
Abstract
Background:
Tonsillectomy is one of the most common surgical procedures in pediatric patients. The tonsillar retractor, which is routinely used during a tonsillectomy, applies high pressure to the patient’s tongue and can lead to various complications.
Aims:
This study aimed to explore tongue edema induced by the pressure applied by tonsillar retractor, using ultrasonography in pediatric patients undergoing tonsillectomy surgeries.
Materials and Methods:
Sixty-one patients were included in the study. The tonsillectomy group included 31 patients who underwent tonsillectomy surgery, while the control group included 30 patients who underwent inguinal hernia and circumcision surgery. Submental coronal plane ultrasonography examinations of the tongue were performed twice for each patient. In the tonsillectomy group, the first examination of tongue area (TA1) was done immediately after intubation but before the placement of tonsillar retractor. The second examination (TA2) was done at the end of the tonsillectomy surgery after the removal of the tonsillar retractor but before extubation. In the control group, the first examination (TA1) was done immediately after intubation, whereas the second examination (TA2) was done at the end of the surgery before extubation. These results were compared with those for the control group.
Results:
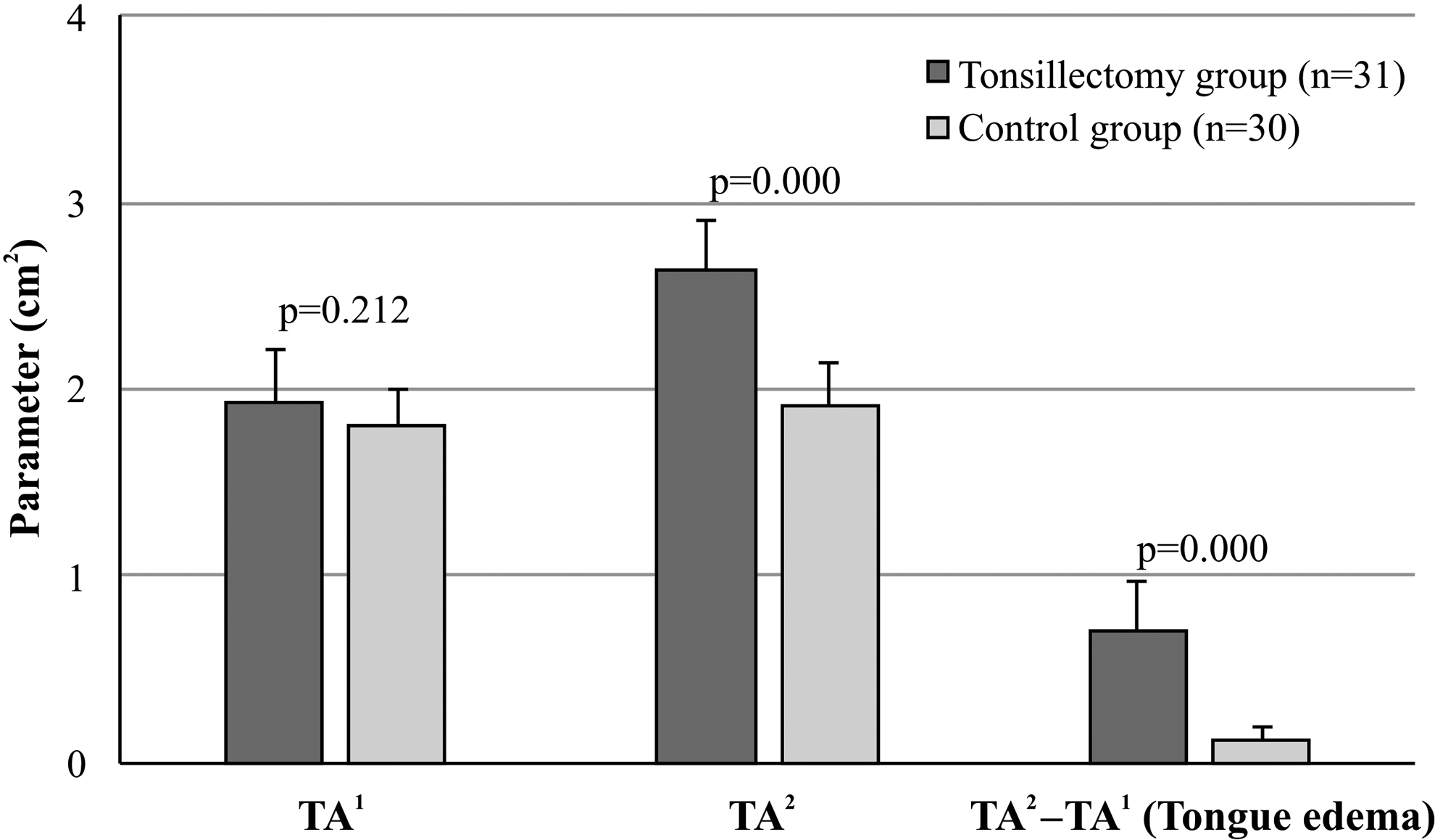
Groups were similar in terms of demographics and intubation duration. Groups did not significantly differ in terms of TA1 (P = .212), but they significantly differed in terms of TA2 (P = .000). They also significantly differed in terms of tongue edema defined as TA2 − TA1 (P = .000).
Conclusions and Significance:
Tonsillar retractor does cause tongue edema in tonsillectomy surgeries. This tongue edema seems to be a result of the pressure applied by the tonsillar retractor. This study is the first to demonstrate the possible role of ultrasonography examination in determining the tonsillar retractor–induced tongue edema in pediatric patients.
Introduction
Tonsillectomy is one of the most common procedures in pediatric patients and is a relatively safe procedure 1 ; however, it carries risk, in terms of airway complications with the rate of 2.4%. 2 Although children with risk factors are more likely to experience airway complications after tonsillectomy, 3 upper airway obstruction by the tongue or by uvular edema can occur and may lead to fatal complications even in healthy children without any risk factors.
The tongue is an organ composed of multiple muscles, and it is a unique organ for ultrasonography assessment; studies have indicated that the tongue can be clearly envisioned by ultrasonography when the probe is positioned under the chin, allowing for the accurate measurement of the tongue area and thickness. 4 Massive tongue edema is defined as the tongue’s enlargement enough to come out of the mouth and it is a rare but a fatal postoperative complication. 5 To date, a few cases of massive tongue edema have been reported, and it has been found that tongue edema is associated with devices that exert direct compression on the tongue; such devices include tonsillar retractor, endotracheal tube, and transesophageal echocardiography probe.5,6
Early diagnosis and rapid intervention are vital to prevent airway problems caused by tongue edema, regardless of the cause. 6 So far, neither a study on the physiological effects of tonsillar retractor has been conducted nor a guideline for the safe use of tonsillar retractor similar to the guidelines for other compression devices has been prepared. 7 No studies have been conducted on the development and diagnosis of tongue edema related with mechanical causes that cannot be noticed immediately after extubation and which may take up to 2.5 hours to develop after extubation, causing airway obstruction.8-10
Therefore, we aimed to detect the occurrence and amount of tongue edema through ultrasonography examination and to point out the association between tongue edema and tonsillar retractor in pediatric patients. The primary outcome was the change from preoperative measurement to postoperative measurement in the tongue area by ultrasonography imaging.
Our primary hypothesis was that there would be an increase in the tongue area because of the use of tonsillar retractor. The secondary outcome was the amount of tongue edema from prior to tonsillar retractor settlement to after removal of the tonsillar retractor. Our secondary hypothesis was that there would be an increase in tongue edema because of the use of tonsillar retractor.
Materials and Methods
Study Design
We prospectively studied submental ultrasonography of the tongue in pediatric patients undergoing tonsillectomy surgery at a university hospital. This study was approved by the Local Research Ethics Board. Informed written consent was obtained from the parents of all the patients.
Participants
Our study consisted of two groups in which patients aged 2–16 were included. Patients were excluded if they had a history of craniofacial abnormalities (e.g., Down syndrome, craniofacial trauma), systemic disorders. The tonsillectomy group (n = 31) consisted of patients who underwent tonsillectomy surgery. The control group (n = 30) consisted of patients who underwent endotracheal intubation under general anesthesia and who underwent inguinal hernia operation and circumcision operation in pediatric surgery.
Measurements
Demographic data, information about anesthesia, and surgery were recorded. Tongue area measurements were assessed twice for each patient by the same experienced anesthesiologist who was trained by a staff pediatric radiologist and who had at least 20 measurements in terms of tongue evaluation with submental ultrasonography. Three measurements were taken, and an average of these readings was used in the analyses for each measurement.
Primary outcome
In the tonsillectomy group, the first measurement (TA1) was done immediately after endotracheal intubation but before placement of the tonsillar retractor (Figure 1). The second measurement (TA2) was done after the tonsillectomy procedure following the removal of the tonsillar retractor just before extubation (Figure 2). In the control group, the first measurement (TA1) was done immediately after endotracheal intubation, and the second measurement (TA2) was done at the end of the surgical procedure just before extubation.
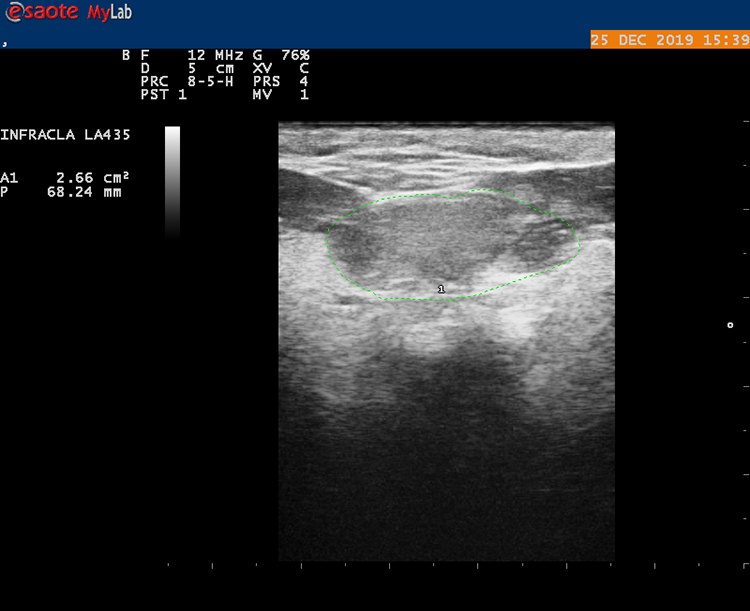
The first measurement of the tongue area before the placement of tonsillar retractor (TA 1 ).
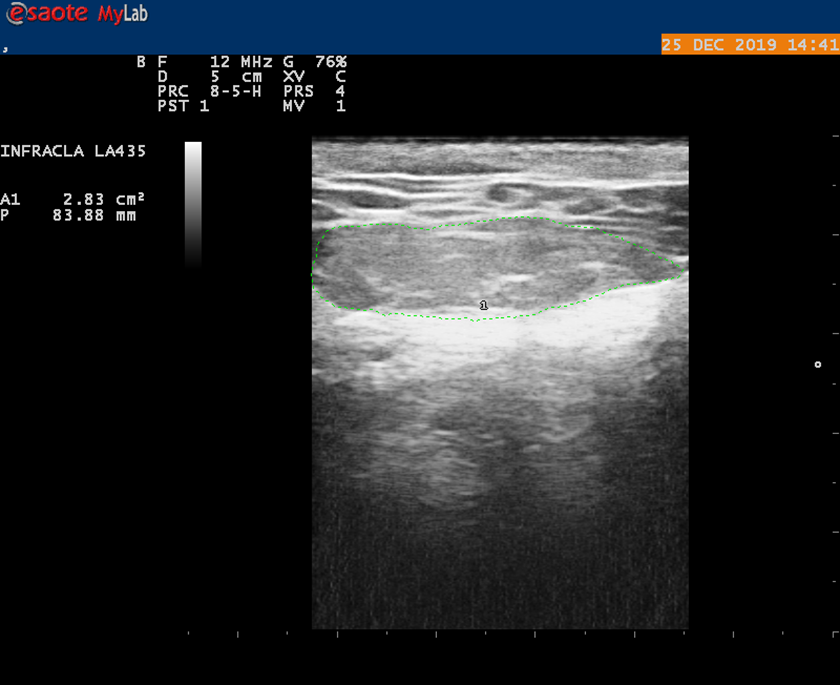
The second measurement of the tongue area after the removal of the tonsillar retractor (TA 2 ).
Secondary outcome
Tongue edema was defined in terms of the difference between TA2 and TA1 (ie, TA2 − TA1) for both groups.
Ultrasound Examination
Esaote MyLab with a convex probe working in the frequencies of 4 MHz was employed for tongue assessment. When the patient in the supine position, the probe was set below the chin, and the probe was not pressed too much when the tongue image was obtained. The probe was modified to envision the whole tongue outline on the monitor. The image was freezed when the tongue was visualized completely, and the tongue area was calculated automatically. The tongue area assessments were performed by a 4-MHz curved array from the submental midline region coronal plane. The duration of the tonsillar retractor attachment was recorded. The tonsillar retractor was not removed until the operation was completed. If the tonsillar retractor had to be removed before the operation was finished, the patient was excluded from this study (Figure 3).
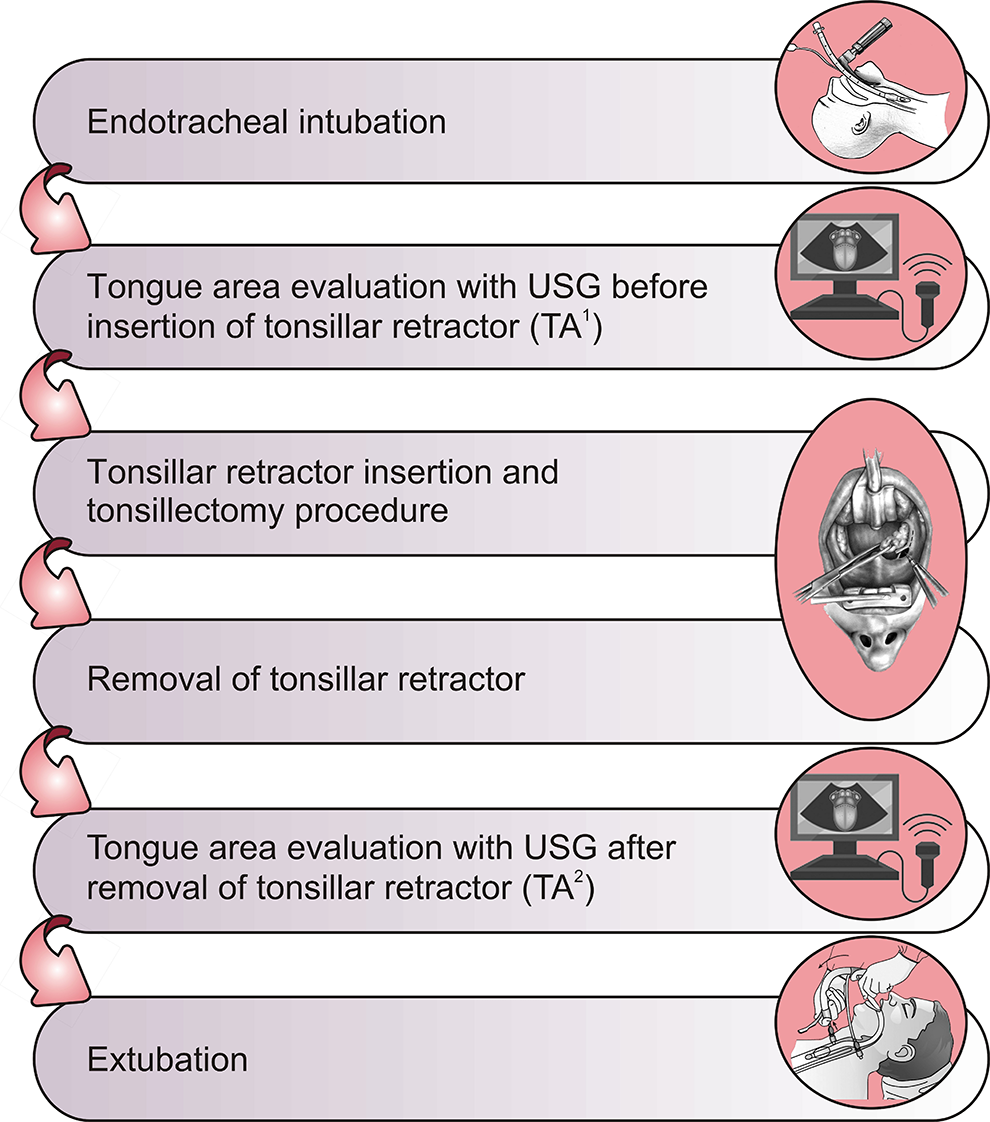
Flowchart of the study.
Surgical Procedure
All tonsillectomy surgeries were performed under general anesthesia using the dissection method by the same 2 experienced surgeons. Tonsillectomy was performed using cold instruments, and hemostasis was achieved with bipolar diathermy. Cold tonsillectomy was performed using the same Crowe-Davis tonsillar retractor blade. Routine general anesthesia was applied to each patient, who received methylprednisolone (1 mg/kg; Prednol-l, Mustafa Nevzat) at the induction of anesthesia. Each patient was intubated with the same brand of an endotracheal tube that was suitable for each patient’s age, and the endotracheal tube was fixed to the middle of the mouth. Tonsillar retractor was placed in the patient’s mouth until the tonsillectomy procedure was completed, and this period was noted.
Statistical Analysis and Sample Size
All data are expressed as mean ± standard deviation (SD). A nonparametric Mann-Whitney U test was used to determine whether the tonsillectomy and control groups differed on each variable. Data analysis was conducted using the Statistical Package for the Social Science software program (SPSS Version 17.0, IBM). A P value of <.05 indicated statistical significance. To consider the sample size, a pilot study was carried out in 10 patients from the tonsillectomy group. In the pilot study, the tongue area assessments before and after the placement of tonsillar retractor were 1.95 ± 0.29 cm2 and 2.63 ± 0.22 cm2, respectively. To suppose an equal SD and to indicate a difference of 20% between the 2 groups, a 2-sided type Ⅰ error of 0.05 and a power of 0.95 were applied. At least, 16 patients in each group were required to explore a significant difference in the tongue areas.
Results
There was no difference between the tonsillectomy and control groups in terms of demographics (Table 1). The mean intubation duration revealed no significant difference between the tonsillectomy (38.2 minutes) and control (35.1 minutes) groups (P = .6). The mean TA1 values revealed no significant difference between the tonsillectomy and control groups respectively, 1.93 ± 0.29 cm2 and 1.80 ± 0.20 cm2; P = .212). The mean TA2 values of the tonsillectomy group were higher and significantly differed (2.74 ± 0.28 cm2) compared to the control group (1.91 ± 0.23 cm2; P = .000). Moreover, the mean tongue edema values of the tonsillectomy group were higher and significantly differed (0.70 ± 0.26 cm2) compared to the control group (0.11 ± 0.07 cm2; P = .000; Figure 4).
Comparison Between the Tonsillectomy and Control Groups in Terms of Descriptive Statistics.a
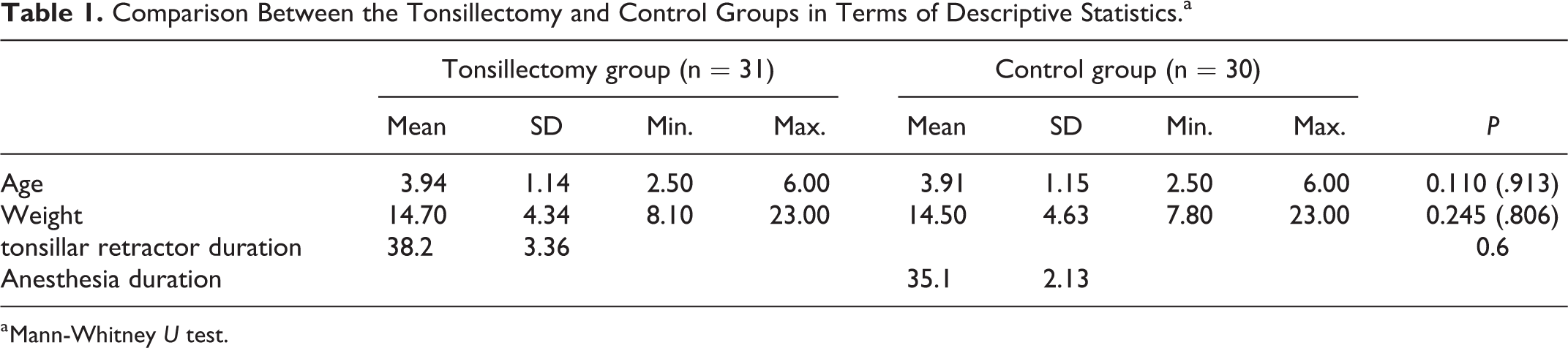
a Mann-Whitney U test.
Discussion
In this study, the tongue area was increased by 36% in the tonsillectomy group, while the rate of increase in the control group was only 6%. In our study, we determined tonsillar retractor–induced tongue edema that refers to pediatric patients due to the tonsillar retractor by ultrasonography. Although it did not produce clinical symptomatic findings in our patients, it may be an important problem because it may not be noticeable to the naked eye every time, and it can be overlooked.
In the literature, there is neither a study on the definition and detection of tongue edema by ultrasonography nor a study on the clinical reflection of tongue edema associated with the tonsillar retractor. However, studies have shown that the majority of postoperative complications in children undergoing tonsillectomy are caused by upper airway obstruction. In our study, we think that 36% tongue edema formation due to tonsillar retractor may cause respiratory complications arising from upper airway obstruction, by completely blocking the airway especially in high-risk patients with already small oropharyngeal airways, such as Down syndrome, morbid obesity, hypotonia, craniofacial abnormalities, obstructive sleep apnea syndrome (OSAS), and those at a young age (<2 years).3,11,12
In support, a study by Kieran et al 13 showed that Down syndrome is one of the factors that increase the risk of developing postoperative respiratory complications within the first 24 hours after surgery in children who underwent tonsillectomy. According to Gerber et al, 14 the probability of respiratory complications after tonsillectomy is higher by 8-fold in patients with Down syndrome than in patients without Down syndrome. Given the nature of Down syndrome, these patients have a large preoperative tongue and therefore, airway passages are already limited in the preoperative period. The tongue of patients with Down syndrome may have been enlarged due to the mechanical pressure created by the tonsillar retractor and that the restricted airway passage may have been further closed which may be related to postoperative respiratory complications.
In 2 different studies, pediatric patients with OSAS were 15 times more likely to have respiratory complications than the normal pediatric patient population, even if they were extubated fully awake after tonsillectomy.15,16 This result might have been observed because the airway passage of young patients with OSAS is already narrowed during the preoperative period, and the tonsillar retractor–induced tongue edema developed after tonsillectomy surgery may have closed this passage completely. Walker et al 17 also noted that the increased risk in these children was due to upper airway edema, but they did not specify a definitive cause or localization. And also, Ishman et al 18 implicated that in children who had just undergone tonsillectomy surgeries, tongue-based obstruction is an important cause of respiratory complications that occur after tonsillectomy surgeries.
In 2 other studies, authors have indicated that patients with craniofacial anomalies, particularly midfacial hypoplasia or micro/retrognathia, which affect their pharyngeal airway and very young children with relatively large tongues that restrict the airway passage, are prone to postoperative respiratory complications after tonsillectomy.3,16
Brown et al 19 noted in a study that respiratory complications that did not develop within the first 1 hour after tonsillectomy but developed between 1 and 8 hours postoperatively accounted for one third of the total respiratory complications. We believe that tonsillar retractor–induced tongue edema, which develops due to the use of tonsillar retractor, may be associated with these late complications. It is important to note the diagnosis of tonsillar retractor–induced tongue edema by ultrasonography in these children while undergoing tonsillectomy in order to prevent postoperative respiratory complications caused by upper airway obstruction.
Limitations
Our most important limitation is that we do not have any clinical outcomes regarding the tongue edema that we detected with ultrasonography. This would require clinical studies and clinical studies should look at not only breathing difficulties but also the effect of the tongue edema on pain, swallowing, and dehydration, as well as the length of time the tongue remains swollen. And also, our study included a relatively small number of patients, we didn’t measure tongue volume using ultrasonography, and the variability of ultrasonography measurements due to human factors, although the same trained anesthesiologist performed the measurements in our study. In addition, if we could have measured the tongue area several times, that is, in the PACU and ward, it would be better; however, in the postoperative period, we thought that measuring the tongue area in children with sore throat would not be very objective. Finally, if we could include pediatric patients with risk factors such as Down syndrome, OSAS, and craniofacial anomalies in the tonsillectomy group although their low incidence, the qualitative results of our study clearly revealed.
Conclusion
In pediatric patients who underwent tonsillectomy surgeries, tongue edema develops because of the pressure of the tonsillar retractor applied on the tongue, and it can be determined through submental ultrasonography. This edema may cause respiratory complications since it develops in the subacute period especially in patients with already restricted airway passage even if the patients are fully awake. A longer, larger prospective study (including patients considered a higher risk of postoperative airway compromise) that measures the change in tongue size pre- and postoperatively and follows patients longitudinally to identify postoperative complications related to upper airway obstruction would be of higher value. This would help determine the predictors of postoperative upper airway compromise such as certain demographic risk factors and degree of change in tongue size.
Supplemental Material
Supplemental Material, CONSORT_2010_Flow_Diagram_(1) - Can Tonsillar Retractor–Induced Tongue Edema Be a New Complication in Pediatric Patients Undergoing Tonsillectomy Detected by Ultrasonography? A Prospective, Case-Controlled, Observational Study
Supplemental Material, CONSORT_2010_Flow_Diagram_(1) for Can Tonsillar Retractor–Induced Tongue Edema Be a New Complication in Pediatric Patients Undergoing Tonsillectomy Detected by Ultrasonography? A Prospective, Case-Controlled, Observational Study by Merih Onal, Bahar Colpan, Cagdas Elsurer, Mete Kaan Bozkurt, Mehmet Ozturk, Ozkan Onal and Alparslan Turan in Ear, Nose & Throat Journal
Supplemental Material
Supplemental Material, ScribendiInc_Receipt_Order_650050_(1) - Can Tonsillar Retractor–Induced Tongue Edema Be a New Complication in Pediatric Patients Undergoing Tonsillectomy Detected by Ultrasonography? A Prospective, Case-Controlled, Observational Study
Supplemental Material, ScribendiInc_Receipt_Order_650050_(1) for Can Tonsillar Retractor–Induced Tongue Edema Be a New Complication in Pediatric Patients Undergoing Tonsillectomy Detected by Ultrasonography? A Prospective, Case-Controlled, Observational Study by Merih Onal, Bahar Colpan, Cagdas Elsurer, Mete Kaan Bozkurt, Mehmet Ozturk, Ozkan Onal and Alparslan Turan in Ear, Nose & Throat Journal
Footnotes
Authors’ Note
M. Onal, B.C., C.E., and M. Ozturk contributed to conceiving and designing the study, or collecting the data, or analyzing, and interpreting the data. M. Onal, B.C., O.O., M.K.B., A.T., and M. Ozturk contributed to writing the manuscript or providing critical revisions that are important for the intellectual content. M. Onal, O.O., and A.T. approved the final version of the manuscript. This study was approved by the Selcuk University Medical Faculty Research Ethics Board with the number of (2018-335). And also, the study was recorded to the Clinical Trials by the number of ![]() Identifier: NCT04204681.
Identifier: NCT04204681.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.