
Abstract
Objective:
This report aimed to present a case of acute calcific tendinitis of the longus colli muscle as an uncommon cause of neck pain and dysphagia and is often misdiagnosed as a retropharyngeal abscess.
Methods:
Case report and literature review.
Results:
Acute calcific tendinitis is often misdiagnosed as a retropharyngeal abscess; however, it is distinguished from the latter based on patient history and unique radiologic findings. History, examination, and laboratory findings do not suggest an infectious etiology, and radiographic findings include a non-rim-enhancing fluid collection with or without calcifications anterior to the upper cervical spine.
Conclusion:
Unlike retropharyngeal abscess, acute calcific tendinitis is managed conservatively. When consulted for a possible retropharyngeal abscess, the otolaryngologist should avoid anchoring bias by independently obtaining a detailed history and examination and personally reviewing radiologic images to avoid unnecessary intervention.
A previously healthy 44-year-old male presented to the emergency department with 3 days of severe right-sided neck pain that was aggravated by movement and was associated with trismus and odynophagia. He denied recent upper respiratory infection symptoms, recent surgery, or traumatic injury. He also denied fevers, chills, runny nose, ear pain, cough, congestion, chest pain, or shortness of breath. His occupation involved physical labor. On examination, the patient was afebrile with stable vital signs. There was no appreciable cervical lymphadenopathy; however, the patient did exhibit tenderness to palpation over the right posterior neck and associated decreased range of motion. Laboratory findings included a normal white blood cell count, an elevated C-reactive protein level of 19.4 mg/L, and an elevated erythrocyte sedimentation rate of 25 mm/hr. Computed tomography (CT) of the neck with contrast described a retropharyngeal/prevertebral fluid collection extending from C2-C6 associated with right parapharyngeal soft tissue swelling (Figure 1).
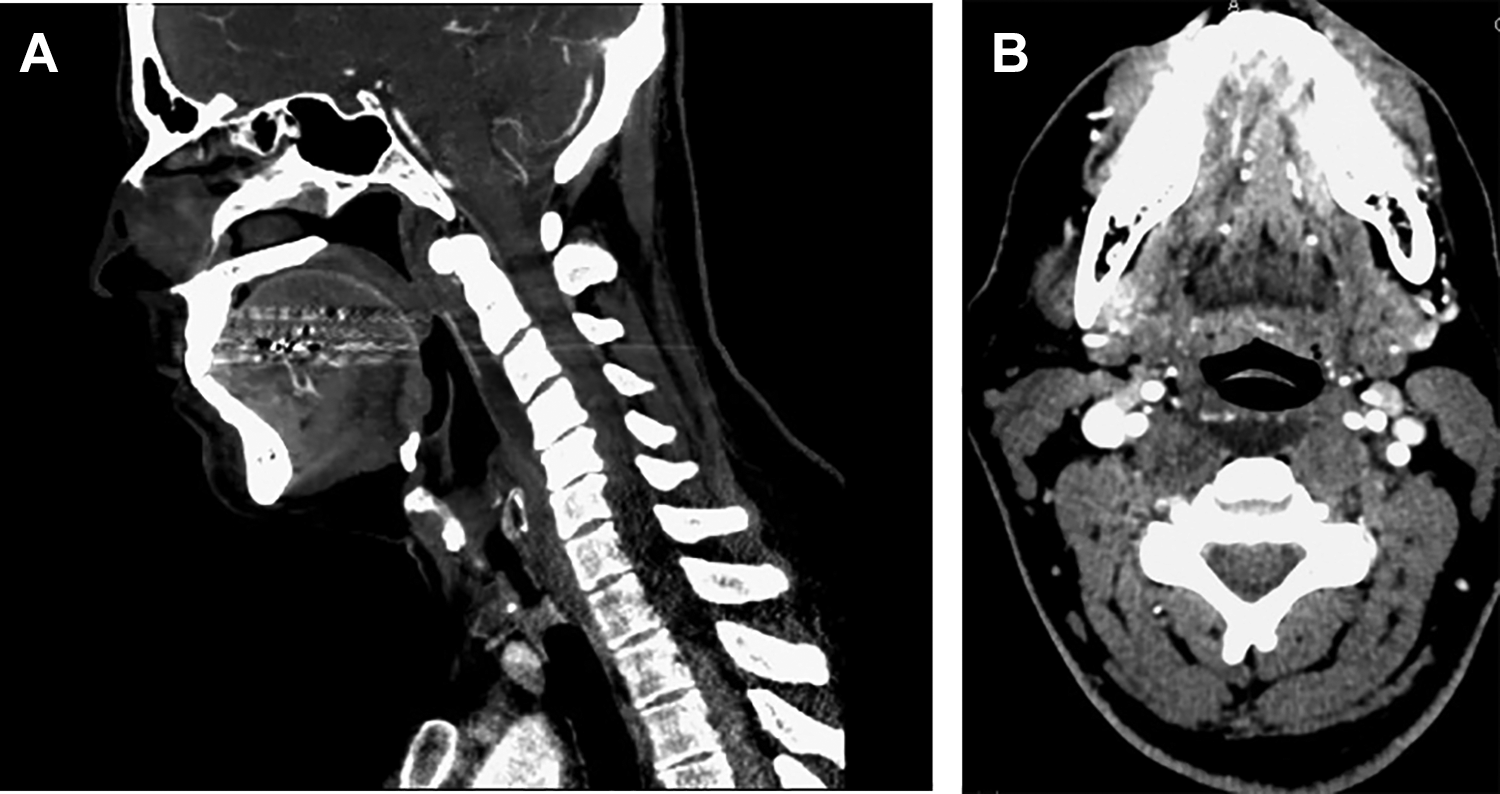
A, Sagittal view of non-rim-enhancing prevertebral fluid. B, Axial view of non-rim-enhancing prevertebral fluid.
Acute calcific tendinitis of the longus colli (ACTLC) muscle, also termed retropharyngeal calcific tendinitis, is an uncommon but self-limited cause of neck pain. However, due to similarities in presentation and clinical findings, ACTLC is often misdiagnosed as a retropharyngeal abscess, a more common and serious condition often requiring surgical intervention.
ACTLC occurs when calcium hydroxyapatite deposition occurs in the longus colli tendon, inciting a reactive inflammatory response in the longus colli muscle. 1 Located within the prevertebral space, the paired longus colli muscle is anterior to the cervical vertebral column, extends from C1 to T3, and is involved in flexion and mild rotation of the head and neck. 2 There are 3 portions of the muscle: the superior oblique, inferior oblique, and vertical portions. 2 The superior oblique portion extends from the transverse processes of C3-C5 and inserts on the anterior tubercle of C1 and is most commonly involved.3,4 Repetitive trauma and degeneration of the longus colli tendon are suspected etiologies that precipitate calcium hydroxyapatite deposition. 5 The presence of these crystals triggers an inflammatory response resulting in tendinitis and a reactive retropharyngeal fluid accumulation that can be mistaken as an abscess on imaging. 6 Acute calcific tendinitis of the longus colli is more commonly diagnosed in adults aged 30 to 60 without a gender predisposition.3,4,6,7 The incidence of ACTLC is hypothesized to be underreported due to misdiagnosis.4-6
Patients with ACTLC often present with acute or subacute onset of neck pain, dysphagia, odynophagia, sore throat, and low-grade fever. 8 Patients may report a progressive worsening of symptoms, limited range of motion in the cervical spine, and pain exacerbated by movement.
Laboratory findings in ACTLC may include a normal or mild leukocytosis, elevated C-reactive protein, and mildly elevated erythrocyte sedimentation rate.7-8 Examination is often unremarkable or may show mild posterior pharyngeal fullness on laryngoscopy. 8 Computed tomography imaging, which is needed to make the diagnosis of ACTLC, 5 typically demonstrates nonspecific soft tissue edema in the prevertebral or retropharyngeal soft tissues extending from C1 to as inferiorly as C6 with a lack of rim enhancement. 8 Additionally, globular or linear calcifications, often near the insertion of the superior oblique portion of the longus colli muscle at C1, are characteristic of ACTLC.
Our patient’s CT images lacked obvious calcifications but revealed fluid without rim enhancement. The patient’s laboratory findings, lack of fever, and unremarkable examination were also consistent with ACTLC. Additionally, the patient presented with a history of suspected repetitive use injury related to his occupation, further favoring a musculoskeletal diagnosis such as ACTLC.
Acute calcific tendinitis of the longus colli typically resolves within several weeks of symptom onset. 3 Contrary to management of retropharyngeal abscesses, antibiotics and surgical intervention are not indicated in ACTLC.4,5 Instead, treatment is conservative and is aimed at decreasing the duration of symptoms, including rest and nonsteroidal anti-inflammatory medications. Systemic corticosteroids are reserved for severe cases. 5
In summary, when a patient presents with CT findings of a non-rim-enhancing retropharyngeal fluid collection without history, examination, or laboratory findings to strongly support an infectious etiology, ACTLC should be considered in the differential diagnosis. Because the presentation is similar to other conditions such as deep neck space infection, meningitis, cervical disc herniation, and vertebral fractures, 9 a detailed history and physical examination along with laboratory and imaging studies are needed to narrow the differential diagnosis. Recognizing ACTLC limits unnecessary antibiotic use, obviates invasive surgical intervention, and decreases other costly health care–related expenses.
Footnotes
Authors’ Note
There are no financial disclosures and there are no sources of funding. This submission has not been presented or published elsewhere.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.