
Abstract
Background:
Use of suction drain after superficial parotidectomy (SP) is based on national consensus considered best practice, but there is no evidence on the effect of the treatment. The aim of the present study is to evaluate the effectiveness of drainage after SP by evaluating the rate of complications after SP in relation to the (ie, duration) of drainage and tumor size.
Methods:
Retrospective analysis was performed involving data from all consecutive patients undergoing SP at the Ear, Nose, and Throat department, Regional Hospital West Jutland, Denmark, between January 1, 2011, and December 31, 2017. Demographics including comorbidity, medication, tumor size, postoperative secretion through the drainage, as well as complications (hematoma, seroma, infection, fistulas, Frey syndrome, facial nerve palsy) were registered. Patients with secretion below 25 mL were compared to patients with secretion above 25 mL, that is, drainage less than 24 hours versus longer than 24 hours.
Conclusion:
Overall, the risk of complications after SP increased with secretion beyond 25 mL (ie, drainage for more than 24 hours). This applied in particular to infections and seromas/hematomas demanding treatment. The use of routine drainage after SP is questionable, and a randomized trial is warranted to unravel the necessity of postoperative drainage.
Keywords
Introduction
Salivary gland neoplasms account for approximately 3% to 10% of all head and neck tumors of which 70% to 80% are benign.1-3 The most common benign subtypes are pleomorphic adenoma (PA) with 65%, followed by adenolymphoma (Warthin tumor) with 25%. 3 Left in situ, there is a time proportional risk of malignant transformation of PA’s (1.6%-7.5%). 4 As a consequence, and to ensure benign pathology, adequate treatment of benign parotic gland tumors involves ultrasound scan, fine needle aspiration followed by surgical removal. In majority of cases, the tumors are located to the superficial lobe of the parotic gland, hence superficial parotidectomy (SP) is the technique of choice.5-7 Insertion of suction drain in surgical wounds in the head and neck region is recommended on the basis of national consensus but with no evidence to confirm the prophylactic effect. Also, empirically, the drain is removed the day after surgery if the amount of secretion is less than 25 mL. The patients remain hospitalized until the drain is removed. The underlying philosophy is that drainage avoids complications such as hematomas and seromas, albeit previous studies found that approximately 2.4% of patients developed hematomas and 4.2% developed seromas despite drainage.3,8 Furthermore, the drain itself increases the risk of postoperative infection because of an open access to the underlying tissue (1%-13%), as well as the risk of developing salivary fistula (2%-10%).2,3,8,9 In addition to hematomas, seromas, salivary fistula, and infection, other complications are associated with SP. The risk of temporary facial nerve palsy has been reported between 18% and 65% after SP, whereas rates of permanent nerve weakness were between 0% and 19%.1-3 Another commonly reported complication following SP are Frey syndrome (1%-25%).1-3,8-12 From a cost-benefit point of view, surgery without drainage seems attractive as the patients can be discharged after a few hours, but of cause only if it is without a higher risk of postoperative complications.
The empirical use of drainage raises 2 questions:
Is it reasonable to set the limit for removal of the drain at 25 mL?
Is drainage necessary at all?
Is there a correlation between tumor size, drainage volume, and complications?
The null hypothesis of the present study was that removal of drains with less than 25 mL secretion (less than 24 hours) was associated with the same risk of complications as in cases with more than 25 mL (longer than 24 hours).
The aim of the present study is to evaluate the effectiveness of drainage after SP by evaluating the rate of complications after SP in relation to the (ie, duration) of drainage and tumor size.
The primary outcome was to determine the rate of complications in terms of postoperative infection, hematomas, seromas, fistula, Frey syndrome, and facial palsy, and to compare patients with less than 25 mL secretion with those above 25 mL. The secondary outcome was to identify risk factors associated with less/more than 25 mL (24 hours). Furthermore, to investigate the correlation between tumor size and drainage volume.
Patients and Methods
The study was approved by the local administration of the department, and followed the general recommendations of discretion to personal data as well as the Helsinki declaration.
Data Selection
Demographic data, comorbidity, and complication data were collected from the electronic patient database including specific clinical investigations.
Surgical Procedure
Preoperatively, ultrasound was performed in all cases to confirm unifocal disease as well as fine needle aspiration to ensure benign cytology. The surgical procedure (SP) was performed by 3 experienced head and neck surgeons by the following technique: As the majority of the parotid gland is located lateral to the facial nerve, SP is the adequate treatment of most benign tumors. Occasionally, the tumor is located in the deep lobe of the gland. In such cases, SP is the initial step in removal of the tumor. After local anesthesia with carbocaine with adrenaline (1%), a skin incision was made starting in the preauricular skin crease from above the tragus going inferiorly underneath the earlobe, inferiorly to the mastoid tip directed to an upper neck skin crease, 2 to 3 cm below and parallel to the mandible. Anterior and posterior skin flaps were raised. The anterior flap was raised to the masseter muscle exerting caution to the superficially running facial branches at the anterior border of the gland. At the posterior border, the gland was freed off the cartilaginous ear canal, the mastoid tip and the sternocleidomastoid muscle. After visualization of the main trunk, blunt dissection parallel and superficial to the nerve was performed. The tumor and surrounding gland tissue were removed. Occasionally the nerve (main trunk or branches) was in close contact with the tumor capsule. In such cases, a partial enucleation of the tumor was performed in order to preserve the facial nerve function.
Postoperative Management
After meticulous hemostasis, an active suction drainage was placed in the operative cavity. The nerve was protected by an absorbable hemostatic mesh (Surgicel, Ethicon). The skin was closed in 2 layers, using absorbable interrupted subcutaneous sutures and interrupted nylon sutures for the external skin. Patients with suction drain stayed at the hospital overnight for observation. The day after the operation, the drain was removed if less than 25 mL secretion was observed, the wound covered with a light absorbing band and the patient was discharged. Skin sutures were removed 6 to 7 days postoperatively in the outpatient clinic. No prophylactic antibiotics (PAB) were administered as there was no national consensus at the time of writing.
Statistical Analyses
All data were analyzed with JMP 13 for Mac (SAS Institute Inc). Drainage-groups with an output of >/< 25 mL were compared using logistic regressions analysis of the risk of complications. Odds ratios and confidence intervals were calculated. Two-sided t test was used to compare continuous variables between groups (age and tumor size). P values <.05 were considered significant.
Results
From January 2011 to December 2016 a total of 226 patients underwent SP at the Ear, Nose, and Throat (ENT) department Holstebro, Hospital unit West, Denmark. Twenty-one patients did not meet the inclusion criteria, either because of age or malignity, leaving 205 patients for inclusion.
Patient Demographics and Diagnoses
The gender ratio was 103 women:102 men, and the average age was 56 years (18-88 years). The histological subtypes were primarily PA (51.7%) and Warthin tumor (37.5%) the last 10.8% was different histological subtypes. In 199 cases, it was possible to identify tumor size.
Comparison of patient demographics is listed in Table 1 in relation to amount of secretion. Secretion below 25 mL the first postoperative morning was found in 160 (78%) patients.
Demographics by Group (mL in Drain).
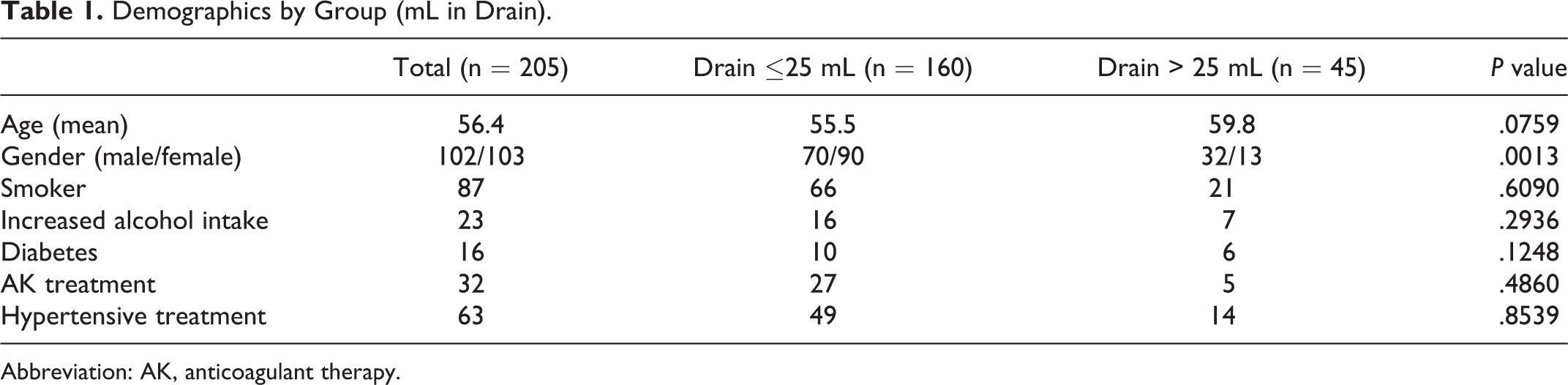
Abbreviation: AK, anticoagulant therapy.
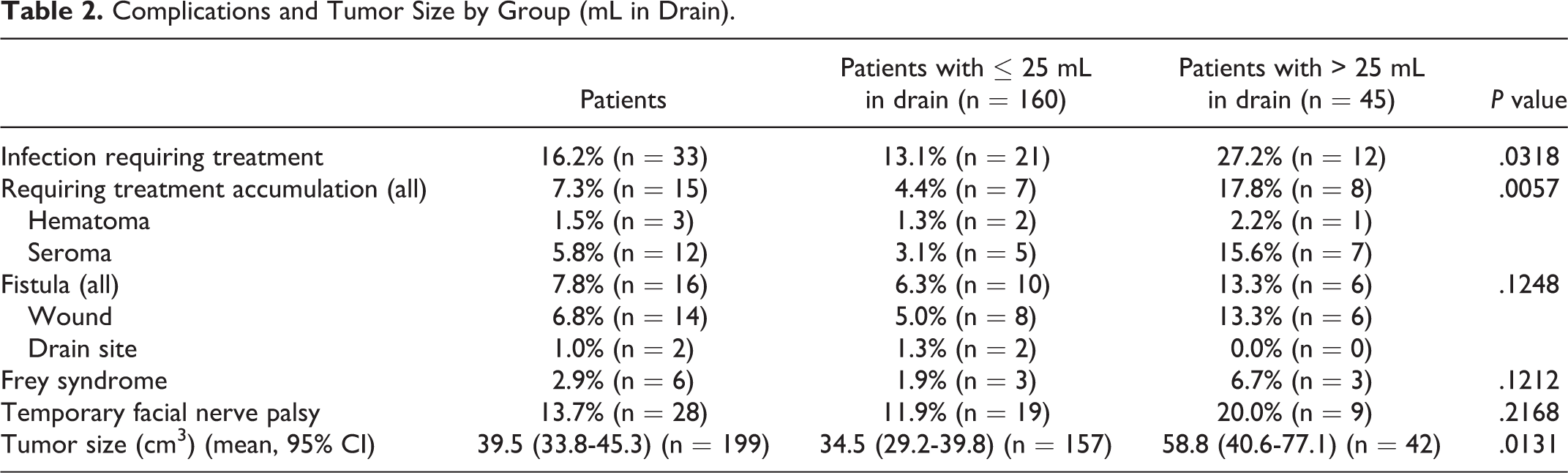
The most common complication was wound infection (16.2%), which was treated with systemic antibiotics alone (Table 2). Infection was considered when a sign of redness, swelling, localized warmth, fever, or pain was noted. After removal of the drain, 1.5% developed seromas and 5.8% hematomas. The diagnosis of seroma or hematoma was based on ultrasound scan. The treatment was aspiration from the cavity and subsequently follow-up in the outpatient clinic. Salivary fistulas developed in 7.8% of the patients, but rarely at the drain site. None of the salivary fistulas were permanent. Frey syndrome was diagnosed among 2.9% of patients. Postoperative facial nerve function remained intact in most cases, except in 13.7%, who had temporary facial palsy. All regained normal facial function within 6 months. Significantly higher incidences of postoperative infections (χ2 = 4.609, P = .0318) and development of hematomas and seromas were seen among patients with more than 25 mL secretion (χ2 = 7.704, P = .0055). Especially, it is notable that 28.1% of the patients who developed infections also presented with seromas or hematomas. In line with these findings, the remaining types of complications tended to occur among patients with more than 25 mL secretion, though not significantly. In order to identify the risk of developing postoperative complications, odds ratio and 95% confidence intervals (CI) were calculated as shown in Table 3.
Complications and Tumor Size by Group (mL in Drain).
Odds Ratio for Postoperative Complications.
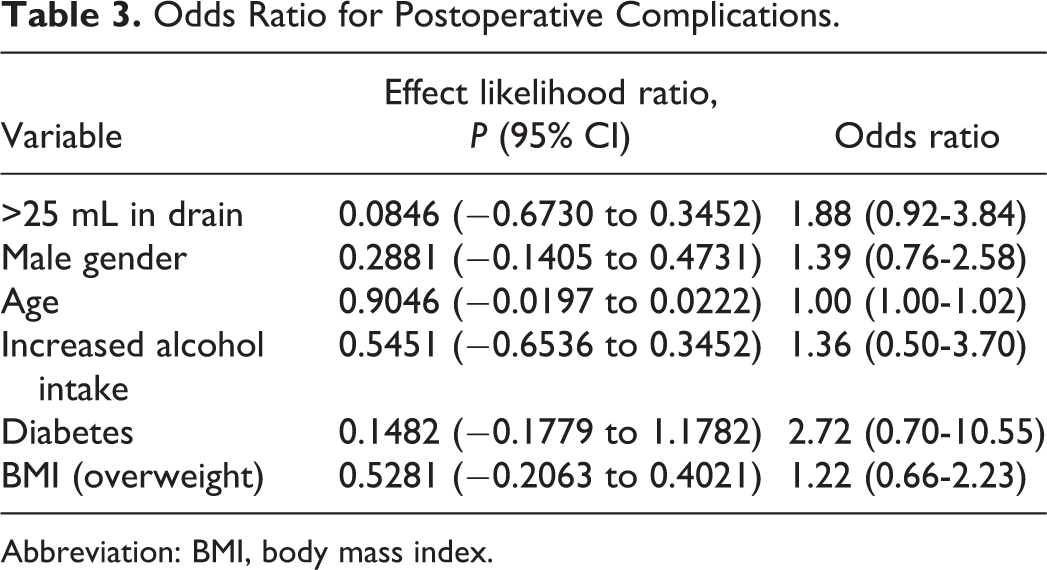
Abbreviation: BMI, body mass index.
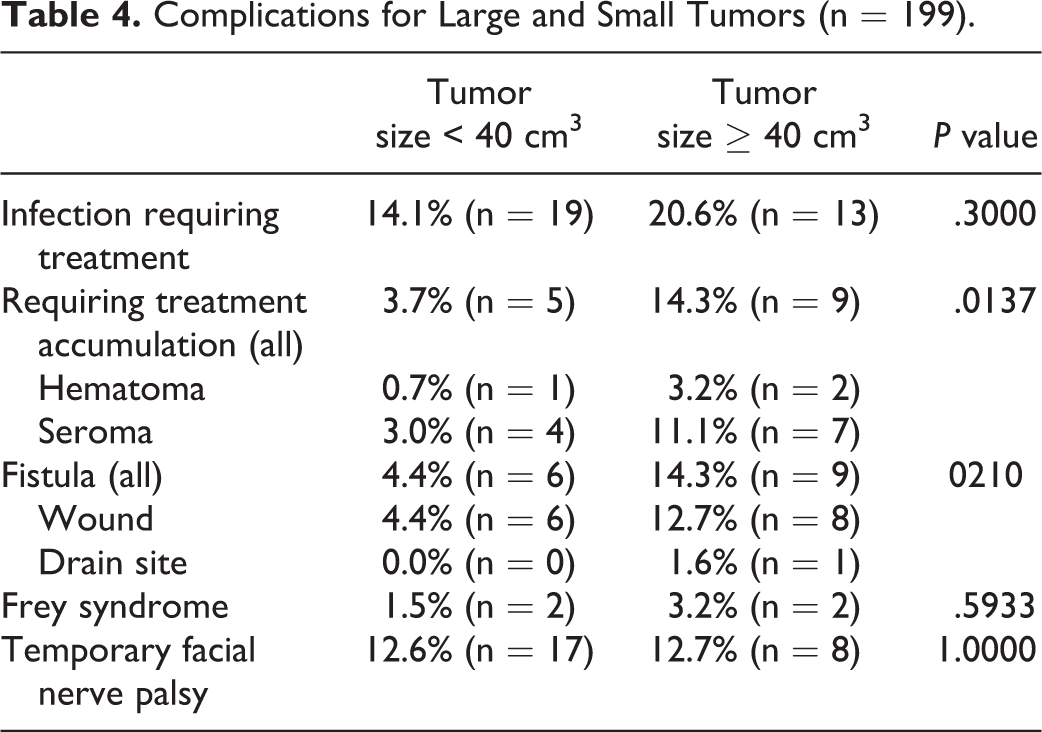
Male gender (P < .001) and tumor size (P = .0131) were associated with a statistically significant higher incidence of more than 25 mL secretion whereas age, smoking status, comorbidity, and medication were nonsignificantly related to amount of secretion. A cutoff for tumor size was identified at 40 cm3 (1.8-292.5 cm3). There were statistically significant correlations with tumor size and development of fistula (0.0210) and seromas and hematomas (0.0137; Table 4).
Complications for Large and Small Tumors (n = 199).
Discussion
To the best of our knowledge, only one study has investigated the correlation between drainage treatment and the incidence of postoperative complication for patient undergoing SP. 13 The specific study finds no significant difference between the drain/no drain groups, but mentions tumor size as a statistical significant risk factor for postoperative secretion. 13 In addition, our study did confirm a statistically significant association between tumor size and secretion above 25 mL. Overall, complications occurred more frequently after SP among patients with secretion beyond 25 mL (ie, drainage for more than 24 hours). In particular, the risk of infection and development of seromas or hematomas was significantly increased, although not unequivocally correlated to tumor size (Table 4).
In this study, it was not investigated whether the patients’ nutritional status had an influence on their ability of wound healing, but it is common knowledge that the nutritional status and wound healing is closely related. However, delayed wound healing in SP, most often caused by wound infection, is well described in the literature.3,5,9,14 In earlier studies, there has not been formulated a connection between the duration of drainage/the amount of secretion and the risk of developing infection after SP. However, Salem et al described drain as an independent risk for surgical side infection after thyroidectomy. 14 Likewise, in a nationwide cohort study (The Danish Thyroid Surgery Database) from 2009, Godballe et al described an increased hospital stay and infection rate in patients treated with drainage after thyroidectomy. 15 In none of these studies was tumor size considered a single risk factor in developing complications. In a previous Danish study from 2014 by Rasmussen et Ovesen, an infection rate of 13% of all head and neck surgical procedures was reported in a study of 362 patients at a Danish university clinic. Even though their study investigated a heterogeneous ENT patient cohort, the infection rate is nevertheless comparable to the findings in our study. 16 Coniglio et al compared a historic cohort of 91 patients before and after introduction of drainless treatment in a private clinic. This cohort is comparable in age and gender to our study and did not find a statistically significant difference in relation to infection rate (P = .91) between the 2 groups; drainage 2% (standard deviation: SD 0.1%-12.6%) and drainless 2.4% (SD 0.1%-10.9%). It was not mentioned whether a prophylactic antibiotic treatment had been given prior to the surgical treatment. 13 In the same study it was hypothesized that tumor location (level) and the surgical lesion, likewise could be a risk factor for secretion. This has not been investigated in this study, but could be a focus of future investigation.
A total of 7.3% of patients in the present study developed seromas or hematomas in spite of drainage. This correlates with previous findings,9,13 albeit no other study did distinguish between outcome secretion. Although it is common practice to use drainage after SP, our findings indicate that it is important to consider whether drainage prevent seroma and hematomas as well as expected. However, it is still necessary to further investigate the drain versus no drain effect after SP, especially in the light of the overlap between development of seromas and hematomas and the development of wound infection.
In our study, a total of 16 (7.8%) patients developed saliva fistulas, but only 2 (1%) patients at the drainage site. Klintworth et al had a similar rate of fistula formation, but the localization of the fistulas was not specified. 3 In the present study, there was a tendency toward higher secretion correlated with higher fistula occurrence, though not significantly.
Seventy-eight percent of the patients in our study had secretion less than 25 mL in the drain, and may as such be considered as overtreated. From an economic point of view, surgery without drainage seems attractive, as the patient can be discharged after a few hours compared to a minimum of one night hospitalization as current practice prescribes. Based on review of the literature, there is no consensus on the use or duration of drainage as postoperative treatment.3,5,6,13 Kligerman et al described a mean duration of postoperative drain of 4 to 5 days. 5 They did not describe a limit secretion value for drainage or any postoperative infection, and it is unclear whether PAB were administered. Previous studies have investigated the effects of PAB in surgery of the head and neck region.16,17 These studies found that even though most head and neck procedures are clean, the infection rate was nevertheless improved by the use of PAB in a single dose pre- or perioperatively. 17 The high infection rate in the current and previous studies indicates that the drainage in itself lacks the prophylactic effect that one could hope for. Therefore, a single use of PAB is an issue for further investigation.
We conducted a multivariate analysis as we wanted to distinguish between patients who needed a drain and those who did not need drainage due to the certain demographic characteristics. We found no evidence that gender, age, diabetes, body mass index, smoking, medications, or alcohol led to increased output in the drainage. Nonetheless, there seemed to be a tendency toward men having higher output in the drainage and therefore a theoretically higher risk of getting hematoma and seroma if not treated with drainage.
Limitations
As our study is retrospective and without a control group, a randomized trial is recommended to unravel the necessity of drainage in relation to SP. Furthermore, the role of PAB, tumor size, tumor location, and surgical lesion should be clarified.
Conclusion
Based on the present results, it could be questioned, whether use of drainage had been unnecessary among the 78% patients presenting with less than 25 mL secretion. Tumor size and male gender were both considered a statistically significant risk factor, but no further demographics were associated with complications. Our rates of complications are in line with previous findings. We have added to the literature that the risk of postoperative infection and development of seromas and hematomas correlate to amounts of secretion beyond 25 mL, that is, drainage for more than 24 hours and tumor size correlates with a higher secretion.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.