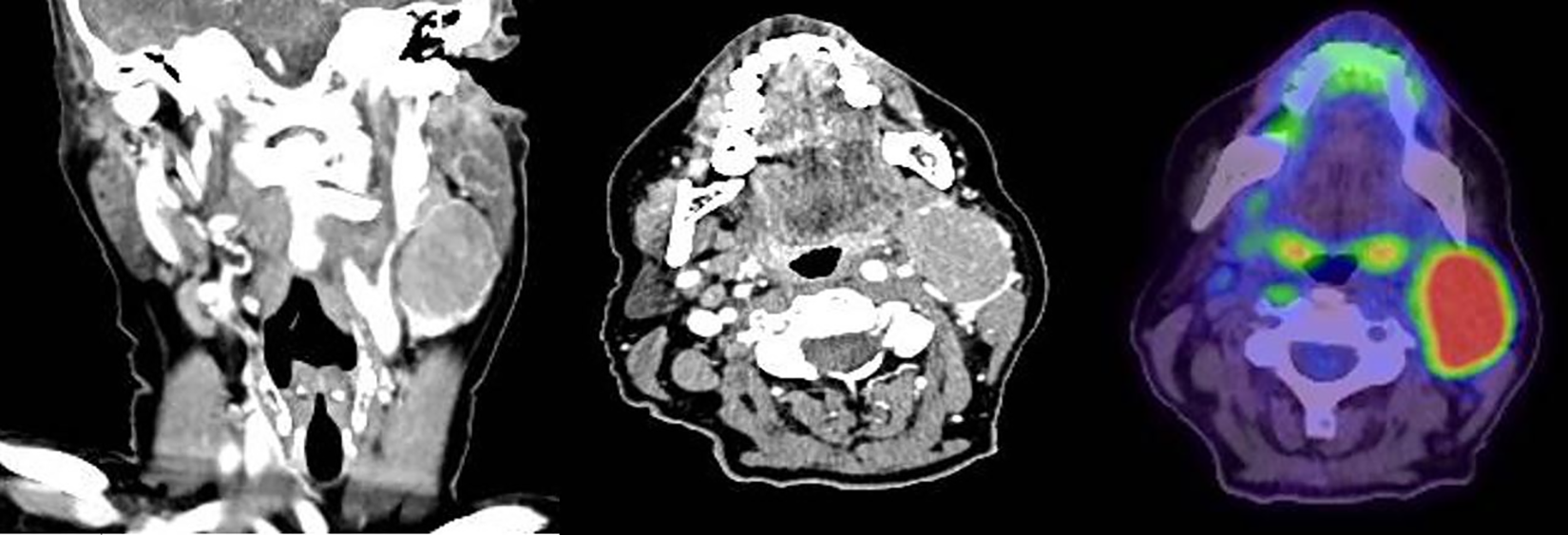
Computed tomography imaging demonstrating (left panel) coronal section and (central panel) axial section of nodal mass. Positron emission tomography axial slice (right panel) demonstrating avid nodal metastasis.
Pituitary carcinomas metastasize more frequently via hematogenous and lymphatic pathways rather than through the central nervous system. 12 Reported sites of metastasis vary and include the cerebral cortex, spinal cord, cervical and pelvic lymph nodes, lungs, liver, and bone. 1 The length of time taken for metastasis to occur from the initial diagnosis of a pituitary adenoma in our case was 8 years, which is consistent with the reported time frame in the literature. 13 Due to its rarity, treatment is not standardized but is typically multimodal incorporating surgical excision with or without nodal dissection, radiotherapy, and chemotherapy. 1 Prognosis of metastatic pituitary carcinomas are poor, with a median survival of 12 months in patients with systemic metastases and 2.6 years in those with central nervous system metastases. 9
Metastatic pituitary carcinomas are extremely rare tumors and diagnosis from needle aspiration or needle biopsies require immunohistochemical staining with clinicoradiological correlation. If metastatic pituitary carcinoma is suspected, we recommend core biopsy or lymph node excision to enable accurate histopathological diagnosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: J Virk received grants from HCA International and the Colledge Family Memorial Research Fund, Royal College of Surgeons for his fellowship.