
Abstract
Approximately 7 cases of spontaneous regression of adult laryngeal carcinoma have been published in the literature since 1900. This case presents a 62-year-old male with a 6-month history of hoarseness who was subsequently diagnosed with a T1aN0M0 left true vocal fold squamous cell carcinoma (SCC) after biopsy. One month following the initial biopsy, histopathological findings on repeat biopsy revealed absence of malignancy and regression of the tumor without radiation. There has been no evidence of tumor recurrence. This case exemplifies how innate immune modulation may play a role in the spontaneous regression of laryngeal SCC, although the mechanism remains unknown.
Introduction
Spontaneous regression of carcinoma of the larynx after inadequate therapy is exceptionally rare. To our knowledge, 7 cases of spontaneous regression of adult laryngeal carcinoma have been published in the literature since 1900. 1 Spontaneous regression of cancer is the partial or complete disappearance of a malignant tumor in the absence of all treatment, or in the presence of therapy, which is considered inadequate to exert a significant influence on neoplastic disease. 2 We report a case of spontaneous regression of laryngeal squamous cell carcinoma (SCC) after small focal biopsies and consider how immune modulation may play a role.
Case Report
A 62-year-old male presented with a 6-month history of hoarseness. He denied any history of smoking or alcohol use. The patient admitted to vocal fatigue, frequent throat clearing, and felt as if his voice was gradually worsening, greatly affecting his work as a minister. He had initially been treated for allergic rhinitis by his primary care physician, but the hoarseness persisted. In retrospect, the patient recalled a coughing paroxysm with exposure to potpourri shortly before his hoarseness began.
On initial evaluation, he exhibited vocal roughness and strain, with a Voice Handicap Index (VHI) of 36, indicating a moderate level of handicap. Laryngeal videostroboscopy (LVS) revealed an exophytic, leukoplakic lesion of the membranous left true vocal fold (TVF) with absent mucosal wave. Given these findings, a concern for malignancy was discussed, and the patient was scheduled for biopsy of the lesion.
One week later, direct microlaryngoscopy (MDL) under general anesthesia revealed a thick exophytic, bulky, irregular mucosal mass that extended from the left vocal process to, but not involving, the anterior commissure (Figure 1). There was no involvement of the contralateral TVF, ventricles, infraglottic region, or false vocal folds. The mass was palpated with a blunt-tip probe and thought to be indurated, concerning for carcinoma. It was then biopsied away from the medial edge with a small 3-mm cupped biopsy forceps. A tissue specimen was sent for permanent pathology evaluation.
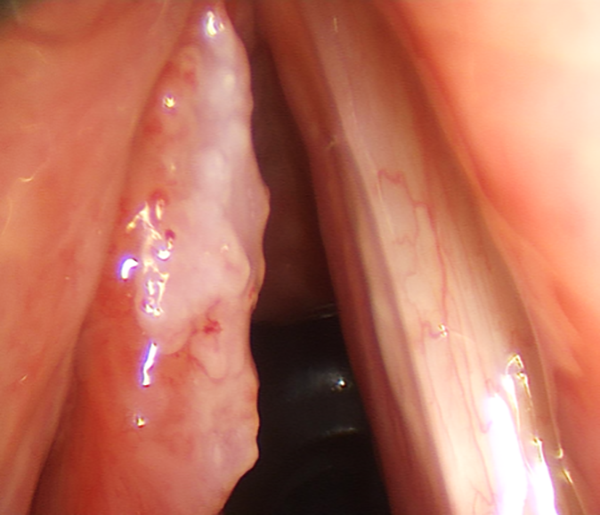
Initial direct microlaryngoscopy, revealing a thick exophytic, bulky, irregular mucosal mass that extended from the left vocal process to, but not involving, the anterior commissure.
Pathologic examination of the six 1 to 2 mm pieces of biopsy tissue showed extensive SCC in situ with rare foci of stromally invasive keratinizing type SCC (Figure 2). This was also confirmed by a second academic institution’s review of the pathology. Their evaluation included an additional report stating the tumor was p16 negative by immunohistochemistry and it was high-risk human papillomavirus negative by DNA in situ hybridization. Neck computed tomography (CT) with contrast revealed normal appearance of the true and false vocal folds and a thin anterior commissure. Chest CT with contrast revealed nonspecific subcentimeter mediastinal lymph nodes and pulmonary nodules. The patient was diagnosed with a T1aN0M0 left TVF SCC.
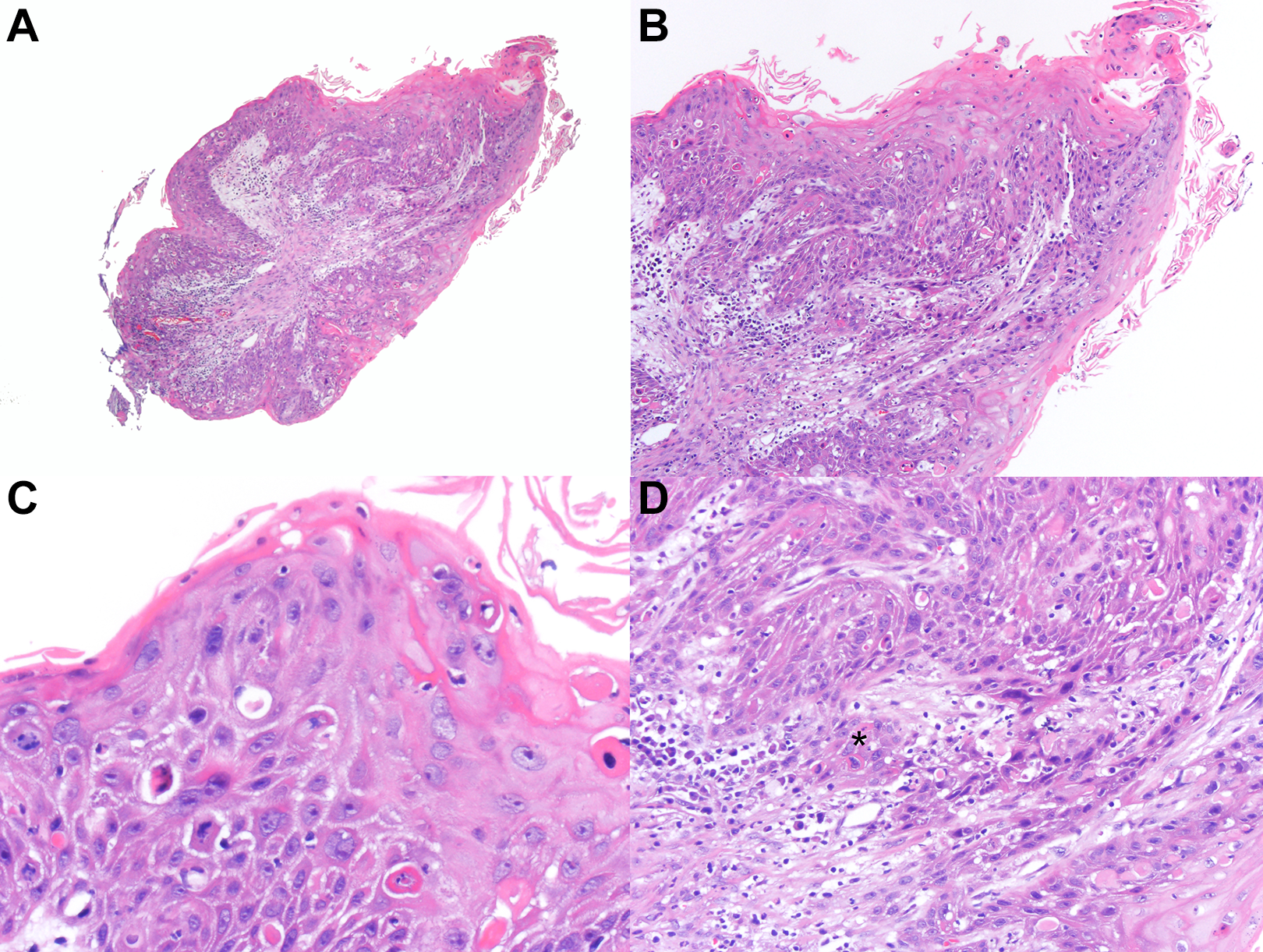
Histopathologic features of the primary diagnostic laryngeal biopsy specimen. A, Exophytic, slightly papillomatous, and very thick, hyperkeratotic squamous epithelium with atypia and irregular rete (×4 magnification). B, Hyperkeratotic squamous epithelium with disordered maturation including large cells with angulated, hyperchromatic nuclei in the mid to upper layers and a very irregular rete pattern with angulated edges concerning for invasive carcinoma (×10 magnification). C, High-power shoring the nuclear pleomorphism and angulation along with numerous dyskeratotic cells (×40 magnification). D, Focus of superficially invasive squamous cell carcinoma where a nest (asterisk) has broken away from the surface epithelial in situ component (×20 magnification).
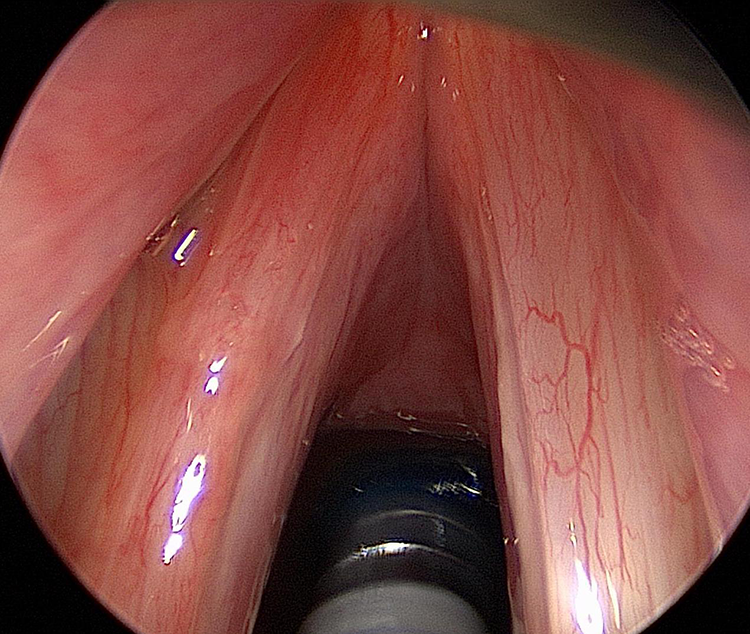
After the treatment options of endoscopic surgical excision with cordectomy versus primary radiation were discussed, the patient elected for radiation. Two weeks after MDL, the patient presented to a radiation oncologist in his home community in another state for pretreatment planning. Of note, the patient noted significant improvement in his voice since the biopsy and repeat clinical examination by a laryngologist revealed significant improvement as well (Figure 3). There was almost complete regression of the exophytic SCC. In considering perioperative factors that may have played a role in his clinical course, the patient reported being diagnosed with influenza shortly after the biopsy. He completed a course of oseltamivir. Prior to his cancer diagnosis, the patient had been taking Protandim, a non-Food and Drug Administration (FDA)-approved herbal supplement purported to prevent and/or treat numerous medical diseases. Subsequent to his diagnosis, he had doubled the dose of this supplement. The FDA has since issued a formal warning to the company due to not labeling its product as a drug, yet claiming Protandim “help[s] fight against cancer.” 3 Lastly, the patient endorsed a spiritual contribution from added prayers from his local church congregation.

Flexible transnasal laryngoscopy 2 weeks after the biopsy revealing almost complete regression of the exophytic squamous cell carcinoma (SCC).
Three weeks after the patient presented to radiation oncology with noted regression of the SCC, the patient was brought back to the operating room for MDL to examine the left TVF under high magnification. It was nearly normal in appearance (Figure 4). There was a small focal area of mucosal irregularity on the left superior surface that measured approximately 2 mm × 1 mm, which was excised in its entirety with microflap phonomicrosurgery techniques. Histopathological examination of the removed tissue reported inflamed squamous mucosa with reactive and regenerative changes that were negative for malignancy.
Examination of the left true vocal fold (TVF) under high magnification after the patient presented with noted regression of the squamous cell carcinoma (SCC), revealing a near normal appearance.
The patient was closely followed in clinic to assess for recurrence. Less than a month after surgery, the patient scored and maintained a VHI of 0. The left TVF was near normal in appearance on physical examination, and successive LVS revealed continued improvement of mucosal wave. The patient continues to have no vocal changes or complaints after 8 years of follow-up, and flexible transnasal laryngoscopy reveals normal vocal fold mobility with no evidence of disease (Figure 5).

Flexible transnasal laryngoscopy 8 years after follow-up revealing normal vocal fold mobility with no evidence of disease.
Discussion
The mechanism of spontaneous regression of malignant tumors remains uncertain; however, several hypotheses on this topic have been proposed. Some of these hypotheses include immune modulation of the host, activated by local trauma or necrosis/devascularization via biopsy, locoregional infection, or prolonged pyrexia.2,4,5 Moreover, possible influential factors contributing to these hypotheses include fever and/or infection, allergic or immune reactions, endocrine influence, unusual sensitivity to routine inadequate therapy, interference with nutrition of the tumor, or removal of carcinogenic agent. 1 A primary hypothesis is that an immunological response can be initiated after trauma to the area, such as biopsy. 6 In a study of 176 cases of spontaneous regression of cancer by Everson and Cole, 40% of those cases were thought to be associated with operative trauma. 6 Butterfield expands on this theory by suggesting that trauma or surgery to the area leads to antitumor immunity, ultimately having “cancer vaccine effects.” 7 It is postulated that this antitumor immunity occurs by the release of dying tumor cells during the procedure or an increase in the expression of tumor antigens, which leads to the formation of antitumor immunity. 7 It is possible that in this case biopsy to the cancerous area led to an antitumor immune response, causing regression of the remaining tumor. The “cancer vaccine” hypothesis further suggests the potential of antitumor treatment modalities that can be significant in the treatment and cure of cancer.
Additionally, the patient reported a case of influenza following the biopsy, suggesting the role of immune modulation or local inflammatory response in the regression of the laryngeal carcinoma. William Coley studied the role of innate immunity in the cure of cancer by using heat-killed bacteria to induce a state of pyrexia, leading to complete regression of the tumor. 8 While the mechanism of action of microbial therapy is not clearly understood, it is hypothesized that the activation of the host immune system causes an antitumor cytokine-mediated response. 8 As research in this field continues, Bacillus Calmette-Guerin has been approved by the FDA for the treatment of superficial, nonmuscle invasive bladder cancer, and investigators have demonstrated the efficacy of live attenuated bacterial cells to kill tumor cells in vitro and in rodents. 8 Additionally, positive results were obtained using bacterial genetics and in vivo imaging. 8 Furthermore, there was a case of spontaneous regression of metastatic melanoma shortly after a febrile illness secondary to the tetanus–diphtheria–pertussis vaccine, suggesting the role of viral markers in tumor regression. 9 This case of spontaneous regression of laryngeal SCC further supports the study of innate immunity and microbial therapy in the treatment of cancer and implies a possible role of these therapies in laryngeal cancers and other cancers of the head and neck.
Of note, the patient was a preacher, which also suggests a theoretical role of faith healing. While it would be extremely difficult to prove a connection between prayer and the spontaneous regression of cancer, there has been a randomized controlled trial published in the literature, showing the positive effects of prayer on outcomes in patients admitted to the coronary care unit. 10 Additionally, to our knowledge, the literature mentions 3 other cases of a connection between prayers and the spontaneous regression of cancer. 11 Lastly, the patient was taking Protandim, which suggests the hypothetical role of herbal therapy.
After 8 years of follow-up, the patient continues to show no evidence of disease. The length of patient follow-up is considerable, and there has not been recurrence of any mucosal abnormality demonstrating complete and irreversible regression of the tumor, as well as definitive cure of the patient. This case is significant because it adds a rare case of spontaneous regression of laryngeal SCC after biopsy to the literature and exemplifies the possibility that immunotherapy may have a significant role in the treatment of carcinoma.
Footnotes
Authors’ Note
This article was presented as a Triological Society Poster at the 122nd Annual Meeting at COSM, Austin, TX, May 1-5, 2019.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.