
Abstract

Case Report
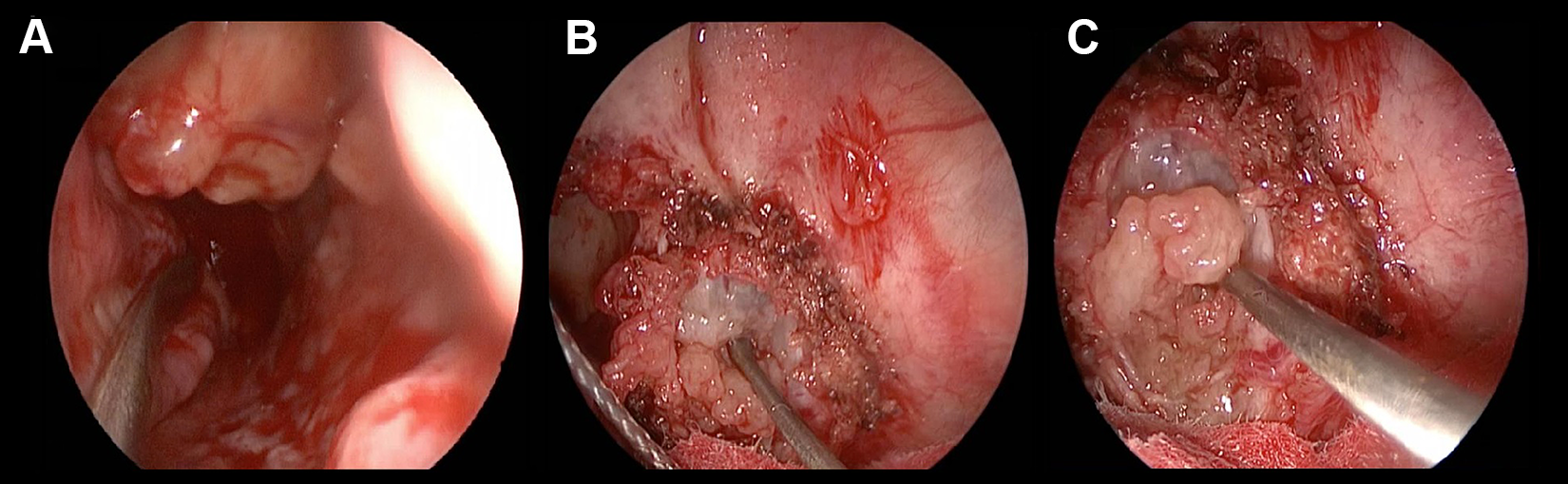
A 75-year-old male with a 2-year history of anosmia, nasal obstruction, and headaches visited at the Otolaryngology Unit of Villa Sofia-Cervello Hospital in January 2017. In the beginning, anosmia was the only symptom, but over time, the patient reported difficulty in breathing through the nose and frequent headaches. Endoscopic examination showed a large mass involving the right nasal cavity (Figure 1A).
A, Preoperative endoscopy evidences the external appearance of the Schwannoma. B and C, Intraoperative endoscopy shows the removal of the mass including the dura component before the placement of the fascia lata graft.
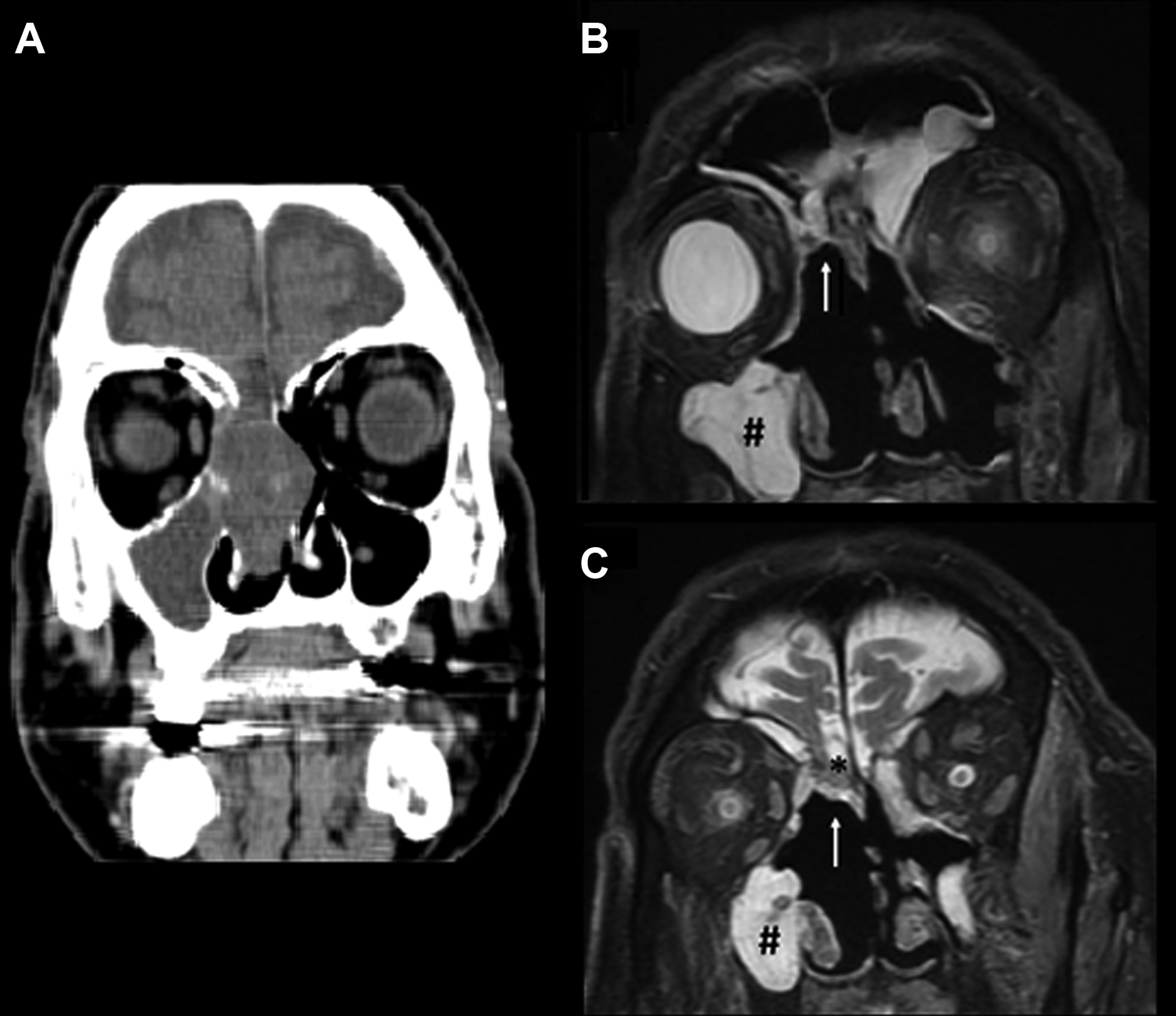
Computed tomography (CT) scan was performed at the Radiological Unit, showing a lesion arising from the right anterior olfactory cleft extending throughout the whole right nasal fossa and a reactive ethmoid–maxillary sinusitis (Figure 2A).
A, Preoperative computed tomography scan on the coronal plane evidences the presence of large mass arising from the anterior skull base and involving the right nasal fossa. B and C, In postoperative magnetic resonance imaging, on the coronal plane (A is a more anterior section), it is possible to see the excision of the neoformation (↑) and no evidence of cerebrospinal fluid leak; there is no presence of disease in the olfactory bulb (*); hyperintensity below on the right side suggests a maxillary sinusitis (#).
An endoscopic preoperative biopsy, performed under local anesthesia, lead to the diagnosis of Schwannoma of the olfactory nerve. Then the patient underwent transnasal endoscopic removal of the mass. Firstly, the surgeon debulked the neoformation starting from the right nasal fossa; afterward, right middle turbinectomy and progressive cauterization up to the olfactory fissure were performed (Figure 1B and C). The Schwannoma was completely removed, including the dural component, determining cerebrospinal fluid (CSF) leak, closed by a triple-layer fascia lata interposition (intracranial intradural, intracranial extradural, extracranial) and Autologous Fibrin Glue (AFG), placed in drops to fix the graft. The closure was completed with a free flap of the nasal mucosa with adipose tissue and more AFG sprayed over the closure region. The patient was then transferred to the intensive care unit and remained in anti-Trendelenburg position for 48 hours. Afterward, a nasal endoscopy showed no more evidence of CSF leaks. No complications (local toxicity, allergy reactions, infections) were observed. After 30 days, the patient underwent follow-up magnetic resonance imaging (MRI; Figure 2B and C) and endoscopy. Definitive histological examination showed a spindle cell proliferation with hemorrhagic and pseudocystic areas (Figure 3A).
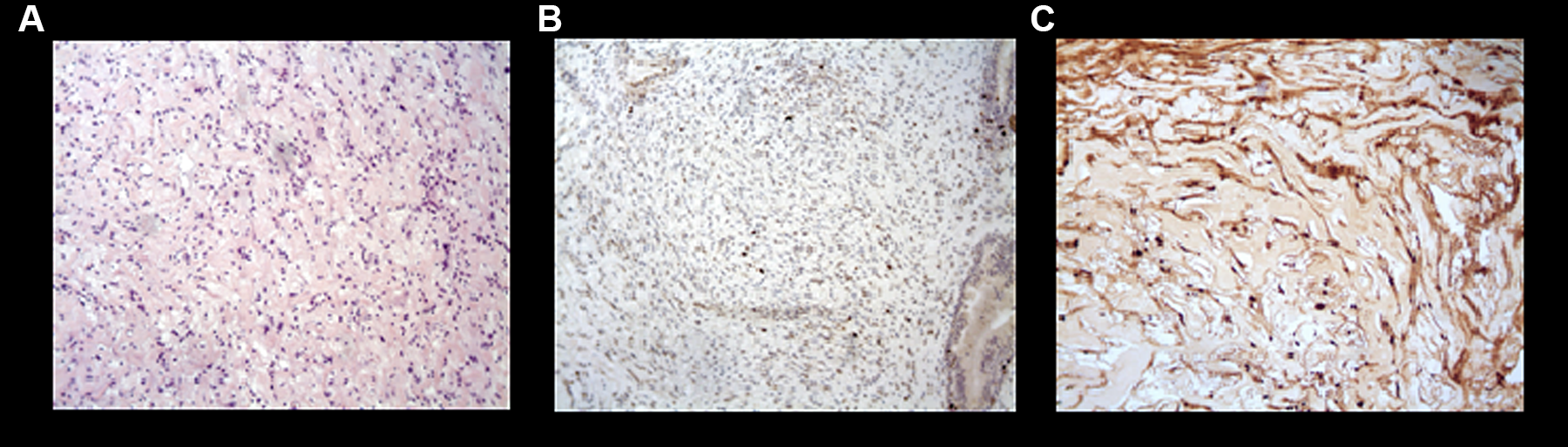
A-C, Pathologic examination of the Schwannoma shows the presence of spindle cells with eosinophilic cytoplasm proliferation (A); a limited number of cells positive to Ki-67 (B); positivity to S100 (C).
Furthermore, the diagnosis of Schwannoma with low expression of Ki-67 (Figure 3B), S100 (Figure 3), and Leu7/CD57 positive with degenerative changes was confirmed by immunohistochemical analysis.
Discussion
Schwannomas of the anterior cranial fossa (ACF) are extremely rare: To the best of our knowledge, only 68 cases, including this one, had been reported in the literature1,2. Symptoms depend on the localization of the mass 3 : In this case, anosmia and nasal obstruction were determined by the nasal fossa extension.
Althought MRI or CT are particularly useful for the scanning and detection of abnormalities in soft tissue4,5, there are no specific findings to differentiate Schwannomas from other types of contrast-enhancing formations. So, a preoperative biopsy has been performed to identify the nature of the mass. From a histological standpoint, Schwannomas are characterized by the coexistence of compact, spindled Antoni A areas and microcystic hypocellular Antoni B areas 3 (Figure 3A). Immunohistochemical lack of epithelial membrane antigen and strong S100 reactivity3,6 (Figure 3C) supports the diagnosis of Schwannoma over neurofibroma and malignant peripheral nerve sheath tumors 3 . Our case was CD57 positive. Negativity of CD57 instead characterizes the olfactory ensheathing cell tumor, which is more aggressive 7 .
Histopathological differential diagnoses include esthesioneuroblastomas, papillomas, meningiomas, nasopharyngeal carcinomas, and sarcomas 8 . The most common therapeutic choice reported is the resection via a subfrontal approach1,9. Although it is considered very conservative10,11, an endoscopic transnasal removal is not always viable and has been used only in a limited amount of cases12-14; when the mass shows intranasal expansion, an endonasal approach could be considered for the exeresis.
In this case, the surgery involved the dural component, determining a CSF fistula: we employed AFG produced with Vivostat to fix both the triple-layer fascia lata and the free flap of the nasal mucosa with adipose tissue interpositions.
Vivostat is a system producing AFG directly from the patient’s blood in approximately 23 minutes, thus avoiding any possible allergic reaction and human borne infections, such as Hepatits A Virus, Hepatits C Virus, or parvovirus B19. This sealant can be applied in single drops or sprayed over the lesion or the graft15-17. After the closure of CSF leak, 30-day follow-up was performed with MRI and endoscopy showed the absence of residual leak and thus the correct execution of the closure.
In conclusion, ACF Schwannomas are very uncommon findings, grossly appearing as an expansive mass without characteristic features. In this case, nasal fossa Schwannoma caused nasal obstruction, anosmia, and headaches. Imaging of Schwannoma (MRI or CT) can be useful to identify the position and the dimensions of the neoplasm, but the final diagnosis is based on pathological examination. When the mass extends in the nasal cavities, we suggest to consider surgery via an endoscopic approach. AFG has been effective in the closure of the CSF leak. This report is the first describing an autologous sealant skull base reconstruction technique after the endoscopic transnasal resection of an olfactory Schwannoma.
Footnotes
Authors’ Note
Salvatore Poma and Domenico Michele Modica contributed equally to this work. Informed consent was obtained from the patient included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.