
Abstract
This study aimed to determine the value of either ultrasonography and computed tomography (CT) alone or both for diagnosing salivary gland stones. Based on their clinical findings and physical examination, 188 patients with salivary stones were included. Initially, an ultrasound was performed, and then a non-contrast-enhanced thin-sliced CT scan was done. The study included 161 patients with suspected submandibular gland (SMG) sialolithiasis and 27 with parotid gland (PG) sialolithiasis. Among the SMG cases, stones were confirmed in 130 patients through interventional sialoendoscopy. Sixteen of the stones were detected by CT scan only and were not seen in the previous ultrasound examination. After the second follow-up ultrasound, which was conducted after reviewing the CT scans, 9 of them were identified. Five patients with distal stones and ductal dilation on ultrasound were confirmed to have sialolithiasis. In 5 patients with stones detected on ultrasound but not on CT, dental filling artifacts were identified as the cause. For PG cases, stones were observed in 18 out of 19 patients with suspected sialolithiasis based on ultrasound and CT findings. Three patients with positive CT findings but negative ultrasound showed stones during sialendoscopy. During an ultrasound examination, palpating the floor of the mouth with the other hand’s index finger can help identify stones obscured by the shadow of the mandible, thereby enhancing the test’s accuracy. Patients with dental fillings, implants, and permanent dentures should not be referred for a CT scan to avoid unnecessary exposure to ionizing radiation. They also cause significant metallic artifacts in the field of interest. In these cases, ultrasound should be considered. To minimize the effects of ionizing radiation, it is recommended to create limited field requests for the target, focusing solely on the submandibular and PGs.
Introduction
Various imaging modalities are used to diagnose sialolithiasis and other disorders of the salivary glands. Ultrasound, sialography, computed tomography (CT) scan, and MRI are the most commonly used imaging techniques. Of course, ultrasonography (USG) is considered the primary modality in many centers worldwide due to its accessibility, affordability, and minimal systemic side effects. However, the sensitivity of USG varies greatly depending on the physician’s experience.1,2
CT is another effective diagnostic method that provides valuable information for imaging salivary gland stones. It is commonly used as the primary diagnostic tool in many medical centers. However, it does not show ductal dilation, other lesions, or parenchymal changes, or side effects such as ionizing radiation. 3
Our study compared both modalities for detecting stones in the submandibular and parotid glands (PGs).
Material and Methods
The records of 250 patients who applied to our institution with clinical findings of salivary stones between 2012 and 2023 were reviewed. Among these patients, 188 patients with properly recorded CT and USG reports were included in the study. Twenty-seven cases were PG stones, and 161 were submandibular gland (SMG) stones. The average age of presentation was 37 years (range: 25-78 years), with a male-to-female ratio of 1:1.8. The primary presenting symptom was recurrent or persistent salivary gland swelling (65%), followed by swelling associated with meals (45%).
After a physical examination, each patient included in the study was requested to have ultrasound and thin-sliced CT scans without contrast (with slices less than 1 mm). The stone’s location, size, and impact on the duct were evaluated.
CT exams were performed using a 16-multi-detector CT scanner (SOMATOM Sensation 16; Siemens, Forchheim, Germany) following the maxillofacial protocol at our hospital: tube voltage of 120 kV, tube current of 150 mA, the field of view of 240 × 240 mm, and rotation time of 0.50 seconds. Our exam protocol included axial acquisition (0.50 mm) with multi-planar reformation images. A lead thyroid collar is used for every patient.
USG scans were carried out at our center using 7.5 to 12 MHz linear probes by a skilled radiologist with head and neck imaging expertise. The average examination time was approximately 15 minutes. Lemon juice was given to the patient before the procedure to increase salivation and ductal flow. Color Doppler and power Doppler were used to distinguish dilated ducts and vascular structures and inspect the glands’ vascularity. Both glands were evaluated simultaneously, and the changes in the glands were observed more clearly.
All radiological evaluations were performed by the same specialist in head and neck radiology. The patients who underwent diagnostic and interventional sialendoscopy were compared based on their surgical records. Patients with inaccessible or incomplete records were not included in the study. The same team of doctors performed all surgical procedures.
Results
SMG Sialolithiasis
Clinically, we classified 161 patients with suspected SMG sialolithiasis based on ultrasound and CT findings (Figure 1).
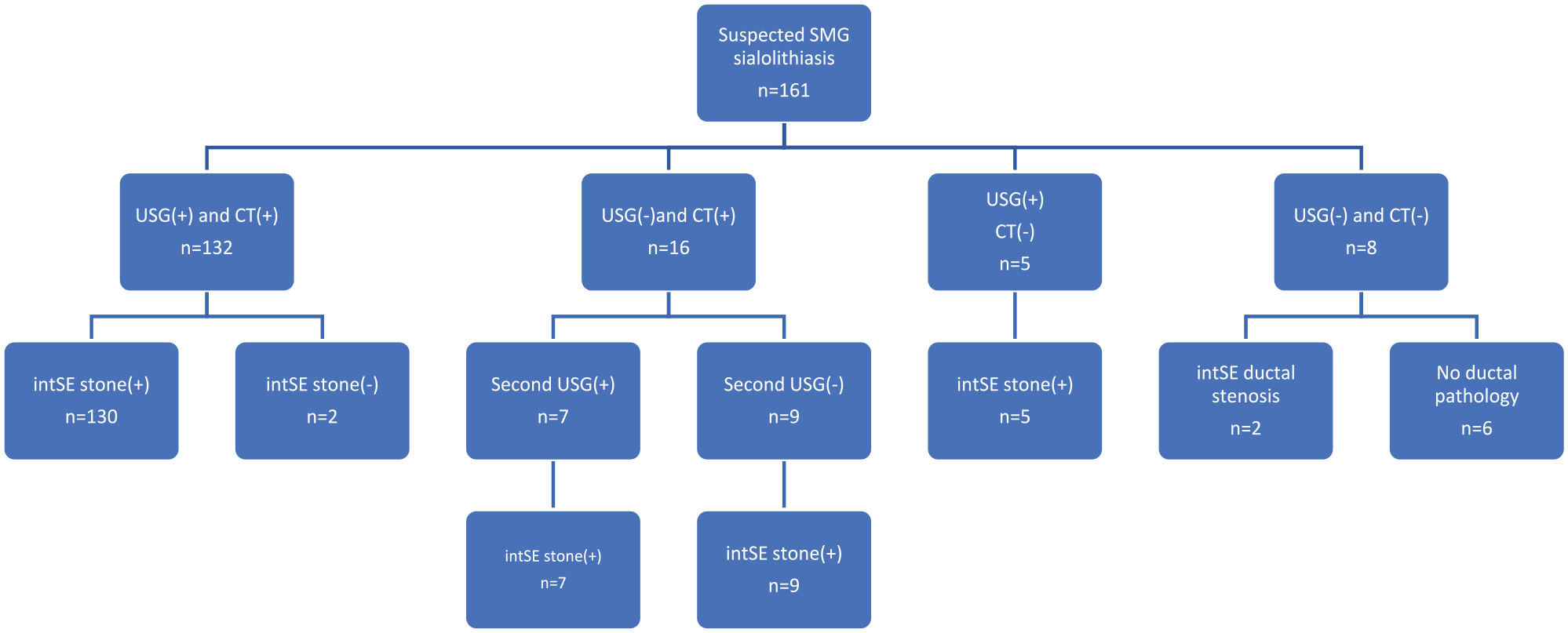
Comparison of CT and USG imaging and sialendoscopic findings in cases suspected of SMG stones. CT, computed tomography; intSE, interventional sialendoscopy; SMG, submandibular gland; USG, ultrasound.
Among the 132 patients with stones observed on ultrasound and CT, interventional sialendoscopy was performed, confirming the presence of stones in 130 patients. During interventional sialoendoscopy performed on 2 patients, stones could not be reached despite CT and USG indicating their location in the parenchyma or hilus (Figure 2).
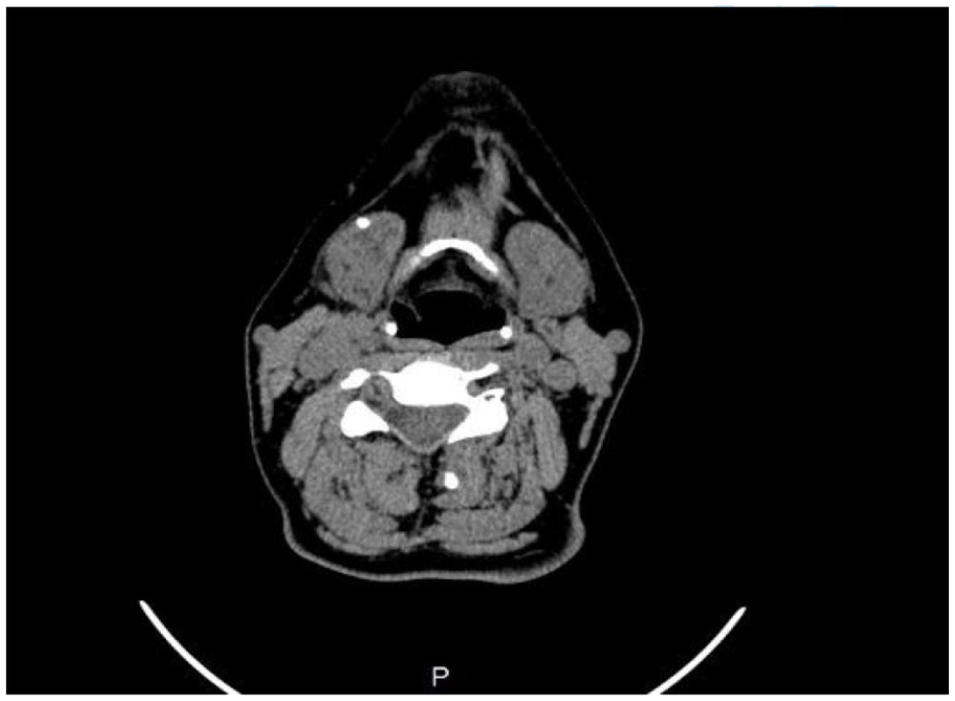
Stone observed in the parenchyma outside the duct.
In 16 patients, stones were observed on CT but were not detected on ultrasound, and a second ultrasound with a bimanual maneuver revealed stones in 9 patients. Five of the remaining 7 patients with distal Wharton secondary ductal stones had ductal dilatation seen in ultrasound, but the stones were seen by CT only. All these cases were confirmed by interventional sialoendoscopy.
Table 1 compares the characteristics of 5 patients with no stones observed on ultrasound but with CT and operative findings.
Characteristics of Patients in False-Negative Ultrasonography Cases for Sialolithiasis.
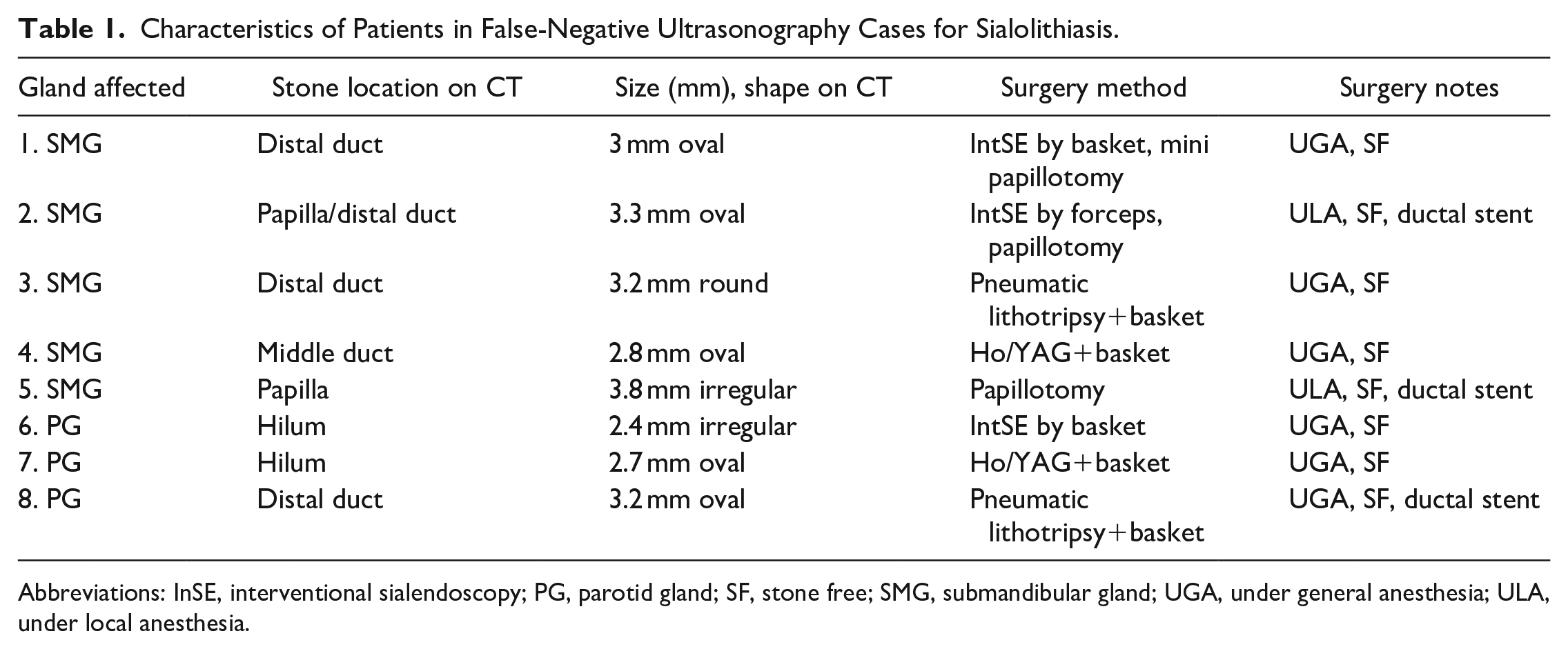
Abbreviations: InSE, interventional sialendoscopy; PG, parotid gland; SF, stone free; SMG, submandibular gland; UGA, under general anesthesia; ULA, under local anesthesia.
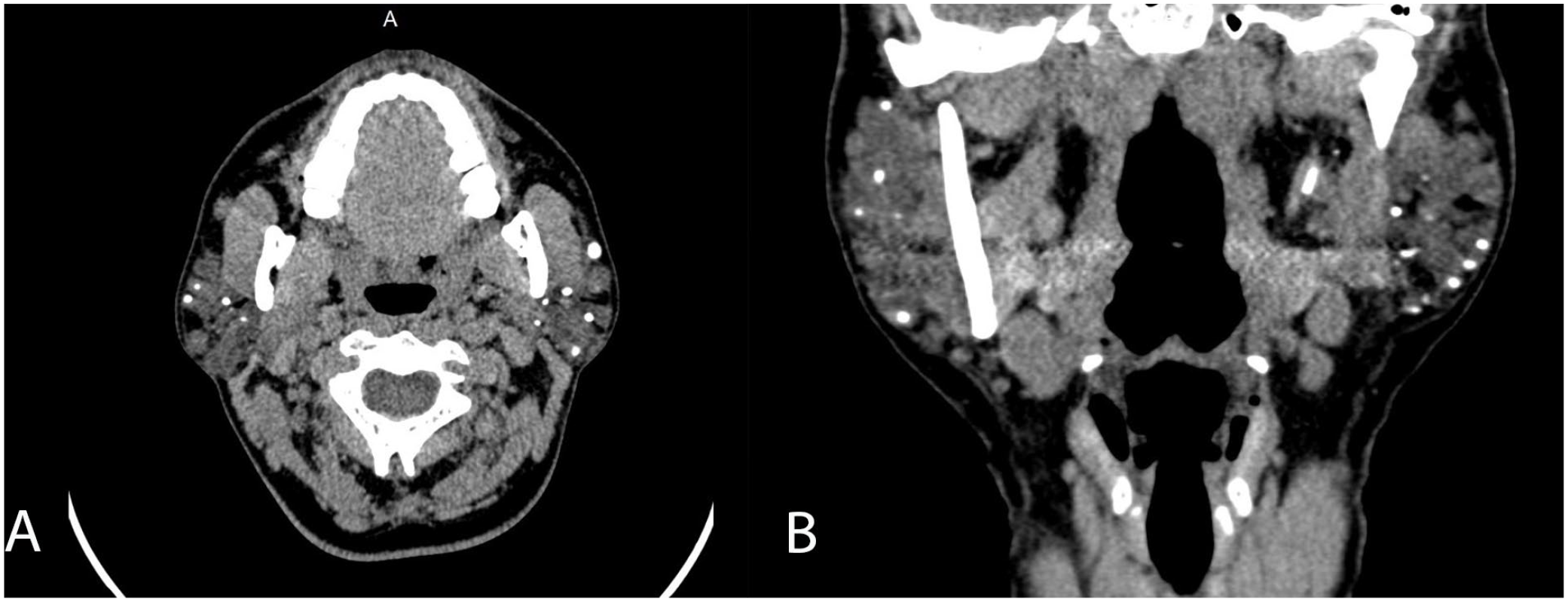
The average stone size in these patients was 2.76 mm, with most (4 out of 5) stones localized in the papilla/distal duct (Figure 3). One patient had a stone in the middle duct.
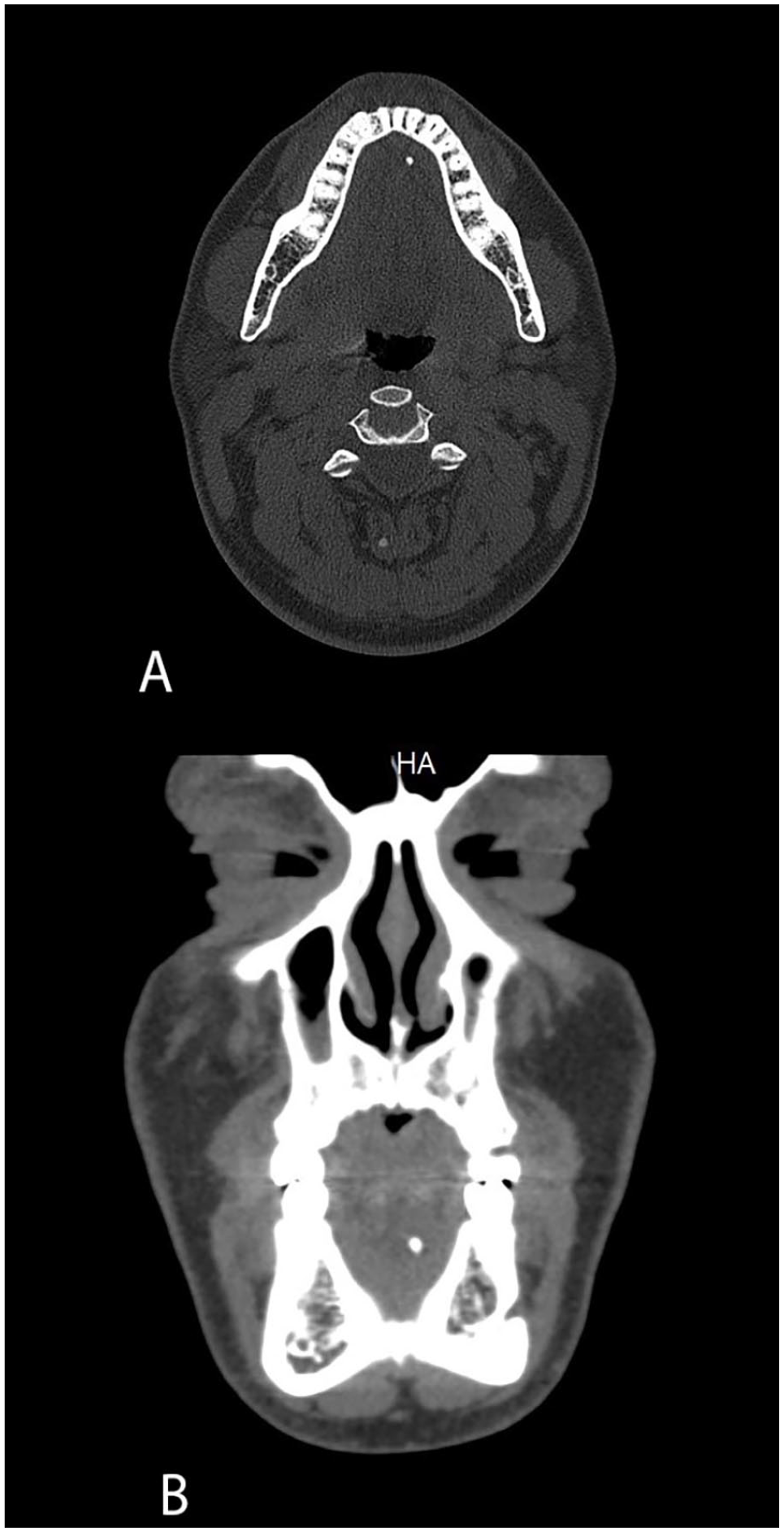
Axial (A) and coronal (B) non-contrast-enhanced CT scans show a stone in the distal aspect of Wharton’s duct. CT, computed tomography.
Five patients with stones observed on ultrasound were not visible on the CT scan due to metallic artifacts from dental fillings on the same side of the lower jaw. During sialoendoscopy, the patients were found to have stones (Figure 4).
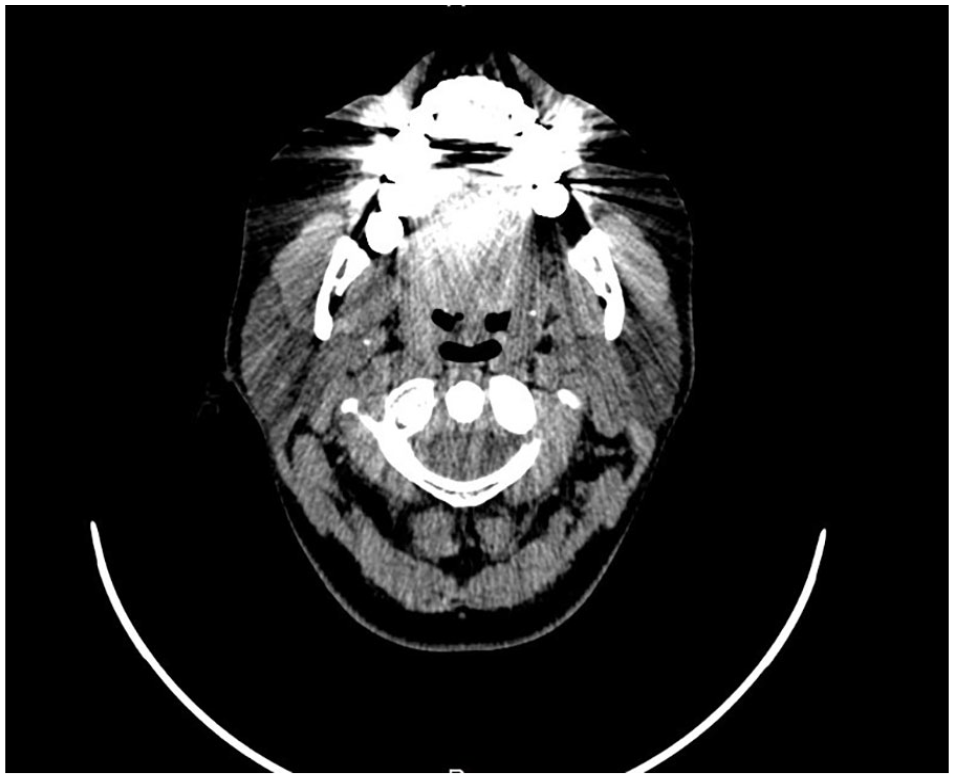
Severe metallic artifacts around the mandible in axial CT scan due to dental implants hiding the distal stone of the right Wharton duct. CT, computed tomography.
Despite presenting clinical symptoms, no stones were observed in ultrasound or CT scans in 8 patients, and all patients had sialendoscopy. Three of these patients with SMG ductal dilation underwent sialendoscopy, which revealed ductal stenosis in 2 patients. Medical records of these patients clarified that 2 underwent a minor salivary gland biopsy, and 1 was diagnosed with Sjögren’s syndrome.
Sensitivity, specificity, and positive and negative predictive values (NPVs) of ultrasound, CT, and sialoendoscopy were compared for stone detection in patients suspected of SMG sialolithiasis. Significant differences (according to the McNemar test, P < .05) were observed in the sensitivity values of sonography compared to the other methods. No significant differences were observed in the specificity and sensitivity of CT and sialendoscopy. Regarding positive predictive value (PPV), ultrasonography, CT, and sialendoscopy showed 98%, 99%, and 100%, respectively, indicating minimal differences between the 3 methods. The NPV was 33%, 61%, and 80%, respectively, highlighting the superior reliability of sialendoscopy in making negative predictions (Figure 5).
Statistical comparison of USG, CT, and sialendoscopy in submandibular gland sialolithiasis patients. CT, computed tomography; USG, ultrasonography.
PG Sialolithiasis
Nineteen of the 27 patients suspected of parotid sialolithiasis had records of stones visible on both ultrasound and CT images, with stones observed in 18 patients during sialendoscopy (Figure 6).
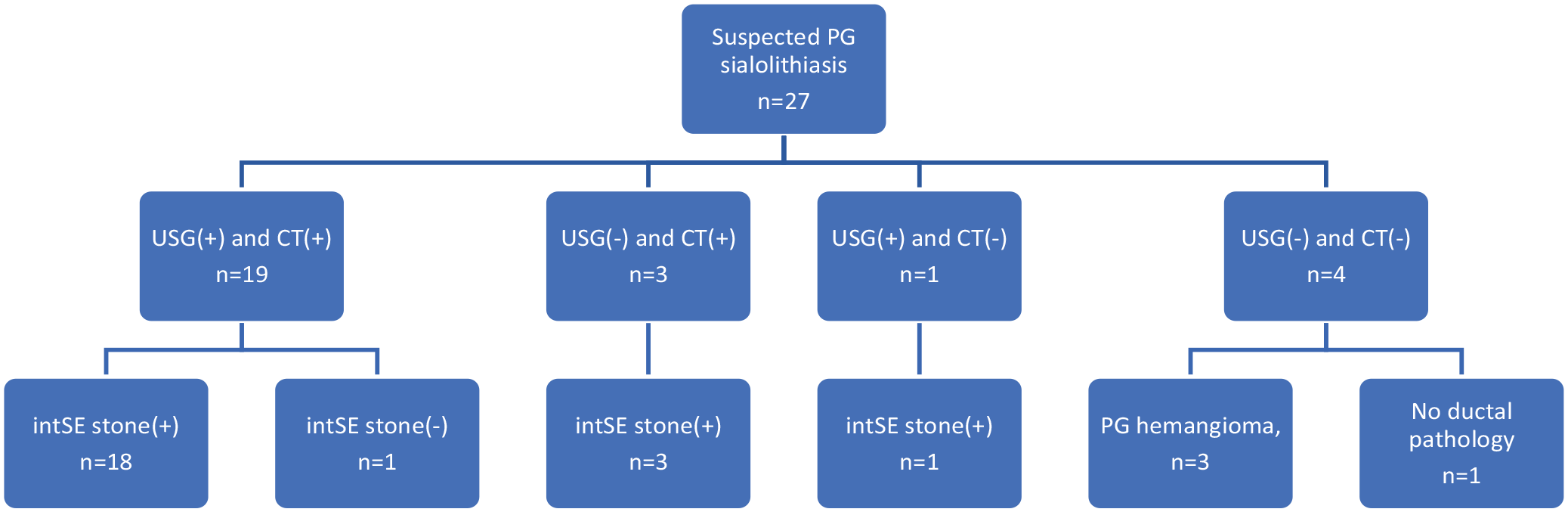
Comparison of CT and ultrasound (USG) imaging and sialendoscopic findings in cases suspected of PG stones. CT, computed tomography; intSE, interventional sialendoscopy; PG, parotid gland.
One patient was inaccessible due to the stone’s location in the intraparenchymal region (Figure 7). In 3 patients with no stones observed on ultrasound but with positive CT findings, stones were observed in all 3 during sialendoscopy. Table 1 compares the CT and intraoperative characteristics of these patients.
Axial (A) and coronal (B) CT scan showing multiple parenchymal calcifications in the bilateral parotid glands in a patient with chronic parotitis. CT, computed tomography.
In 1 patient with suspected sialolithiasis on ultrasound but with no stones observed on CT, a stone was found during sialendoscopy. The patient’s CT report indicated that evaluation could not be performed due to metallic dental artifacts in the upper jaw area.
Four patients presented with recurrent parotid swelling, with calcifications observed on both ultrasound and CT reports. Three of them were diagnosed with parotid hemangioma (Figure 8).
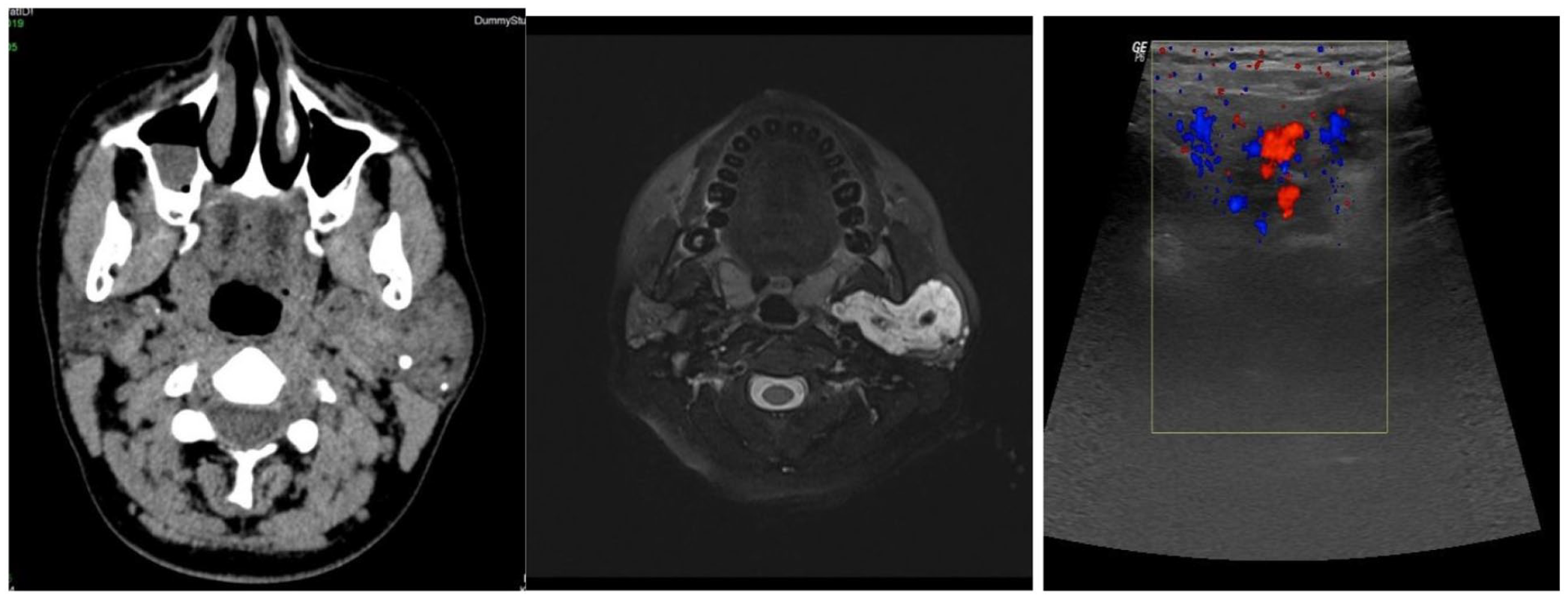
Axial CT (A) and axial MRI (B) show multiple calcifications within a hemangioma in the superficial lobe of the left parotid gland. (C) Calcified foci on the hemangioma walls when the USG test was performed with Doppler. CT, computed tomography.
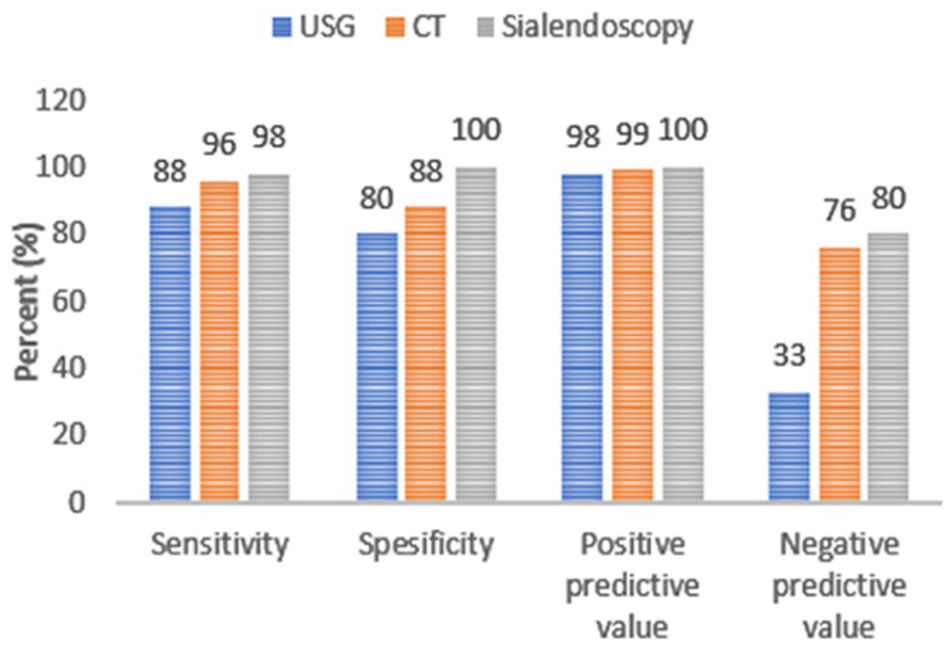
The sensitivity, specificity, PPVs, and NPVs of ultrasound, CT, and sialendoscopy for detecting stones in patients suspected of PG sialolithiasis were compared. According to these results, sialendoscopy demonstrated high sensitivity (100%) in detecting PG sialolithiasis, which was statistically significant (McNemar test, P < .05) compared to both ultrasonography (86%) and CT (95%; Figure 9).
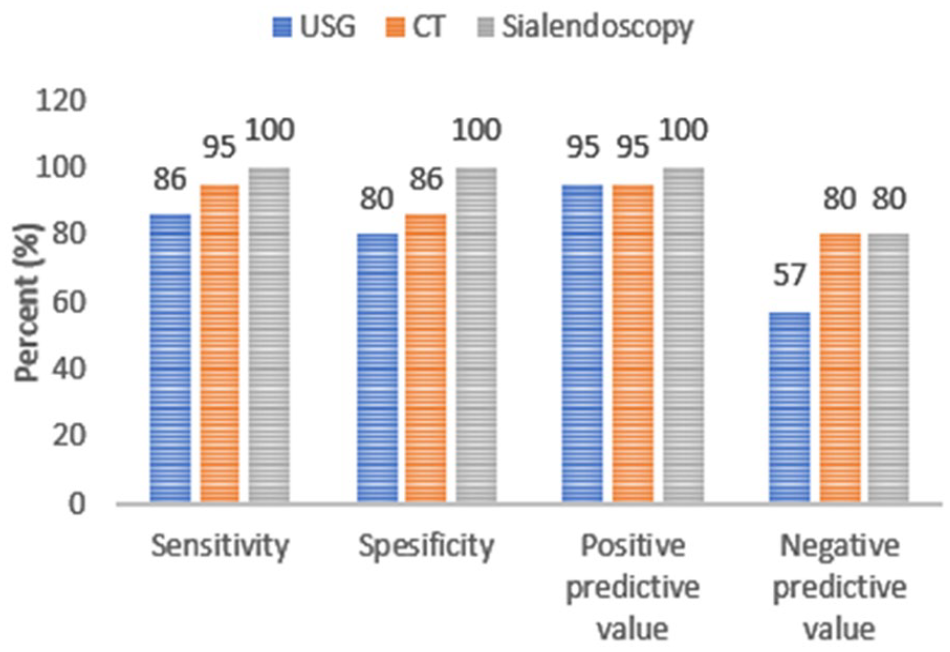
Statistical comparison of USG, CT, and sialendoscopy in parotid gland sialolithiasis patients. CT, computed tomography; USG, ultrasonography.
Regarding the PPV, there are no substantial differences between ultrasonography (95%), CT (95%), and sialendoscopy (100%). However, the NPV for ultrasonography (57%) is notably lower compared to CT (80%) and sialendoscopy (80%).
Discussion
Various imaging modalities are used to diagnose sialolithiasis of the salivary glands. Here, we compare our findings with the information presented in the existing literature.
While ultrasound imaging of the head and neck region requires particular expertise, ultrasound imaging of the salivary glands appears to be a more specific area. For this reason, the literature states that a lack of experience in performing USG in the head and neck region is significant in contributing to false-negative results.4,5
Ultrasound offers several advantages. It is a cost-effective examination that is easy to perform and is readily available in medical institutes. No radiation is involved, making it safe for all age groups without any restrictions. With advances in ultrasound technology, high-resolution superficial transducers, and sophisticated machines, we can now differentiate and diagnose most salivary gland diseases and lesions.6,7
In studies conducted by Schwarz, the sensitivity of USG was determined to be 70%. 8 Thomas et al observed that ultrasound (USG) sensitivity was 65%, and a lack of standardization in the ultrasound protocol was noted. While explaining this low rate in his article, he stated that USG examinations were performed in conjunction with intraoral palpation and assessment by an ear, nose, and throat (ENT) physician in other studies. He stated that a USG examination was performed by a radiologist at his institution. 8
Since USG converts the signals reflected from the stone’s surface into images, it only gives complete information about the stone even if performed in 2 planes.9,10
In our study, the USG examination was conducted by a radiologist specializing in the head and neck region in collaboration with an otolaryngologist capable of performing sialendoscopy. We determined the sensitivity of USG to be 88%.
False negativity in SMG sialolithiasis was observed in 16 patients. In most patients, active symptoms and the significant dilation of ductal structures observed in the initial sonography strongly suggested sialolithiasis. In the following CT scans, all these patients were found to have stones. In the second look sonography, after evaluating the CT scans, stones were visualized in 9 patients, while 7 showed no stones. During the secondary sonography, the radiologist palpated the floor of the mouth with the index finger of the other hand to help identify stones in the mandibular shadow.
In recent literature, the combined intraoperative use of ultrasound with endoscopy has been reported to treat selected cases. The location of the stone was determined using ultrasound during sialendoscopy in the operating room. The skin was marked, and the endoscope light was directed toward the marked location. 11
Our study observed false negativity in 3 cases of PG sialolithiasis. Two of these patients had stones localized in the proximal duct; these stones were less than 3 mm in size, as observed in CT imaging. One patient had a stone located distal to Stensen’s duct, which was not visualized on ultrasound due to dental interference (Table 1).
However, another issue that should be noted is that the USG examination of the PG was more reliable than the SMG USG. The reason for this is the SMG’s proximity to the mandible. Still, only a tiny portion of the deep lobe of the PG may be obscured by the mandible’s acoustic shadow. 12
Small stones measuring 2 mm can be missed by ultrasound. Palpating the floor of the mouth during the USG exam with the index finger of the other hand can identify stones in the shadow of the mandible and increase accuracy. Intraoral ultrasound probes can detect distal Wharton’s duct stones. 13
The test, which had been previously reported as multiple stones in the salivary gland in other centers without sialendoscopy experience, was determined to be calcified foci on the hemangioma walls when the USG test was performed with Doppler at our institution (Figure 8C). Incorrect diagnosis of sialolithiasis can result in unnecessary interventions.
The impact of stone localization and size on the false negativity of sonography is particularly significant. False-negative results were especially encountered in cases where the stone diameter was less than 3 mm and in stones located close to the mandible at the exit of the duct in the SMG.
In most countries, USG imaging is performed by a radiologist. The author, who conducts sialendoscopy, was also present during the exam at our center. This application is beneficial for both ENT specialists and radiologists. 14
Non-enhanced CT is highly sensitive in detecting salivary gland stones, particularly the small ones. Many medical centers use it as the primary diagnostic tool for sialolithiasis. It is especially useful in identifying stones that may not be detected by ultrasound, either due to their distal ductal location or the operator’s limited experience. The disadvantages of a CT scan include its inability to show the gland parenchyma and its ducts and its use of ionizing radiation. Using thin-sliced CT scans and 3D reconstructions is very important to detect distal ductal stones that were not visible on ultrasound. We verified that CT is more sensitive 95% (59/62) than ultrasound 74% (46/62) in detecting distal ductal stones in SMG. Yet, CT scans cannot show the ductal ectasia and the parenchymal changes. For this purpose, we may use MRI and MRI sialography. It is a fact that ionizing radiation is a significant disadvantage.
CT imaging provides better information about the stone itself than USG. Some of the stones determined to be single stones on USG were found to be multiple sialoliths on CT scans. We encountered such a situation in 3 of our patients.
Terraz et al cited ductal stenosis with wall fibrosis as the cause of false-positive findings, which was erroneously interpreted as lithiasis. 15
In imaging, calcifications outside the duct are more clearly visible on CT scans. Especially in these cases, evaluating the patient’s symptoms along with ultrasound and MR sialography findings is essential to exclude false positives. 16 In our case series, we observed widespread multiple calcifications in the parenchyma of 2 patients with false-positive CT findings.
We observed a sensitivity of 98% and a specificity of 83% for diagnosing sialolithiasis using CT scans. Preoperative CT scans are particularly valuable as they provide essential information about the size, structure, and location of stones, especially for interventional sialendoscopy procedures conducted under general anesthesia. To minimize the significant disadvantage of radiation exposure, targeted imaging can be considered, or lead shielding can be used to protect the thyroid gland, which is sensitive in the neck, from radiation exposure during scanning.
Metallic artifacts can degrade image quality and obscure structures at the ductal level in patients with a history of dental implants. In our study, stones could not be observed in 3 cases of SMG sialolithiasis and 1 case of PG sialolithiasis for this reason. Therefore, before conducting a CT scan, it is essential to confirm the presence of fillings in the same area. If fillings or dental implants are present, a CT scan should not be performed to prevent unnecessary radiation exposure.
Kiringoda et al wrote some parotid stones were described as radiolucent in the literature. These types of stones could not be visualized with a CT scan. The author stated that although these stones were not seen in a CT scan, they were detected during sialendoscopy. 17 We did not encounter such a finding in our study.
In our study, all false-negative cases in sonography were found to be located at the distal ductal level, with an average size of 2.9 mm. Approximately 85% of distal ductal stones were detected by ultrasound, while most were identified through CT scans. Thin-sliced CT scans and 3D reconstructions are essential for identifying distal ductal stones that were not visible on ultrasound.
Our study revealed that sialendoscopy demonstrated superior sensitivity and specificity to USG and CT in detecting stones.
However, despite being considered a minimal intervention, sialendoscopy has significant disadvantages, including its limited availability in medical centers and high cost. 18
As a result of this study, we found that the combined use of USG and CT in the appropriate order provides more accurate information for diagnosing and treating sialolithiasis.
Finally, we must acknowledge several study limitations, including small sample size, single-center design, and retrospective evaluation. Future prospective studies with more extensive case series are needed to elucidate further the varying effectiveness and inadequacies of USG and CT.
Conclusion
The sensitivity of USG varies greatly depending on the experience of the person performing it. Palpation of the mouth and neck area floor during USG can increase accuracy.
Simultaneous palpation of the mouth and neck area floor during USG can increase accuracy. For example, palpation of the floor of the mouth with the other hand’s index finger can identify stones hidden by the mandible’s shadow.
It is recommended to decrease the scan area and protect the thyroid gland with a lead collar to minimize the side effects of ionizing radiation.
CT scans are not recommended for individuals with dental fillings, implants, and permanent dentures due to severe metallic artifacts.
Footnotes
Acknowledgements
None.
Author Contributions
Data Availability Statement
The available data of the study may be sent upon request for scientific purposes.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
This study was approved by the Medipol University, Medical Faculty, Ethics Committee (Date, September 30th, 2021 and No. 10840098-772.02-4982).
Informed Consent
Informed consent was obtained from the patients before they were included in the study.