
Abstract
Objectives:
Tracheal stenosis is defined as a narrowing of the airway distal to the lower edge of the cricoid cartilage. It is initially diagnosed based on clinical presentation and then confirmed using direct laryngobronchoscopy. Other adjunctive diagnostic methods, including spirometry, have been proposed. This study aimed to evaluate the relationship between tracheal stenosis severity and pre- and post-balloon dilatation spirometry parameters in order to assess for significant changes in spirometry values and to evaluate for the effects of stenosis-associated factors on post-dilation spirometry values, including vertical length and grade of the stenosis, as well as the role of wound-modifying agents.
Methods:
This retrospective study included adults (>18 years of age) with isolated tracheal stenosis who underwent endoscopic balloon dilations at King Saud University Medical City from June 2015 to May 2019, with detailed documentation of operative findings and valid spirometry measurements pre- and post-balloon dilation. Basic demographic data and operative note details, including information about the percentage of tracheal stenosis, distance of tracheal stenosis from vocal cords, vertical length of stenotic segment, and use of wound-modifying agents (topical mitomycin C or triamcinolone injections), were extracted.
Results:
Fourteen patients with spirometry measurements obtained on 50 occasions (25 pre-balloon dilation and 25 post-balloon dilation) were included. Each 1-unit increase in the vertical length of the stenosis showed a statistically significant negative relationship (−1.47 L/s) with pre-balloon dilation peak expiratory flow (PEF; P = .034). Post-balloon dilation spirometric values showed statistically significant improvements for most variables.
Conclusions:
The vertical length of an isolated tracheal stenosis can be predicted before surgical interventions using PEF values and may be a significant indicator of anticipated post-balloon dilation surgical success. Our study suggested that spirometry is a very useful technique for evaluating patients with tracheal stenosis due to its noninvasiveness, cost-effectiveness, with a good clinical value.
Introduction
Tracheal stenosis is defined as a narrowing of the airway distal to the lower edge of the cricoid cartilage. In adults, there are several causes of tracheal stenosis, including post-intubation trauma, long-term tracheostomies, infections, systematic inflammatory conditions, and neoplasias.1,2
Tracheal stenosis is generally a relatively late sequela of an initial pathological process and may not be recognized until symptoms of airway compromise are already present, including stridor, respiratory distress, apnea, cyanosis, or hoarseness. Diagnosis of tracheal stenosis is typically determined on the basis of history, clinical examination, and other noninvasive testing modalities, including computed tomography (CT), pulmonary function testing (PFT), and, more recently, multiplanar reformatting, and 3-dimensional reconstruction CT. A final diagnosis can be made via a bronchoscopy for evaluation of the airway.3-5
The role of PFTs in evaluating patients with upper airway obstruction (UAO) was first investigated in the early 1970s,1,6,7 with studies reporting its many benefits, including low cost, noninvasiveness, and easy accessibility.8,9 In the 1970s, Empey first introduced the Empey index, 6 which was defined as the forced expiratory volume in 1 second (FEV1) divided by the peak expiratory flow (PEF). This ratio was significantly higher in patients with UAO than in control patients and in patients with lower airway obstruction, with an FEV1/PEF ratio of more than 10 (mL/L/min) in the UAO group. Consequently, Nouraei et al 10 studied PFT values in upper airway stenosis subgroups, including tracheal stenosis patients, using a nonlongitudinal protocol and the derived expiratory disproportion index (EDI), which is the ratio of FEV1 to PEF (EDI = FEV1[L]/PEF[L/s] × 100).
In the literature, the sensitivities and specificities of spirometric values as indicators for surgical interventions in subglottic stenosis patients ranged between 55% to 86% and 62% to 83%, respectively, with higher sensitivities and specificities noted for PEF, total peak flow (TPF), peak inspiratory flow rate, and EDI.11,12 When comparing patients with laryngotracheal stenosis and those without stenosis, including healthy controls and patients with lung diseases, the sensitivities and specificities were as high as 95% and 94%, respectively. 10 Evidence has been reported to support the use of PEF, EDI, and other spirometric parameters for initial evaluations and for monitoring of suspected laryngotracheal stenosis cases, particularly those with subglottic stenosis.10-16
Management strategies for tracheal stenosis include open techniques with laryngotracheal reconstructions, cricotracheal resections, tracheal resections with end-to-end anastomoses, and slide tracheoplasties; endoscopic techniques, including balloon dilations; and adjuvant therapies, including intralesional steroid injections and topical mitomycin C (MMC) applications, though the role of these wound-modifying agents remains controversial.15,17-21
This study aimed to evaluate the relationship between tracheal stenosis severity and pre- and post-balloon dilation spirometry parameters in order to assess for changes in spirometry values; to evaluate for the effects of stenosis-associated factors, including vertical length and grade of the stenosis, on post-dilation spirometry values; and to clarify the role of wound-modifying agents in the management of these patients, using spirometry parameters as objective indicators of their effects.
Patients and Methods
This retrospective study included adults aged >18 years with isolated tracheal stenosis who underwent endoscopic balloon dilation surgeries at the Otolaryngology-Head and Neck Department of the King Saud University Medical City in Riyadh, Saudi Arabia from June 2015 to May 2019, with detailed documentation of operative findings and valid spirometry measurements pre- and post-balloon dilation. Prior to initiation of this study, approval was obtained from the institutional review board (Project No. E-19-4039). The confidentiality of identifiable patient records was maintained at all times, and patient data were collected through E-Sihi (Cerner electronic health records system, Riyadh, Saudi Arabia).
For this study, isolated tracheal stenosis was defined as a stenosis distal to the cricoid cartilage without other airway stenosis, as described in the operative note. We excluded patients with tracheostomies, airway stenosis with multilevel involvement, incomplete clinical documentation, missed clinical follow-up, suspected inconsistencies in spirometric results (eg, nonrepeatable records or patients with low cognitive abilities who could not follow the instructions), parenchymal lung diseases, or active smokers.
Demographic data, including patient sex, age, height, weight, and body mass index (BMI); stenosis etiology; and smoking history were documented. Decisions about surgical interventions were mainly based on patients’ signs and symptoms. All patients underwent endoscopic evaluations and radial incisions using a Cold Steel technique, followed by a balloon dilation using a 15-mm balloon dilation catheter (CRE, Pulmonary Balloon Dilation Catheter, Boston Scientific Co) 3 times for 40 to 60 seconds depending on the patient’s condition. The decision to use MMC or triamcinolone was based on surgeon preference. The MMC concentration used in this study was 4 mg/mL in a total of 2.5 mL soaked on a cottonoid patty for 4 minutes. Triamcinolone injections of 40 mg/mL were used.
Operative notes were reviewed, and relevant information was extracted, including the percentage of the isolated tracheal stenosis, distance of the tracheal stenosis from the vocal cords, vertical length of the stenotic segment, and the use of wound-modifying agents (MMC application or triamcinolone injection).
Pre-balloon dilation spirometry was performed within 2 weeks prior to the intervention, and post-intervention spirometry was conducted without a fixed time during patient follow-up. We exclusively included spirometric results that were repeatable and fulfilled the recent acceptability criteria of the American Thoracic Society (ATS) guidelines. 22 Stenosis severity was stratified into 4 grades using the Cotton-Myer grading system, in which a grade I stenosis referred to a narrowing of the lumen by up to 50%; grade II, a narrowing of 51% to 70%; grade III, a narrowing of 71% to 99%; and grade IV, no detectable lumen. 23 The vertical length of the stenosis was also used as a severity indicator and was classified as <1, 1 to 2, and > 2 cm.
Statistical Analysis
Data analysis was conducted using R software, version 3.6.2. 24 Data are expressed as mean ± standard deviation (SD) for continuous variables and counts with percentages for categorical variables. Multivariate analysis was performed using generalized least squares. Generalized least squares with autoregressive covariance structure or compound symmetry (based on model fit) was used to analyze the associations of the Cotton-Myer grade, vertical length of stenosis, and use of topical MMC or triamcinolone injections with the final postoperative spirometry results. Baseline preoperative values were used as covariates in the model. Generalized least squares was used to account for multiple measurements per patient. The same methodology was used to assess the associations of these parameters with preoperative spirometry values. Preoperative and postoperative values were compared using paired t tests. Hypothesis testing was performed at a 5% level of significance.
Results
Fourteen patients (28.6% females and 71.4% males) met the study inclusion criteria and underwent spirometry measurements on 50 occasions (25 pre-balloon dilation and 25 post-balloon dilation). The mean age of the included participants was 31.1 ± 12.9 years. The average weight and height of the included participants were 73.3 ± 16.5 kg and 167 ± 9.95 cm, respectively, with a mean BMI of 26.4 ± 6.02 kg/m2. The most frequent etiology for stenosis was post-intubation trauma (78.6%). Comorbidities included diabetes (21.4%), ischemic heart disease (7.14%), papillary thyroid cancer (7.14%), and bronchial asthma (14.3%). Mitomycin C and triamcinolone were used in 78.6% and 42.9% of cases, respectively. Exsmokers represented 21.4% of the study sample (Table 1).
Descriptive Statistics for the Study Sample.a
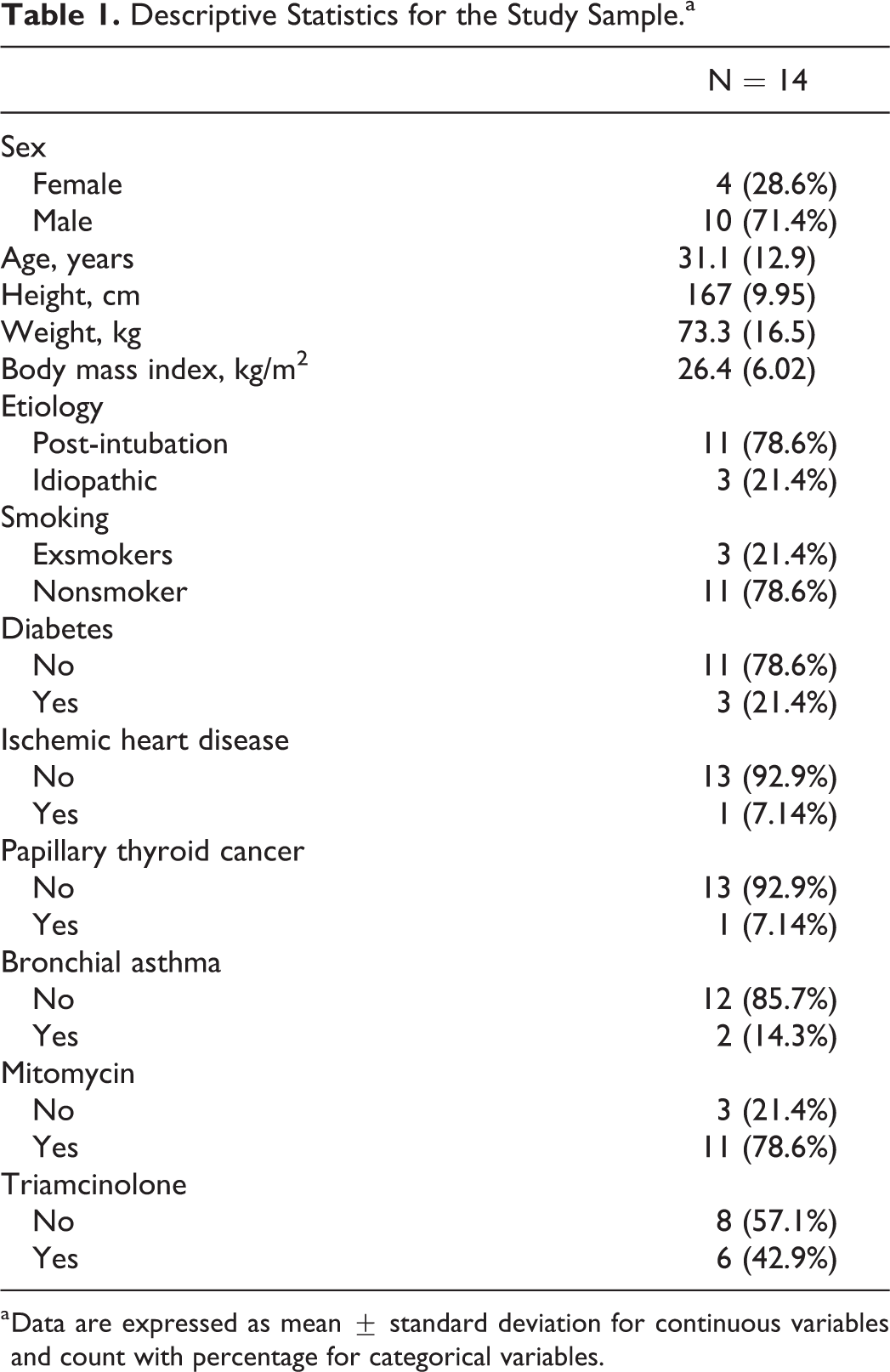
a Data are expressed as mean ± standard deviation for continuous variables and count with percentage for categorical variables.
Spirometry values were expressed as mean ± SD. Statistical analysis showed that the forced vital capacity (FVC) and forced expiratory flow (FEF) 75% were not significantly different before and after the intervention (P = .267 and P = .25, respectively). After the intervention, FEV1 significantly increased from 1.78 ± 0.60 L to 2.15 ± 0.79 L (P = .018); PEF significantly increased from 2.68 ± 2.33 L/s to 3.84 ± 2.33 L/s (P = .005); and FEV1/FVC (FEV1% F) significantly increased from 60.90% ± 17.5% to 70.60% ± 18.15 (P = .034). FEF 25% and FEF 50% values were both significantly higher than pre-intervention values (P = .002 and P = .001, respectively). The average post-intervention value for maximum midexpiratory flow (MMEF) was 2.37 ± 1.48 L/s, which was also significantly higher than the pre-intervention average value of 1.6 ± 0.78 L/s (P = .005). The average EDI significantly decreased post-intervention (82.1 ± 21.9 vs 71.2 ± 23.9, P = .045). These results indicated favorable changes in spirometry results after the intervention (Table 2).
Spirometry Values Before and After Intervention.a
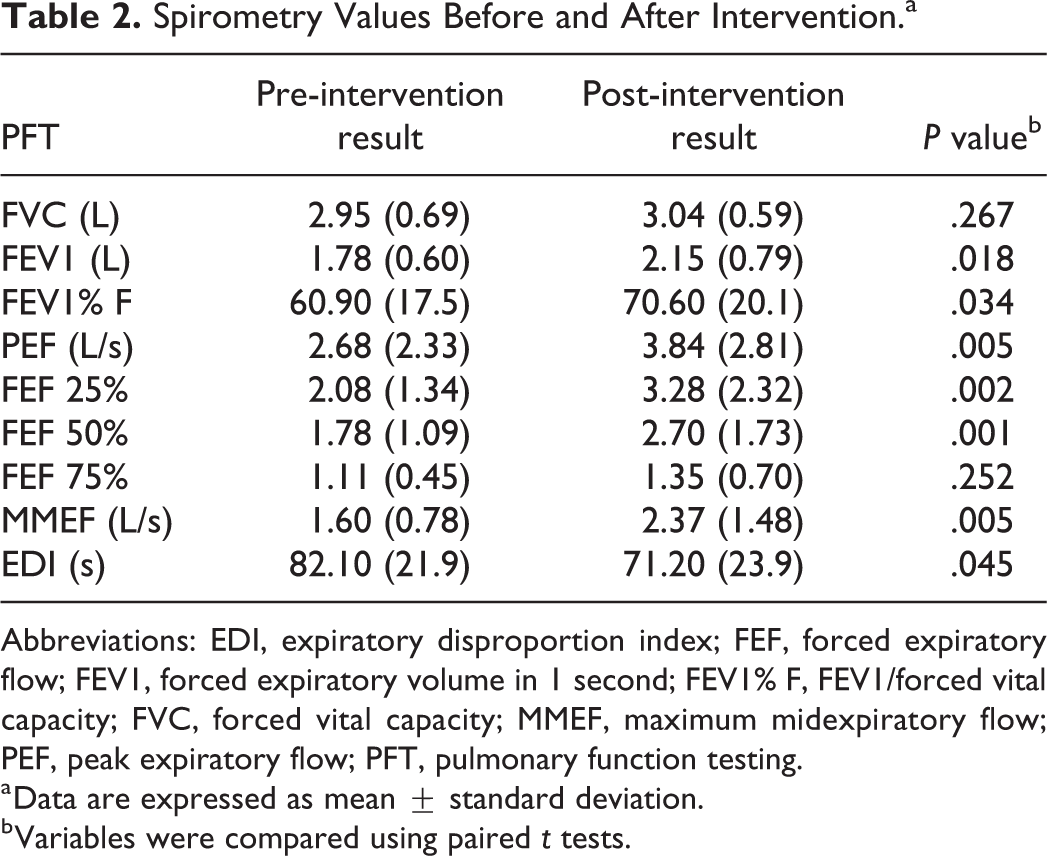
Abbreviations: EDI, expiratory disproportion index; FEF, forced expiratory flow; FEV1, forced expiratory volume in 1 second; FEV1% F, FEV1/forced vital capacity; FVC, forced vital capacity; MMEF, maximum midexpiratory flow; PEF, peak expiratory flow; PFT, pulmonary function testing.
a Data are expressed as mean ± standard deviation.
b Variables were compared using paired t tests.
We also assessed the correlation of different pre-intervention spirometric parameters with the vertical length and grade of the tracheal stenosis, as shown in Table 3. All the correlations were nonsignificant, except for the vertical length of the stenosis, which showed a statistically significant association with the pre-intervention PEF (Table 3).
Factors Associated With Pre-Intervention Spirometry Values.
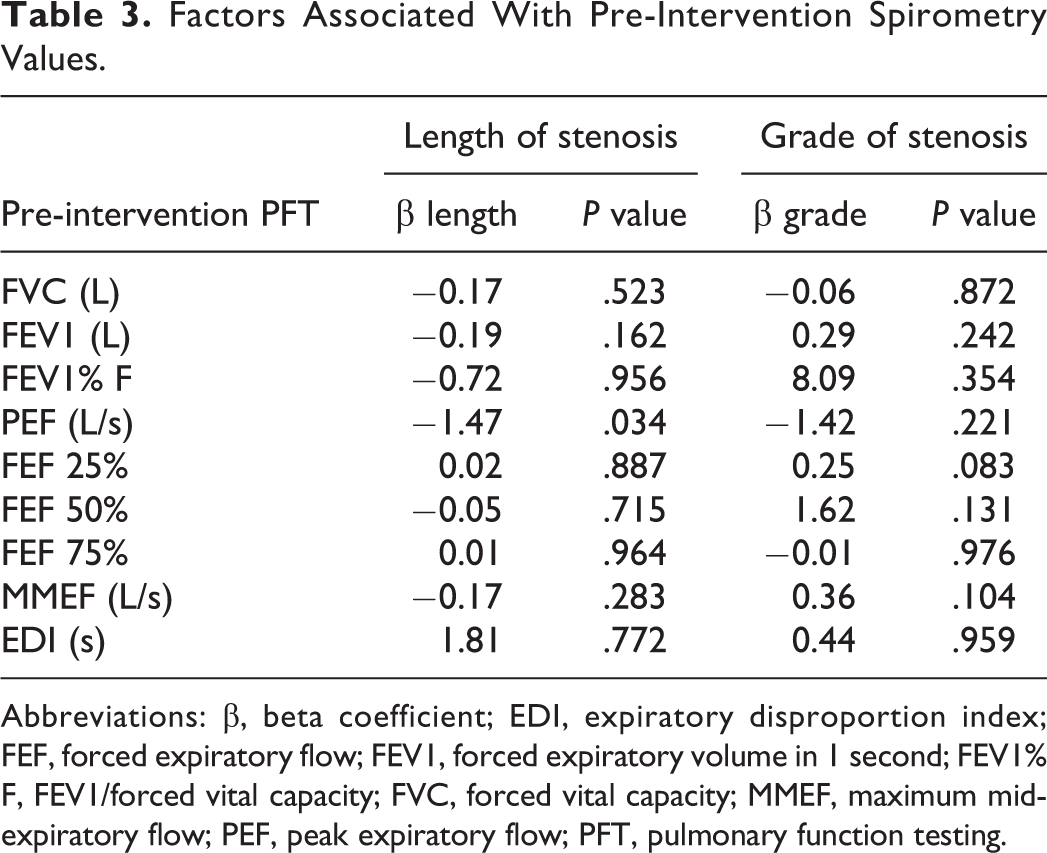
Abbreviations: β, beta coefficient; EDI, expiratory disproportion index; FEF, forced expiratory flow; FEV1, forced expiratory volume in 1 second; FEV1% F, FEV1/forced vital capacity; FVC, forced vital capacity; MMEF, maximum midexpiratory flow; PEF, peak expiratory flow; PFT, pulmonary function testing.
Post-intervention FVC, FEV1, FEV1% F, FEF50%, and MMEF values showed statistically significant associations with the vertical length of the stenosis (P values = .042, .003, <.001, .022, and .026, respectively), and post-intervention average values could be predicted in relation to a 1-unit increase in the vertical length of the stenosis (estimated effects of −0.24, −0.36, −12.3, −0.91, and −0.82, respectively). Topical use of MMC was significantly associated with FEV1 and FEV1%, with expected post-intervention improvements of 0.68 L and 20.13%, respectively. Triamcinolone injections were significantly associated with FVC and FEV1, with expected improvements in post-intervention values of 0.53 and 0.45 L, respectively (Table 4).
Factors Associated With Post-Intervention Spirometry Values.
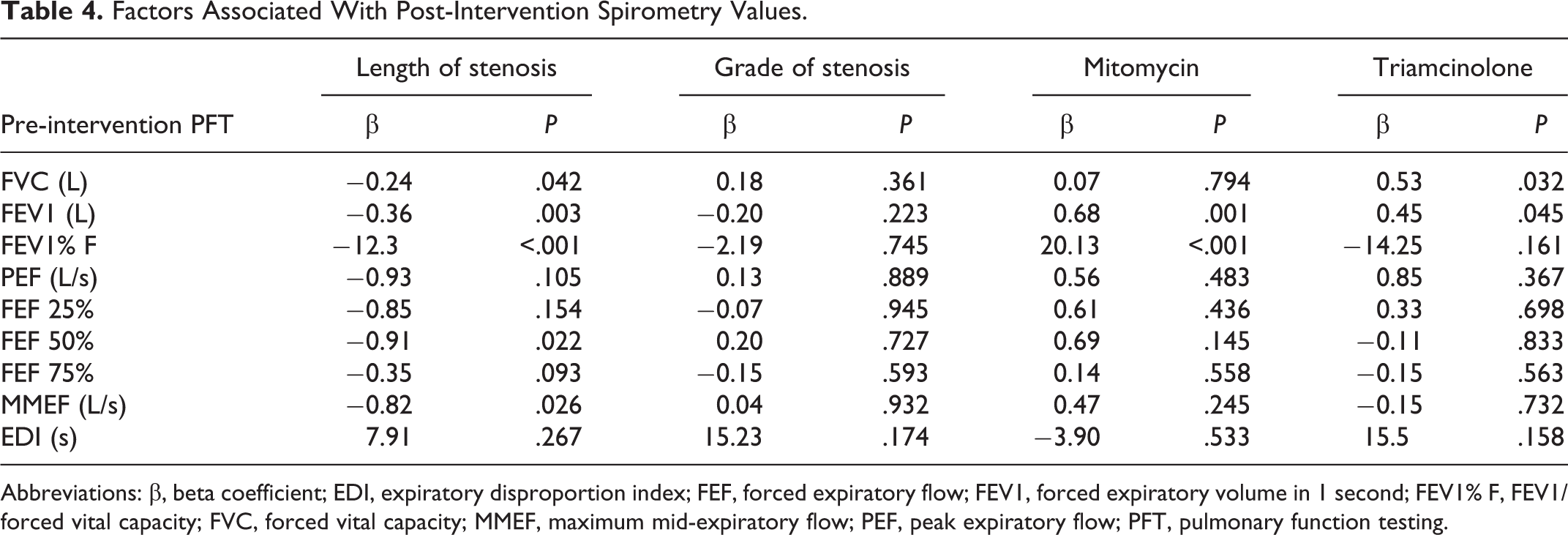
Abbreviations: β, beta coefficient; EDI, expiratory disproportion index; FEF, forced expiratory flow; FEV1, forced expiratory volume in 1 second; FEV1% F, FEV1/forced vital capacity; FVC, forced vital capacity; MMEF, maximum mid-expiratory flow; PEF, peak expiratory flow; PFT, pulmonary function testing.
Discussion
Tracheal stenosis is a distinct entity from subglottic stenosis, and its correlations with flow-volume loop spirometry parameters have not yet been investigated. It is important to clarify the relationship between spirometric parameters and isolated tracheal stenosis for improved diagnosis, monitoring, and prognosis of this condition and for comparisons of different surgical treatment modalities.
We observed that the pre-dilation PEF showed a statistically significant (P = .034) association with the vertical length of the stenosis. Each incremental 1-unit increase in the vertical length of the tracheal stenosis was associated with 1.47 L/s decrease in the average expected pre-dilation PEF. Interestingly, the grade of the stenosis did not correlate with the pre-dilation spirometry values, a finding that has also been reported in subglottic stenosis patients by Abdullah et al. 14 In comparison, Carpenter et al 11 identified cutoff values for PEF, EDI, and TPF, without overlap of the results among subglottic stenosis grades.
There were statistically significant improvements in most spirometry parameters after dilation, including FEV1, FEV1% F, PEF, FEF 25%, FEF 50%, MMEF, and EDI, with similar findings previously identified in patients with subglottic stenosis who underwent dilations.11-14
We determined that the vertical length of the stenosis was significantly associated with the post-dilation values for FVC, FEV1, FEV1% F, FEF 50%, and MMEF (P = .04, .003, <.001, .022, and .026, respectively). Expected average reference spirometry values could be predicted if the vertical length of stenosis was known, with a post-dilation FVC decrease of 0.24 L/s from the expected average FVC associated with an increase in the length of the stenosis by 1 unit. The expected average post-dilation FEV1 decreased by 0.36 L for each 1-unit increase in the length of the stenosis, while a 1-unit increase in the length of the stenosis was associated with 12.3% decrease in the average predicted post-dilation FEV1% F. The predicted average post-dilation FEF 50% value was expected to decrease by 0.91 L/s for each 1-unit increase in the length of the stenosis. The predicted average post-dilation MMEF value decreased by 0.82 L/s for each 1-unit increase in the length of the stenosis.
Use of wound-modifying agents, including either topical application of MMC or triamcinolone injection at the affected area, had different results. Topical MMC use was noted to have statistically significant effects on both FEV1 and FEV1% F (P = .001 and P < .001, respectively) compared to nonuse, while triamcinolone use was noted to have statistically significant effects on both FVC and FEV1 (P = .032 and P = .045, respectively) compared to nonuse. These differing results may reflect surgeons’ preferences or inconsistencies in the indications for use of these agents in tracheal stenosis patients, which may weaken the importance of these findings. The avoidance of topical MMC use in patients with a higher grade of stenosis may also have occurred due to the possibility of open reconstructive procedures in the near future.
It is important to note the role of the vertical length of the stenosis as a potential contributing factor to spirometry results and during assessments of improvement expectations in tracheal stenosis patients. Nouraei et al 17 evaluated the relationship between vertical length of a stenosis and the success of endoscopic balloon dilation procedures and found that more than 3 cm of stenosis length was associated with higher failure rates compared to shorter stenotic segments.
Limitations of this study included its retrospective design, which affected its causality, and its relatively small sample size. The rarity of finding patients with isolated tracheal stenosis made the total number of cases low. Because of the subjectivity nature of percentage of stenosis estimation with inter- and intra-rater variability might decrease its correlation to spirometry value. Spirometry is also a subject-dependent procedure, with variability in results from patient-to-patient and from time-to-time for the same patient. We exclusively selected those spirometry results that were repeatable, according to recent ATS guidelines. Patients without substantial improvement in results were also included in this study, which might have affected assessments of post-dilation improvements; however, this inclusion may also be considered a study advantage, as we continue to study the factors that cause a lack of improvement in spirometry values post-dilation.
In conclusion, the vertical length of an isolated tracheal stenosis can be predicted using PEF values before surgical intervention and may be a significant indicator of anticipated post-balloon dilation surgical success. Most post-intervention spirometry values showed statistically significant improvements when compared to pre-intervention values. Wound-modifying agents also showed significant associations, which may require further large-scale prospective trials for confirmation of their roles. These findings suggest that spirometry can be a very useful technique for evaluation of patients with isolated tracheal stenosis because it is noninvasive, cost-effective, and easily accessible, with a good clinical value that aids in the diagnosis and monitoring of patients after surgical interventions.
Footnotes
Acknowledgments
Special thanks to the support provided by King Saud University, Deanship of Scientific Research, College of Medicine Research Center.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.