
Abstract
Sinonasal organized hematomas (OHs) are rare lesions that primarily localize to the maxillary sinus. The rate of growth of these masses has not been described in the literature. We present a case of a 59-year-old gentleman with polyostotic fibrous dysplasia who presented with acute loss of vision in the left eye from an expanding OH of the sphenoid sinusitis. After expanded endonasal, transpterygoid approach and debulking, patient experienced significant vision improvement. Close follow-up imaging preoperatively allowed radiologic documentation of the rate of OH growth and this is presented in detail.
Keywords
Introduction
Sinonasal organized hematoma (OH) is a rare, slow growing, 1,2 and destructive lesion with almost all reported cases localized to the maxillary sinuses. 3 -5 First described in the Japanese literature as a “blood boil” within the maxillary sinus, 6 patients with OH most commonly present with epistaxis and nasal obstruction, headache, facial pain, epiphora, and other compressive symptoms seen less commonly. 4,5,7 Various conjectures regarding pathophysiology have been described, but all share the common causative event of an initial hemorrhagic event derived from various etiologies. 2,5,7 -9 The hemorrhagic contents undergo organization through fibrosis and neovascularization, and the vascular mass expands over time. 5,10 The rate of growth of OH and the initial hemorrhagic event have never been specifically observed and reported in the literature.
We present a case of OH causing blindness secondary to optic nerve compression in a patient with fibrous dysplasia (FD) and visual recovery after expanded endonasal surgery. Independently, the patient underwent close radiologic follow-up preoperatively secondary to his underlying FD and worsening headaches uniquely allowing for radiologic documentation of the rate of OH growth.
Case Report
A 59-year-old gentleman with extensive history of cranial/maxillofacial FD presents with worsening headaches for 1 year. He has a history of multiple reconstructive surgeries of the orbit and cranial vault in the past and reports aborted plastic operations secondary to severe bleeding. He underwent sphenoidotomy for mucocele 8 years prior to presentation. Physical examination and nasal endoscopy show baseline exophthalmos, extensive facial deformity, and scarring with hypertrophic tissue in bilateral sphenoethmoidal recess and middle meatus recess with loss of landmarks.
Computed tomography (CT) showed a soft tissue mass occupying 90% of the left sphenoid sinus with a large middle cranial fossa defect and complete clival recess and left carotid canal erosion. Multiple past CTs were available dating back to 50 months prior to presentation (t-50 months). The mass had been stable from t-50 months to t-13 months (Figure 1). Growth was evident between t-13 months and time of presentation. Magnetic resonance imaging (MRI; Figure 2) demonstrated a 5.5 cm lobular heterogeneously enhancing soft tissue mass filling the left sphenoid sinus encroaching the left cavernous sinus and encasing the left orbital apex. The mass showed extensive, interspersed enhancement centrally and frond-like T2 hyperintensity.
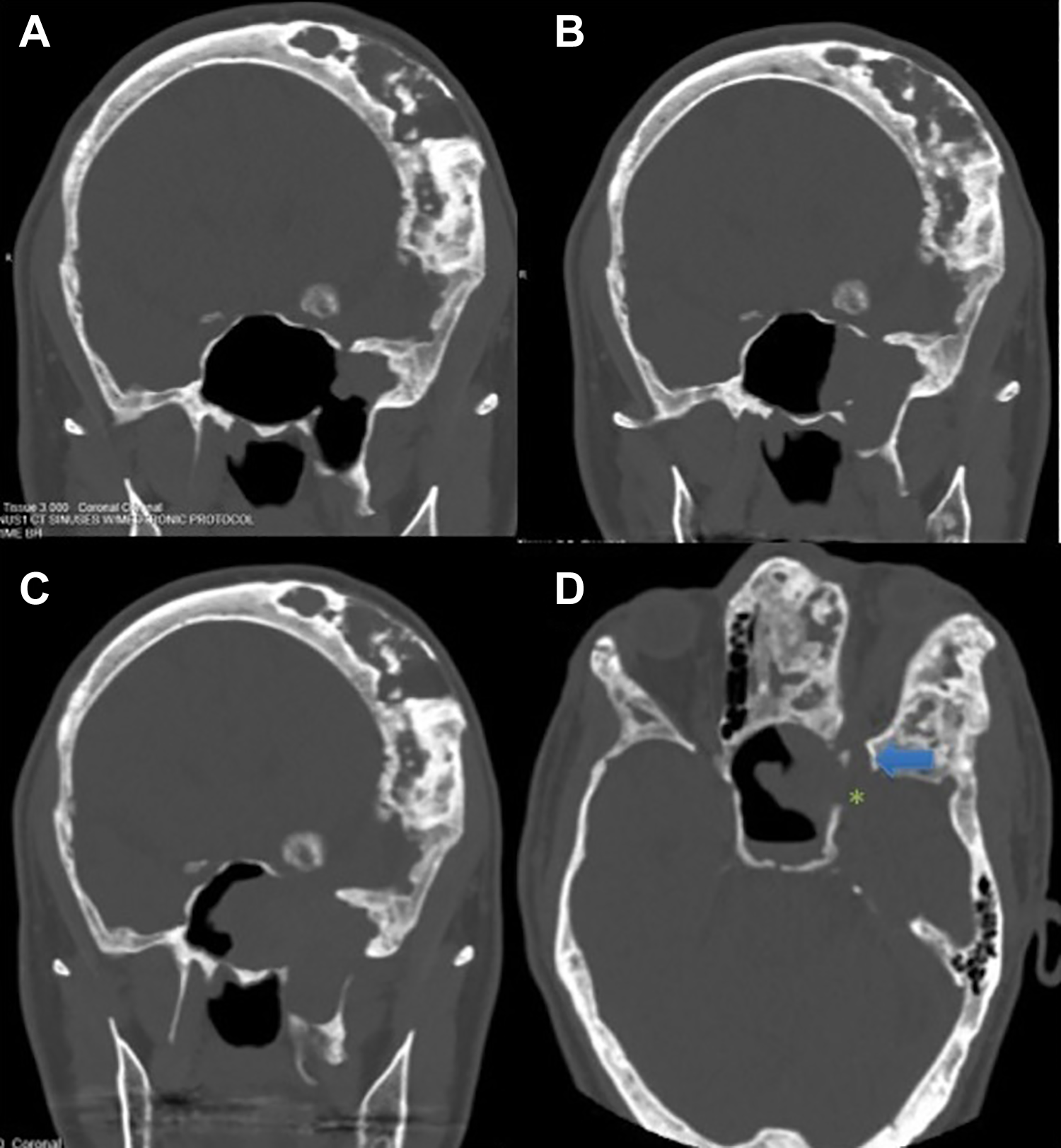
Coronal CT of patient 13 months before presentation (A), 3 months before presentation (B), and time of presentation. The soft tissue opacification in the left lateral sphenoid recess had been stable for at least 3 years prior to growth as seen above. Axial scan (D) shows dehiscence of middle fossa (*) in the lateral sphenoid with communication with the superior orbital fissure (arrow). Demineralization of the optic strut medial to the superior orbital fissure is evident. CT indicates computed tomography.
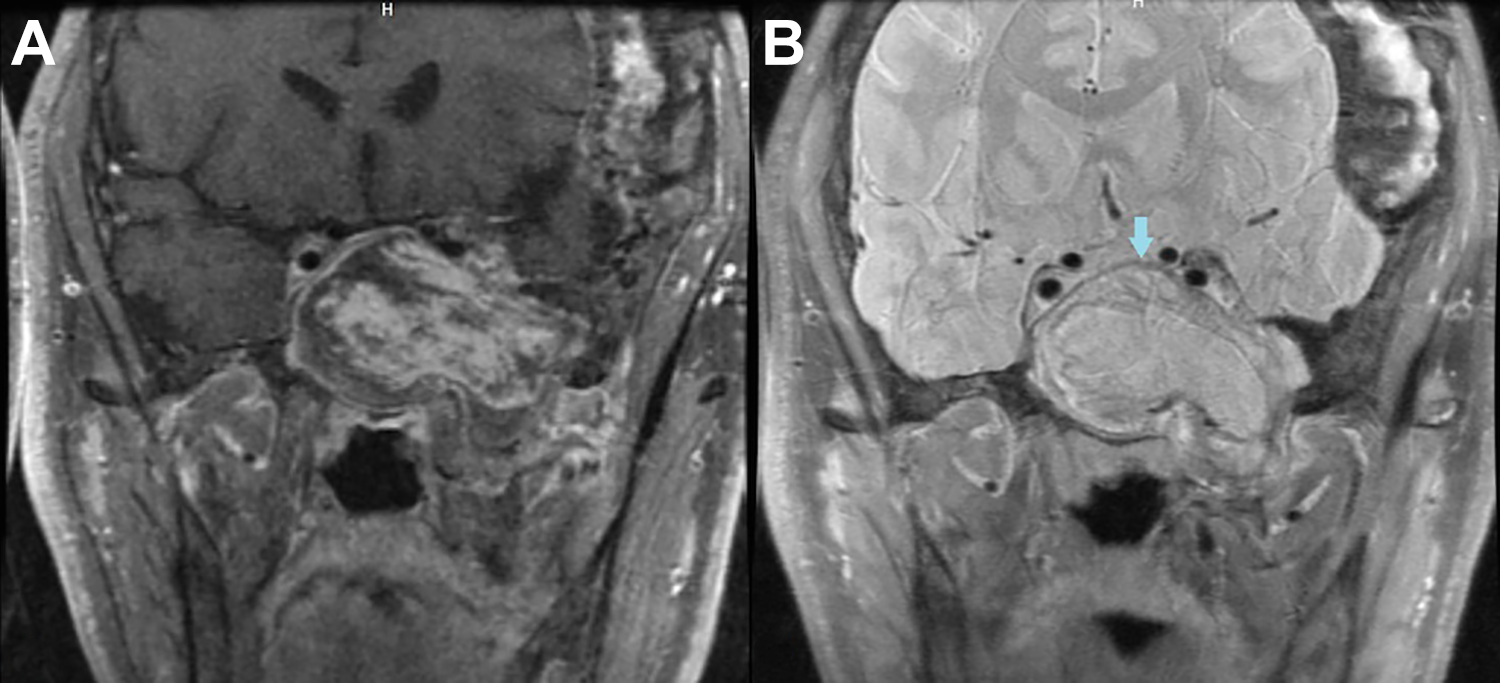
A, T1-weighted contrast-enhanced MRI with fat saturation shows papillary, frond-like enhancement of the sphenoid mass. B, T2-weighted MRI shows heterogeneous hyperintensity with rim of T2 dropout (arrow) in the periphery of the mass. MRI indicates magnetic resonance imaging.
The patient underwent endoscopic transsphenoidal biopsy of the sphenoid sinus mass by otolaryngology and neurosurgery. A posterior septectomy was performed. The left middle turbinate was partially removed, and extensive drilling was performed to remove the sphenoid rostrum. Intraoperatively, the mass was fragile, solid, and nodular with purple coloration. Dural pulsations from the middle fossa were evident but no cerebrospinal fluid (CSF) leak was encountered. Histopathology demonstrated acellular, necrotic material with organized hemorrhage.
The patient presented 8 months later with severe epistaxis and acute visual loss, OS. Ophthalmologic evaluation demonstrated light perception vision with complete inferior altitudinal visual defect OS. Urgent carotid angiography did not reveal any significant feeding vessels from the external carotid circulation. A branch of the left ophthalmic artery supplied the mass, which could not be safely embolized without risk to the parent vessel. He underwent expanded endonasal, 4 handed approach for maximal debulking of the vascular mass with decompression of the intracanalicular segment of the left optic nerve. The mass lesion was highly vascular and significant bleeding was encountered with debulking of the lesion intraoperatively (1000 mL), with active pulsatile vessels identified within the mass. Bleeding was controlled with combination of bipolar electrocautery and suction monopolar cautery, and the resection cavity was packed heavily with oxidized regenerated cellulose. No CSF leak was encountered. Ophthalmologic examination 2 months after the last surgery demonstrated significant improvement of vision (trace afferent pupillary defect, 20/60 OS with full visual fields). Fundus examination did show residual optic disc pallor.
Histopathology demonstrated predominantly organizing fibrin blood clot (Figure 3), and the final diagnosis was sphenoid sinus organized hematoma.
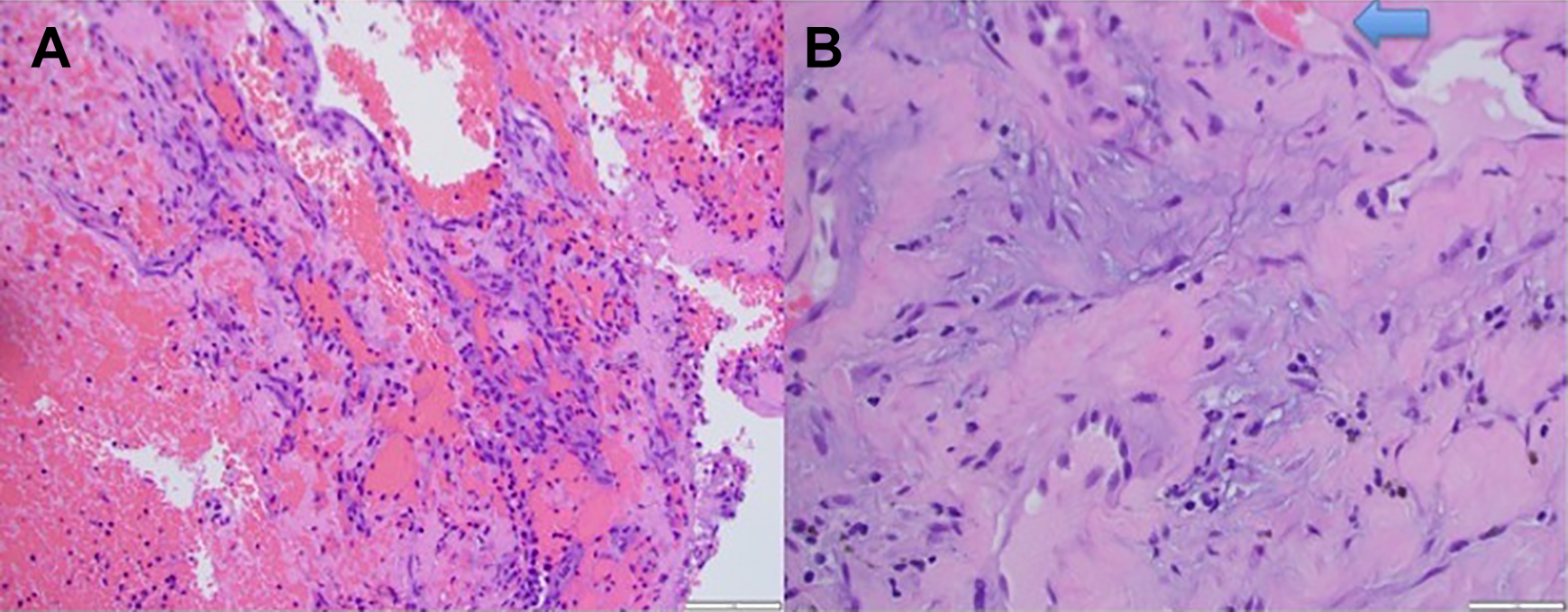
A, Histopathology shows fresh hemorrhage, with large population of erythrocytes mixed with polymorphonuclear leukocytes. B, Slide shows spindle fibroblasts admixed in fibrin, with capillary ingrowth (arrow), which is a feature of organization.
Written consent was obtained from the patient for publication of the present case report, including publication of accompanying images.
Discussion
Sinonasal organized hematomas are difficult to diagnose secondary to its rarity and its aggressive radiologic appearance analogous to low grade malignancy. 3,11,12 The mean age of presentation in the largest series to date was 50 years, with most patients older than 40 years. 4 The maxillary sinus is by far the most common site reported in the literature. 3,4,7,8,13 The largest series by Pang et al 4 reported 84 cases of OH, with 82 occurring within the maxillary sinus and 2 in the nasal cavity. Organized hematoma within the sphenoid sinus is extremely rare, with only 4 cases reported to date (Table 1). 1,7,14,15
Cases of Sphenoid Sinus Organized Hematoma Reported in the Literature With Details.
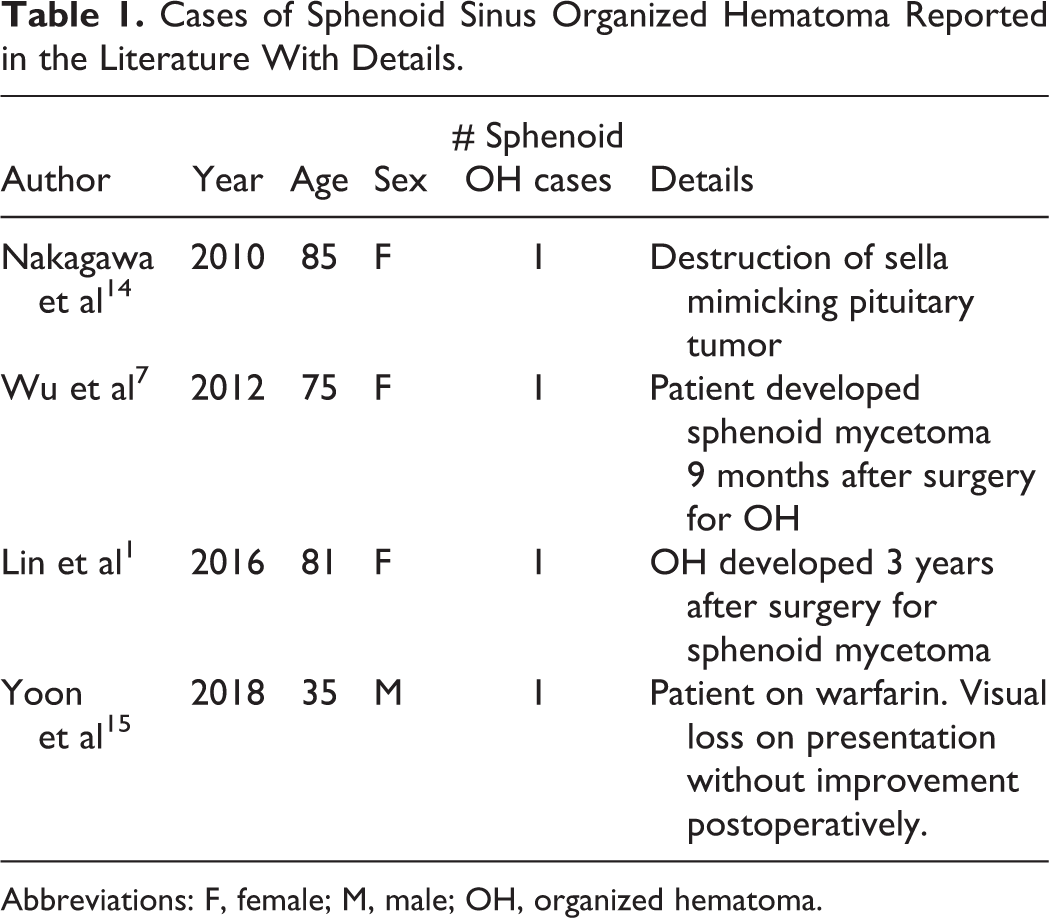
Abbreviations: F, female; M, male; OH, organized hematoma.
Typical CT appearance of sinonasal OH is hyperdense, with ground glass consistency without contrast administration. 7,16 There is usually bony expansion and remodeling of the involved sinus, and adjacent structures such as the orbit, pterygopalatine fossa, and infratemporal fossa can be deformed, 4 but typically without surrounding bony destruction. With intravenous contrast, OH on CT show papillary or frond-like enhancement, 16,17 as opposed to solid, nodular, and more heterogenous enhancement seen in malignancy. Organizing hematoma is generally well demarcated, distinguishing this pathology from malignant neoplasms. On MRI, OH are isointense to the inferior turbinate on T1-weighted images, with occasional additional foci of slight hyperattenuation. 2,16 T2-weighted images usually show a heterogeneous mass with mixture of hypointense and hyperintense signal intensity. Numerous authors 2,7,12,16 have suggested that the peripheral hypointense rim on T2-weighted images to be the most specific radiologic appearance on MRI. The “shell” of T2 drop out corresponds with the fibrous capsule of OH. On 18F-fluorodeoxyglucose (FDG)-Positron emission tomography/CT, OH typically demonstrates FDG uptake in the peripheral rim without central activity. 18 Differential diagnoses include inverted papilloma, mycetoma, mucocele, cholesterol granuloma, hemangioma, and low-grade malignancy.
Different etiologies of bleeding within the poorly ventilated sinus have been suggested as the initial inciting event in the pathogenesis of OH, with eventual organization of the accumulated blood including neovascularization and fibrosis. One theory involves vascular compromise from angiomatous polyps, 19 but this theory seems unlikely to be the major cause, as polyps are not consistently reported in other cases series and reports in the literature. Prior head and neck and sinus surgery has also been suggested as a possible contributing etiology, 4,7 including dental implantation. 3 In addition, there is association with antiplatelet medication, anticoagulation, and bleeding diathesis in the literature. Bleeding diathesis was first reported by Ozhan et al, 9 who postulated that von Willebrand disease contributed to development of a maxillary sinus OH. One patient with sphenoid sinus OH was taking warfarin for valvular heart disease. 15 Choi et al 5 reported on 17 cases, and all patients older than 60 years were taking aspirin. However, this is a minority of the case series (6/17 patients). Only 5% of patients with OH in the literature review of 75 patients were on aspirin. 5
The above case represents the first case in the literature of acute blindness from sphenoid sinus OH with partial but significant recovery of vision after endoscopic surgery. Our patient also had active arterial bleeding intraoperatively from within the mass, which had not been reported in the past. The highly vascular tissues from severe FD were the most likely cause of bleeding in this case, giving further credence to vascular compromise as part of the pathogenesis of OH. Based on the rebleeding and growth of the mass after initial surgery, we believe that OH does not develop from a single bleeding event but instead from recurrent bleeding leading to growth and expansion. The abundant intralesional and pulsatile bleeding encountered intraoperatively suggest repeated arterial bleeding within an obstructed sinus as a plausible cause of sinonasal OH, perhaps from an aberrant feeding vessel.
We radiographically document semirapid growth of OH within a 10-month period from a focus of soft tissue density of the lateral sphenoid recess that had been stable for 4 years, with further expansion and progressive middle fossa erosion over 3 more months. In the 2 largest case series in the literature, the median symptom onset prior diagnosis was 1 month in one report 5 and 18 months in another, 4 with wide range reported in both. Our case suggest that OH develops over months time, and failure to identify the source of bleeding may lead to further growth and recurrence.
Conclusion
Sphenoid sinus organized hematoma should be included in the differential diagnosis of expansile, enhancing sphenoid mass. Patients can present with acute blindness, and urgent surgery may save vision in selected cases.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.