
Abstract
Objectives:
To analyze the clinical characteristics of congenital cholesteatoma (CC), to explore the risk factors related to recurrence of the disease, and to clarify the importance of staging for treatment.
Methods:
A total of 87 patients were followed up for more than 5 years, who had undergone surgical procedures for CC from September 2010 to January 2017 in Beijing Children’s Hospital, Capital Medical University. Patients with CC were identified in accordance with the following Levenson’s criteria. The clinical characteristics of CC on different stage and risk factors related to recurrence of the disease were analyzed.
Results:
Canal wall up mastoidectomy and tympanoplasty (n = 45), transcanal endoscopic approach (n = 29), and canal wall down mastoidectomy and tympanoplasty (n = 13) was, respectively, performed depending on cholesteatoma extension. Between 2010 and 2013, 20.93% of patients had stage I-II disease, whereas 61.26% had stage I-II disease from 2014 to 2017. Meanwhile, the proportion with stage III-IV disease decreased from 79.07% to 38.64% between these 2 time periods. The preoperative air conduction threshold in patients with stage I, II, III, and IV was, respectively, 23.36 ± 8.20, 45.40 ± 12.82, 47.49 ± 12.03, and 50.37 ± 11.80 dB. The stage of disease was a significant risk factor regarding recurrence (P = .02). Surgery on patients with stage III-IV disease was performed with the aid of a microscope from 2010 to 2013 and with a microscope and endoscope from 2014 to 2017, which reduced the recurrence rate from 26.92% in the former period to 8.33% in the latter period.
Conclusion:
Early detection of CC is crucial regarding the facilitation of minimally invasive surgery and reducing complication and recurrence rates. The stage of the disease is a significant risk factor regarding recurrence. The surgery shows us the possibility of reducing the recurrence rate of CC, which is performed under a microscope and an endoscope.
Introduction
Congenital cholesteatoma (CC), defined as a whitish mass lesion in the middle ear behind an intact tympanic membrane (TM), is relatively rare. In 1989, Levenson et al modified and established the criteria that are now widely accepted. 1 Congenital cholesteatomas account for 1% to 5% of cholesteatomas in most published series. 2 The symptoms are diverse, depending on the location and extent of lesions, from asymptomatic to conductive hearing loss, facial nerve palsy, sensorineural hearing loss, and intracranial complications. These lesions may enlarge progressively to surround and destroy the ossicles, resulting in conductive hearing loss. Early diagnosis and intervention have been emphasized because delay may be associated with more extensive disease. Not only is CC in children more aggressive than in adults, it is also more prone to recurrence. 3 Thus, the aim of this study was to present the clinical features of CC of the middle ear in children and try to determine the risk factors related to recurrence of the disease.
Patients and Methods
In this study, the medical records of patients with a diagnosis of middle ear cholesteatoma in Beijing Children’s Hospital, Capital Medical University from September 2010 to January 2017 were retrospectively reviewed. Patients with CC were identified in accordance with the following criteria, 1 which were proposed by Levenson et al: a white mass or masses behind an intact TM; the absence of TM perforation; and no history of otologic procedures such as paracentesis or ventilation tube insertion. Patients with a history of acute otitis media or otitis media with effusion were included. All study patients had undergone surgery and the final diagnosis of CC had been confirmed by postoperative pathological examination in all cases. Patient characteristics examined included age at surgery, sex, and chief complaint at the time of initial diagnosis. Tympanic membranes were examined by endoscopy before surgery and intraoperative findings included the location of each mass in the middle ear, extent of disease, and erosion of ossicles. All study patients underwent preoperative examination with high-resolution computed tomography (CT) images in the axial plane with coronal reformation. Staging of the cholesteatomas was based on the classification suggested by Potsic et al, 4 which is as follows: stage I, disease confined to a single quadrant; stage II, cholesteatoma in multiple quadrants but without ossicular involvement or mastoid extension; stage III, ossicular involvement without mastoid extension; and stage IV, mastoid involvement. The type of CC was determined according to the morphological classification of McGill et al, 5 that is, closed cyst (encapsulated cholesteatoma) or open infiltrative cyst (cholesteatoma matrix in direct contact with the middle ear mucosa). All patients were followed up for 5 years postoperatively. The presenting symptoms, distribution of cholesteatoma stage and type, duration of disease, age at surgery, surgery type, complications, and recurrence rates were analyzed. Magnetic resonance imaging (MRI) is used to assess patients who have difficulty in CT scan and otoscopy confirming recurrence of cholesteatoma in the middle ear. The statistical significance was assessed by SPSS version 19.0, P < .05 being taken to denote a statistically significant difference.
Results
Ninety-six patients were initially included in this study, but only 87 patients have completed the follow-up work for more than 5 years. All patients were unilateral, involving 87 ears, 45 left ears, and 42 right ears. The characteristics of the 87 patients are summarized in Table 1. Sixty-two boys (71.26%) and 25 girls (28.74%), who had been diagnosed with CC and undergone surgical treatment between September 2010 and January 2017 were included in the study. The mean age at surgery was 6.04 ± 2.41 years (range: 2.17-12.92 years). The mean duration of disease was 8.61 ± 11.13 months (range: 0.3-72 months). The chief complaint was hearing loss in 73.56% (64/87), accidental finding in 20.69% (18/87), facial paralysis in 3.45% (3/87), and other in 2.30% (2/87). The diagnosis was made by CT examination in 62 cases (71.26%), endoscopy in 23 cases (26.44%), and during myringotomy for otitis media with effusion in the remaining 2 cases (Table 1).
Characteristics of 87 Patients With CC.
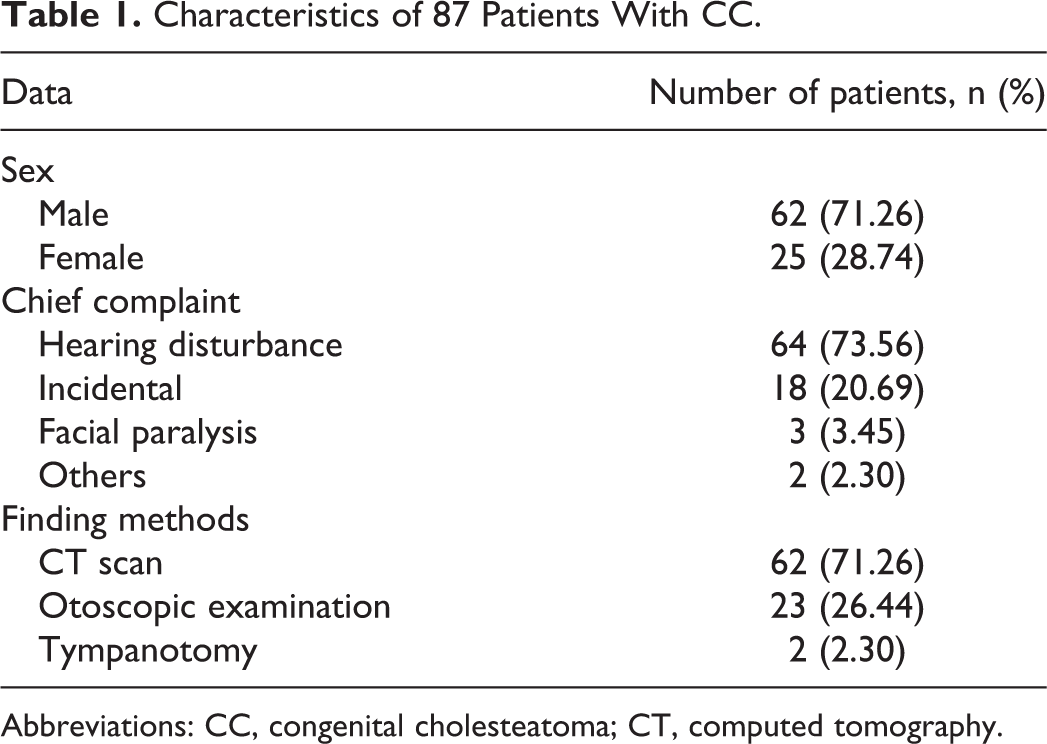
Abbreviations: CC, congenital cholesteatoma; CT, computed tomography.
According to the staging system, 16.09%, 25.59%, 20.69%, and 37.93% of patients had stages I, II, III, and IV disease. Of the 87 patients, 64 (73.56%) had the open type of cholesteatoma and 23 (26.44%) the closed type, as determined by the surgical findings. The locations of the lesions in the tympanic cavity are shown in Table 2. Among the lesions involving 1 or 2 quadrants, 74.07% (n = 40) were in the posterior-superior quadrant (PSQ) and 62.96% (n = 34) in the anterior-superior quadrant (ASQ). The most frequently performed surgical technique was canal wall up mastoidectomy and tympanoplasty (CWU+T; n = 45; 51.72%), followed by a transcanal endoscopic approach (TEA; n = 29; 33.33%) and canal wall down mastoidectomy and tympanoplasty (CWD+T; n = 13; 14.94%; Table 2). Those patients undergone TEA were followed up closely, but no mandatory second-look surgery was performed. For patients with TEA younger than 6-year-old with stapes involvement, 2-stage operation was performed.
Intraoperative Findings.
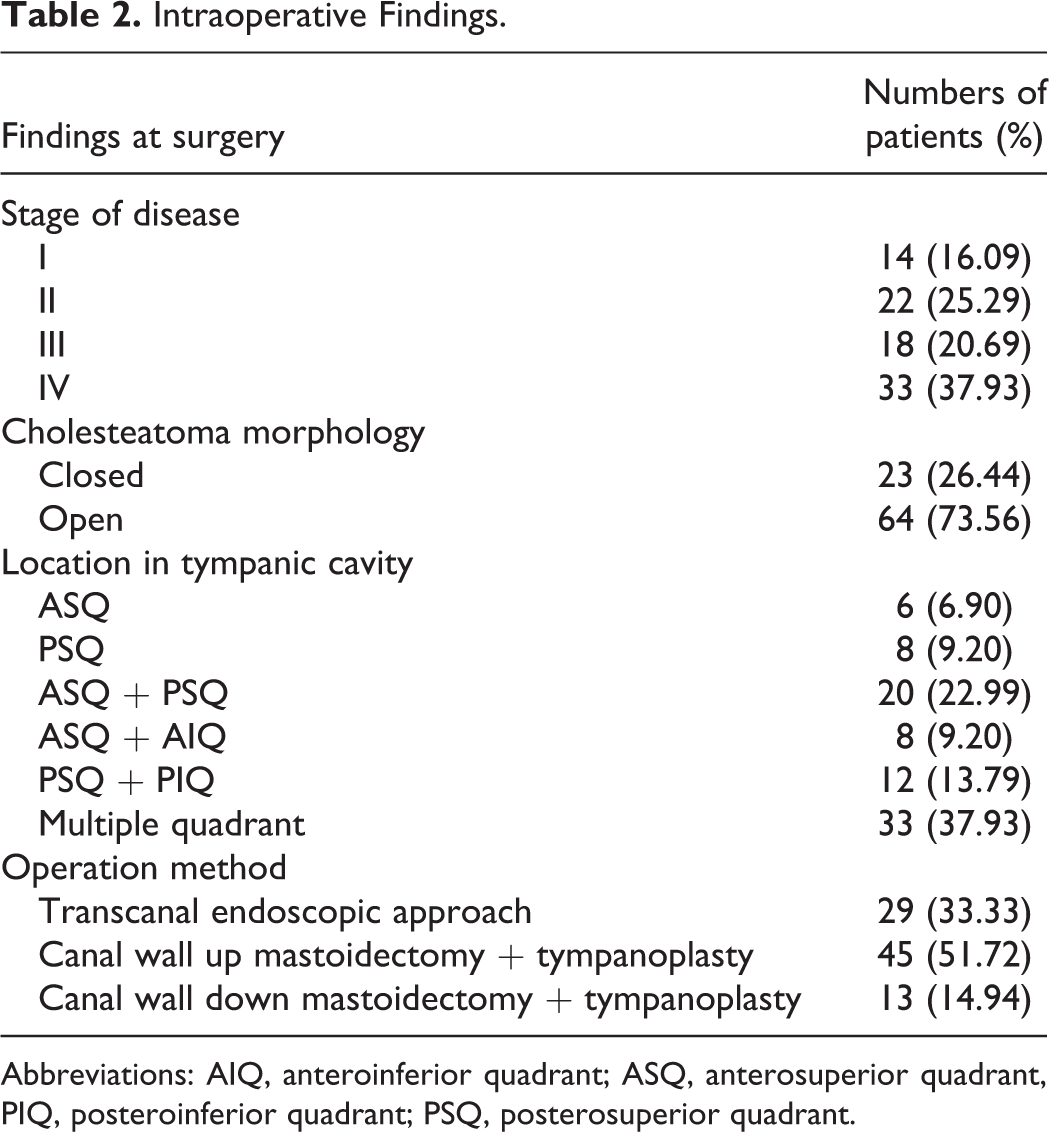
Abbreviations: AIQ, anteroinferior quadrant; ASQ, anterosuperior quadrant, PIQ, posteroinferior quadrant; PSQ, posterosuperior quadrant.
Between 2010 and 2013, 20.93% of the patients had stages I-II disease; the proportion increased to 61.26% between 2014 and 2017. Meanwhile, the proportion with stages III-IV disease decreased from 79.07% to 38.64% between these 2 time periods. Figure 1 shows the proportion with each stage of disease in these 2 time periods; the differences are statistically significant (P < .05).
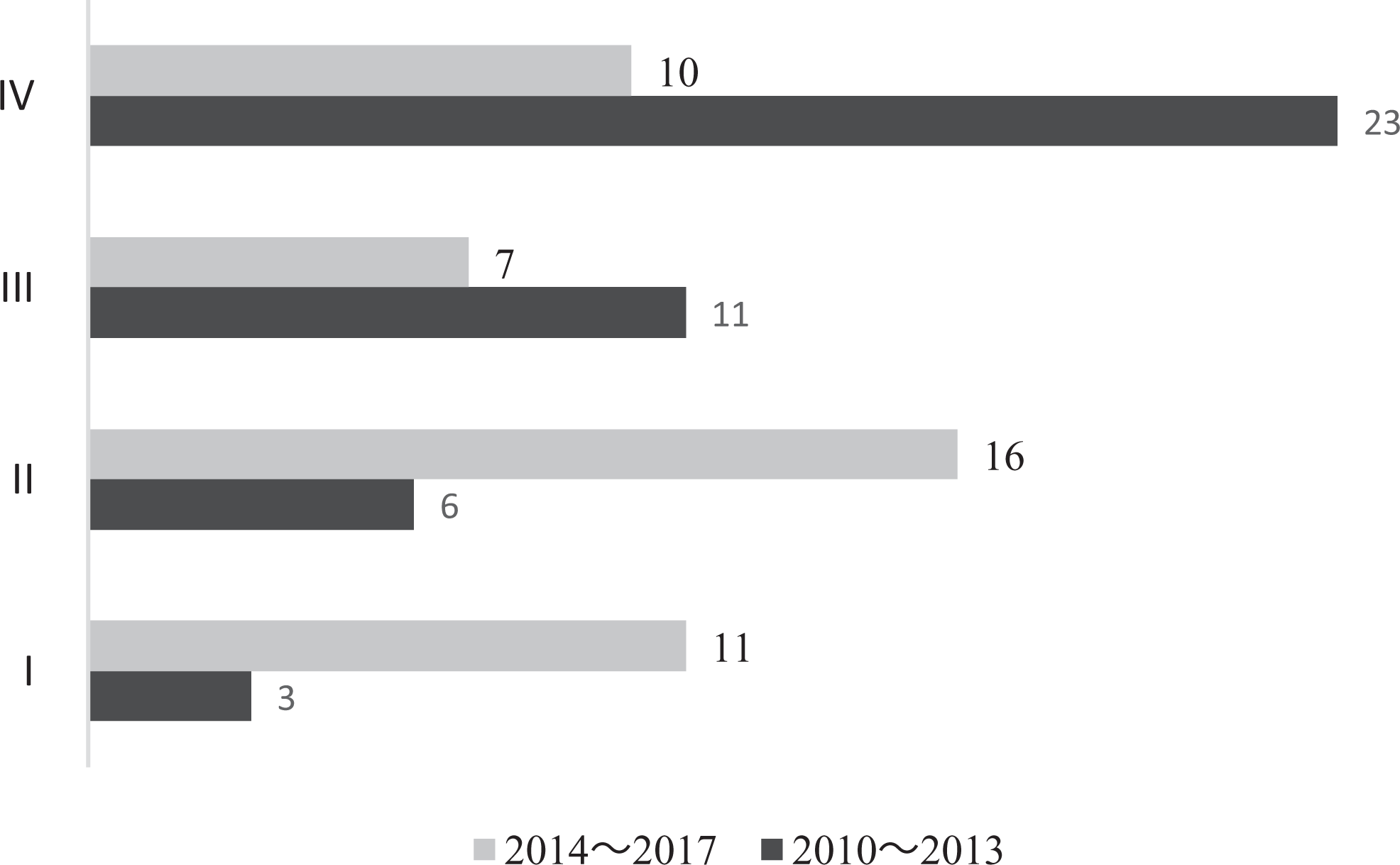
Number of cases according to disease stage in 2010 to 2013 and 2014 to 2017.
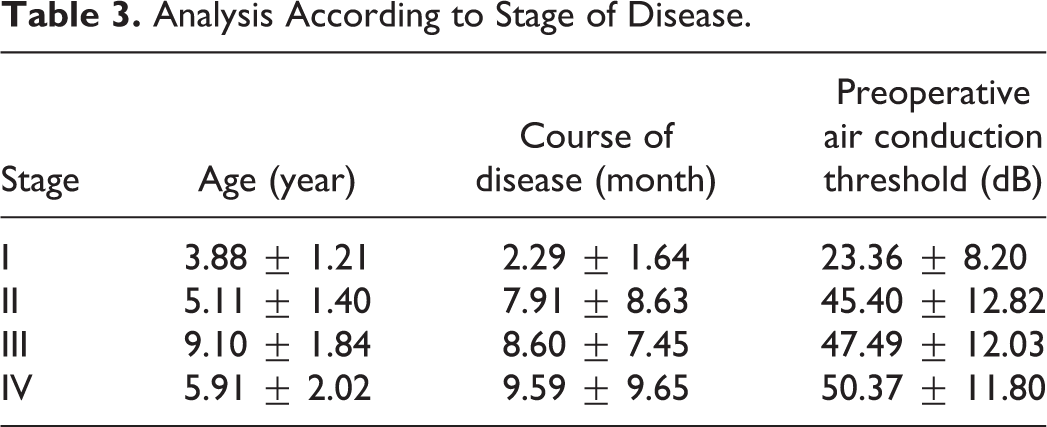
As shown in Table 3, the mean age at the time of surgery was 3.88 ± 1.21 years for stage I disease, 5.17 ± 1.40 for stage II, 9.09 ± 1.84 for stage III, and 5.91 ± 2.01 for stage IV. The differences in age between stages II/III/IV and stage I are statistically significant (PI-II = .004, PI-III = .000, and PI-IV = .000, respectively). The preoperative air conduction threshold in patients with stage I disease was significantly lower than that of stages II, III, and IV (PI-II = .000, PI-III = .000, and PI-IV = .000, respectively). The course of the disease was shorter in patients with stage I disease than in those with stages II, III, and IV (PI-II = .043, P I-III = .009, and PI-IV = .038, respectively).
Analysis According to Stage of Disease.
Of patients with stages I-II disease (early group, 77.77%) were asymptomatic, whereas the chief complaint was hearing loss (94.12%) in those with stages III-IV disease (advanced group). In addition, peripheral facial paralysis was found preoperatively in 1 patient with stage III and 2 with stage IV disease. In terms of means of diagnosis, otoscopy (fiber or rigid) was the most frequent (52.78%) in the patients with early disease, whereas more patients (92.16%) in the advanced group were diagnosed by CT scan. Based on intraoperative morphologic findings, 21 patients (58.33%) had closed-type cystic masses in the early group, whereas 49 (96.08%) had open-type lesions in the advanced group. There were significant differences in the chief complaint, means of diagnosis, and morphology of CC between the early and advanced groups (Table 4).
Analysis According to Stage of Disease.
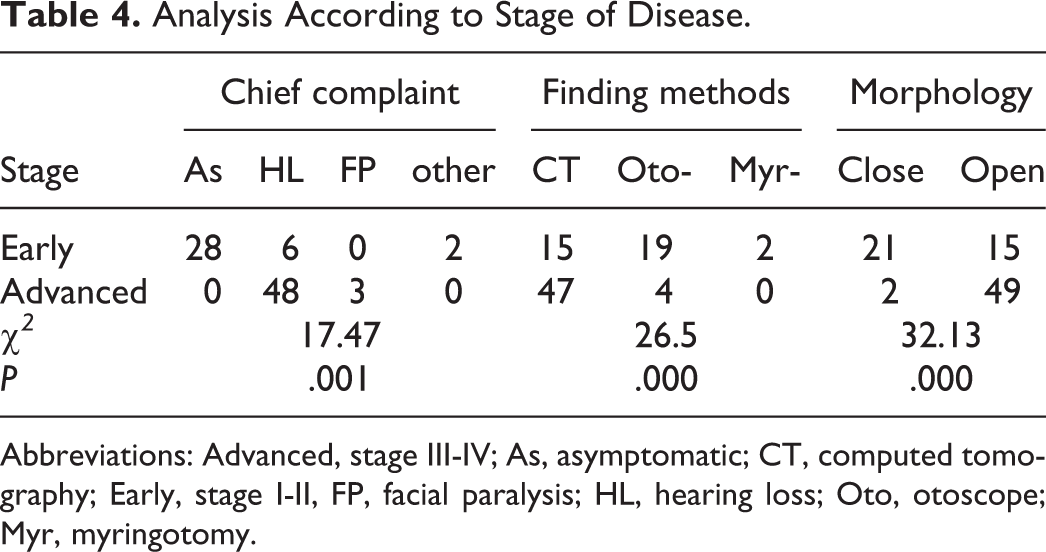
Abbreviations: Advanced, stage III-IV; As, asymptomatic; CT, computed tomography; Early, stage I-II, FP, facial paralysis; HL, hearing loss; Oto, otoscope; Myr, myringotomy.
Ossicular erosion was found intraoperatively in 58.62% of all patients, 32.18% having stapes lesions. The disease was classified into the following 3 grades according to the degree of ossicular chain injury: grade 1, no damage to ossicular chain; grade 2, involvement of ossicles excluding the stapes; and grade 3, involvement of ossicles and stapes. The preoperative air conduction thresholds in the 3 grades were 24.13 ± 8.51, 42.14 ± 14.93, and 49.03 ± 12.09 dB, respectively; these differences are statistically significant (P0–1 = .00; P0–2 = .00; and P1–2 = .04).
In the early group, TEA was performed in 63.89% of patients, CWU+T in 30.56%, and CWD+T in 5.55%, whereas in the advanced group CWU+T was performed in 66.67% of patients, TEA in only 11.76%, and the rest was CWD+T (21.57%). These differences in the choice of surgical procedure between the 2 groups are significant (P = .000). Overall, 11 patients (12.64%) had recurrence after surgery, 2 of whom had 2 recurrences (Table 5). Only 2 of the recurrences occurred in the early group, the remaining 9 (81.88%) occurring in the advanced group. The main complications were otalgia, dizziness, nausea, vomiting, and facial paralysis. One patient with facial paralysis in HB′ grade 3 (House-Brackmann grading system) recovered to normal after 2 weeks of conservative treatment. Figure 2 and 3 showed the closed cholesteatoma and open cholesteatoma respectively.
Type of Surgery, Recurrences, and Complications According to Stage.
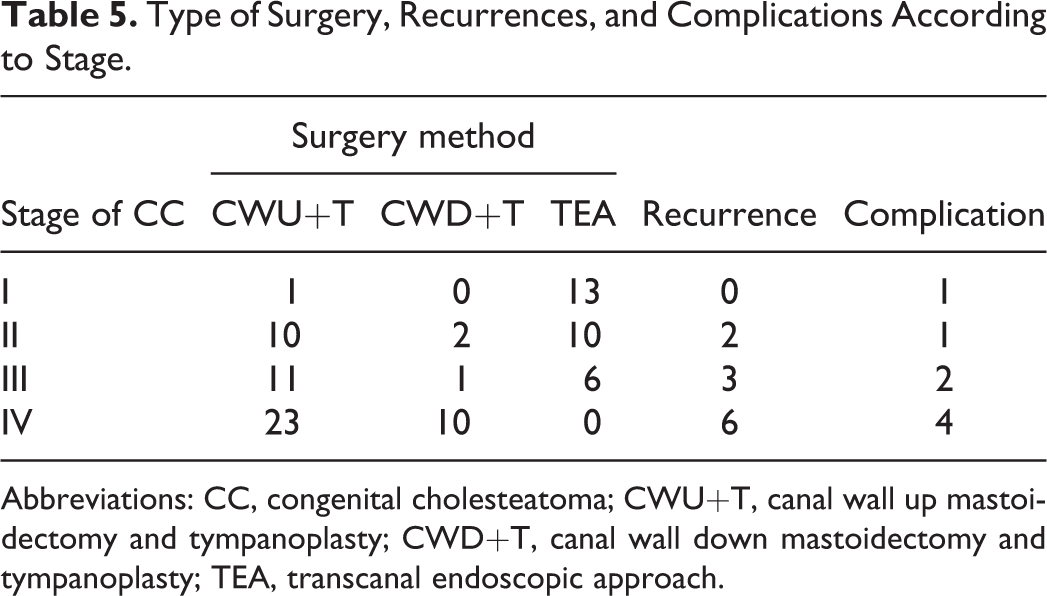
Abbreviations: CC, congenital cholesteatoma; CWU+T, canal wall up mastoidectomy and tympanoplasty; CWD+T, canal wall down mastoidectomy and tympanoplasty; TEA, transcanal endoscopic approach.
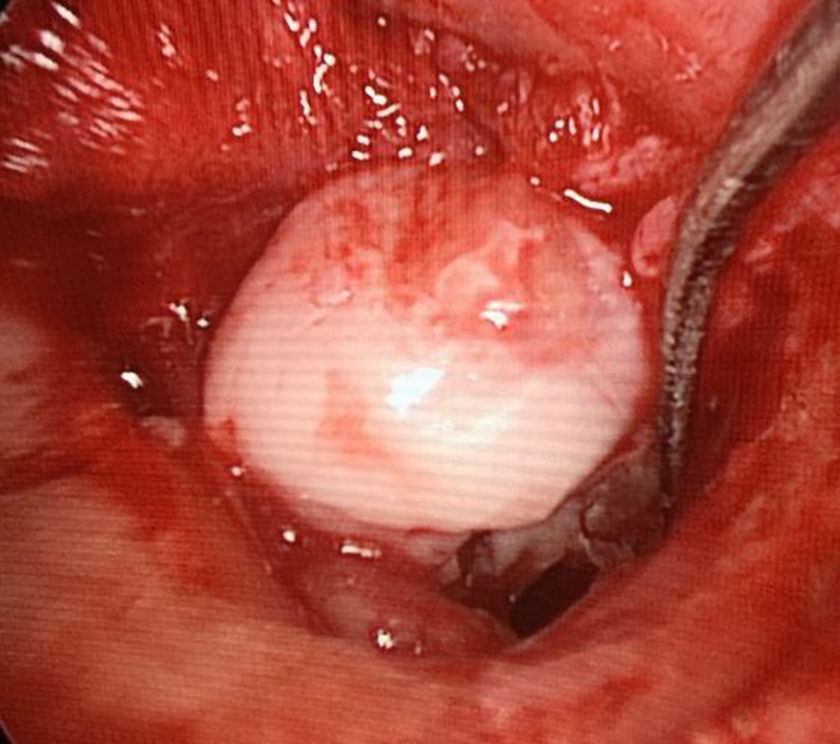
Closed cholesteatoma of middle ear under otoendoscopy.
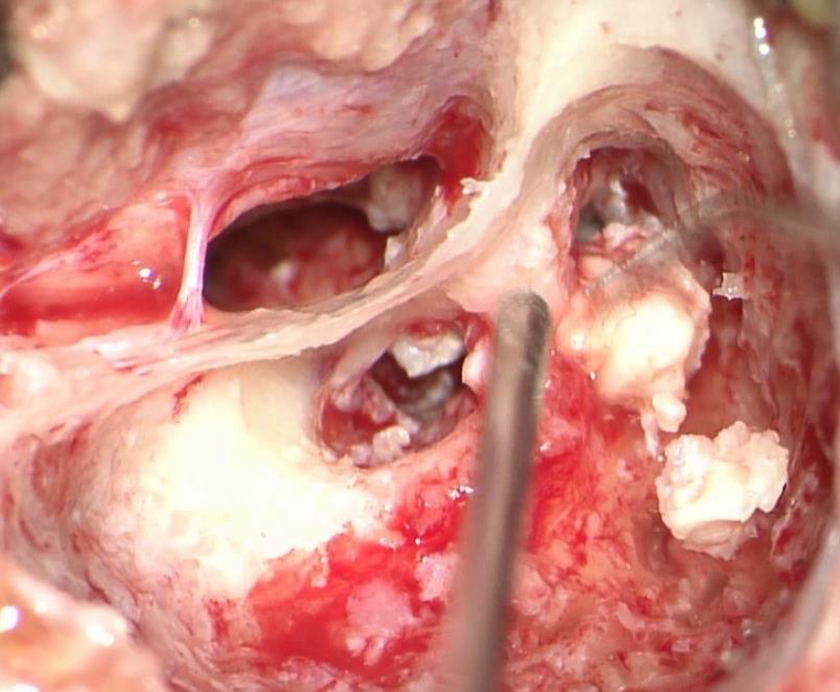
Open cholesteatoma of middle ear under microscope.
Eleven recurrent cases were found in all of the patients postoperatively. Four of them were finally diagnosed by MRI, who have difficulty in CT scan and otoscopy confirming recurrence of cholesteatoma in the middle ear. To determine the causes of recurrence of the disease, various factors were studied, including age at surgery, morphology, stage, invasion of ossicles, and surgical procedure. As shown in Table 6, the stage was the only examined factor that significantly affected the incidence of recurrent disease (P = .02).
Univariate Analysis of Risk Factors Affecting Recurrence of CC.
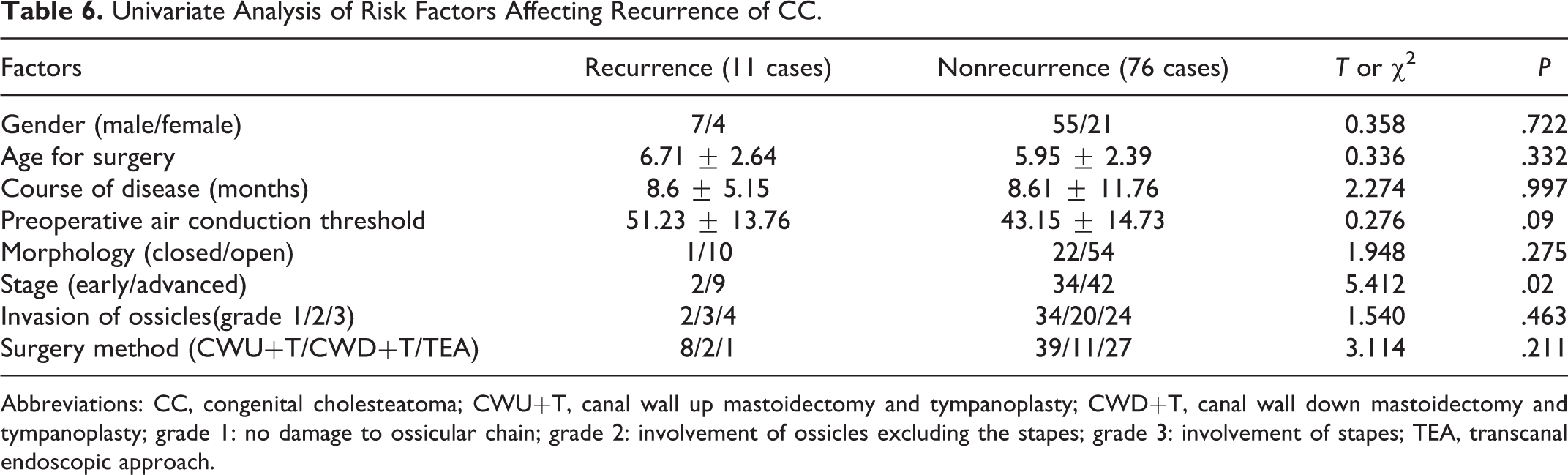
Abbreviations: CC, congenital cholesteatoma; CWU+T, canal wall up mastoidectomy and tympanoplasty; CWD+T, canal wall down mastoidectomy and tympanoplasty; grade 1: no damage to ossicular chain; grade 2: involvement of ossicles excluding the stapes; grade 3: involvement of stapes; TEA, transcanal endoscopic approach.
In addition, the 2 patients with recurrent in the early group had undergone endoscopic surgery, whereas the remaining 9 patients who developed recurrences in the advanced group had undergone microscope-assisted surgery. As shown in Figure 4, microscope-assisted surgery was performed on 26 patients in the advanced group from 2010 to 2013; thus, the recurrence rate in this subgroup was 26.92% (7/26). In contrast, the corresponding recurrence rate was 8.33% (2/24) from 2014 to 2017, this reduction being associated with the use of microscopic and endoscopic surgery. However, this difference was not statistically significant (χ2 = 2.922, P = .087).
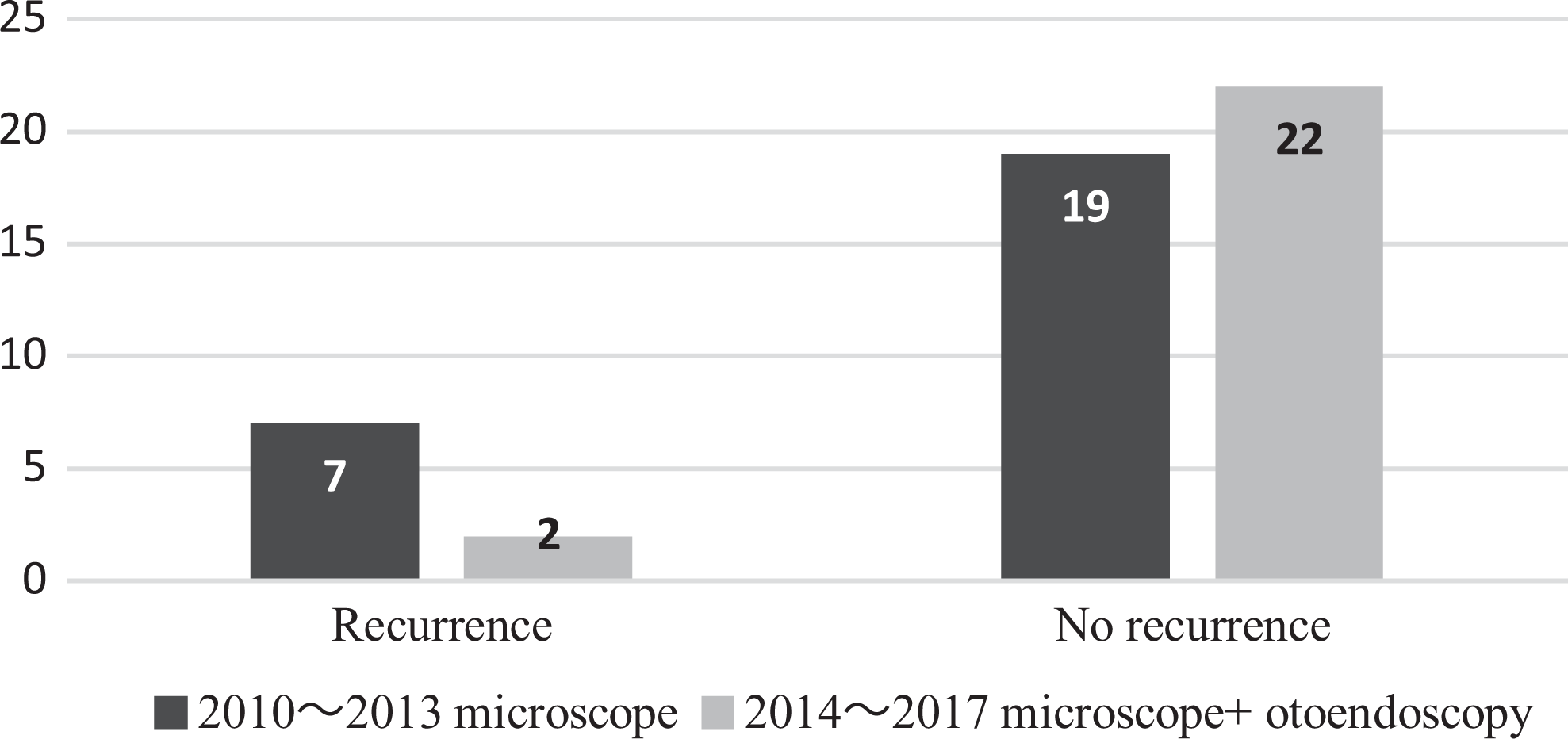
Factors affecting the incidence of recurrence of CC in the advanced group. CC indicates congenital cholesteatoma.
Discussion
The number of patients diagnosed as having CC has increased recently due to greater interest in pediatric otitis media, improved diagnostic tools such as pneumatic otoscopes and endoscopes, and the prevalence of audiometric screening procedures. 6 Although there was no difference in the number of cases between 2010-2013 and 2014-2017, there was a major change in the stage of CC. During the last most recent years, the number of patients with stage I-II disease increased notably, whereas the number of patients with stage III-IV disease decreased (Figure 1). The same trend has been found in many recent studies,7,8 suggesting that CC is now diagnosed earlier than it was previously. Because the growth of CC is closely linked to patient age and delays in detection and treatment may facilitate extension of the disease, early diagnosis, and surgical intervention is crucial.9-11
Among the lesions involving 1 or 2 quadrants, the most common location was the PSQ (74.07%; Table 2). During surgery, cholesteatoma was often found to be originating from the incudostapedial joints and extending into the surrounding space. Congenital cholesteatomas can occur anywhere in the temporal bone but have a predilection for the ASQ of the middle ear. Most CCs reportedly arise in the ASQ and grow into the PSQ, eroding ossicles and finally invading the mastoid.12,13 Many investigators have suggested that the closed type of cholesteatoma first develops at the tendon of the tensor tympani muscle, the cochleariform process, or the posterior side of the malleus.14,15 In contrast, other researchers have found that the PSQ is the most common location of cholesteatoma. 16 A meta-analysis conducted by Hidaka et al 17 found that the ASQ is less frequently involved in Asian than in Western patient cohorts and that in Asian cohorts the PSQ is more frequently involved than the ASQ. The origin of disease is uncertain in many patients with advanced disease; thus, the location of the origin can more accurately be determined in patients with early disease. 18 Stage I-II accounted for only 41.38% of cases in our series, making it difficult to accurately analyze the origin of the cholesteatomas.
Compared with other stages, the patients in our study with stage I CCs had the youngest age of onset, shortest duration, and mildest preoperative hearing impairment (Table 3), again emphasizing the importance of early detection of lesions.
In the early group (stage I-II), 77.77% of patients had no symptoms, their CCs having been found incidentally during routine physical examinations or hearing screening (Table 4). Lim et al 9 reported that 70.8% of their patients were asymptomatic at the time of diagnosis in their 2012 study. In contrast, most of the patients in the advanced group (stage III-IV) had varying degrees of conductive hearing loss. The mean preoperative air conduction threshold in patients without ossicular erosion is 24.13 dB. As the lesion invades the ossicular chain, hearing decreases significantly. Some researchers have emphasized early detection of the disease using otoscopic, audiologic, and radiologic evaluations in children with conductive hearing loss; these researchers have suggested a screening program for school children. 19 In terms of the means of diagnosis, otoscopy (fiber or rigid) was the most frequent means in the early group (52.78%), whereas more patients (92.16%) were diagnosed by CT scan in the advanced group. It is therefore necessary to let parents know the importance of routine health examination, while strengthening training of community physicians in otolaryngology. In addition, we suggest that children with these findings should be referred to an otolaryngologist for confirmation of the diagnosis and definitive management. We found a significant (P = .000) relationship between morphology and stage of CC: patients with stage I-II disease had a higher proportion of closed type (58.33%), whereas those with advanced stage CCs mostly had open type (96.08%). Prasad et al drew a similar conclusion in their article. 20 As reported by El-Bitar et al, 13 the sizes of CCs tend to increase with age at the time of surgery. The linear correlation between mass volume and age suggests that cystic CCs grow steadily and proportionately over time.
Surgical resection is the preferred method of treatment. Various surgical approaches can be selected according to the size, location, and stage of the CC. In the early group, TEA was performed on 63.89% of patients, none of whom developed recurrences. Except for 1 patient with mild earache, most patients had no postoperative complications. Transcanal endoscopic approach can provide better visualization of hidden areas and has become increasingly popular in surgery for middle ear disease. Transcanal endoscopic approach is a proved effective surgical option for patients with early stages of CC and is preferable for children because it is less invasive.21,22 It has been pointed out that performance of TEA using endoscopes of diameter 2.7 mm requires that the diameter of the external ear canal be more than 4.5 mm, as ascertained by CT scanning. 23 Because there were more patients in the advanced than the early group in our series, particularly those with stage IV disease (37.93%), the most common surgical procedure was CWU+T, this being performed on 51.72% of all patients and 66.67% of patients with stage IV disease. The ultimate goals of surgery are eradication of keratinizing squamous epithelium from bone and preservation or restoration of hearing. 24 Maintaining the integrity of the structure of the ear can improve the rate of successful restoration of hearing, especially in children. Prasad et al reported that hearing recovery is excellent with CWU procedures, remaining stable over 5 years in their study of 40 patients. 24 The CWU+T procedure should be performed as far as possible on children with advanced stages of CC. However, it is not advisable to perform CWU in certain situations, such as extensive disease, low lying dura, anterior placed sigmoid, and destruction of the ear canal, for which CWD should be considered. 25 Canal wall down mastoidectomy and tympanoplasty was performed on 13 patients (14.94%) overall and 21.57% of patients in the advanced group.
Pediatric CC tends to be more aggressive and extensive than CC in adults and is associated with a higher rate of recurrence. 26 In our study, the overall recurrence rate of pediatric CC was 12.64% (11/87) at the final postoperative follow-up. The reported recurrence rate of CC is between 5.7% and 26.7%.27-29 The considerable variation in published recurrence rates is attributable to the different types and stages of CC, surgical procedure, and duration of follow-up. Four of them were finally diagnosed by MRI, who have difficulty in CT scan and otoscopy confirming recurrence of cholesteatoma in the middle ear. To determine the causes of recurrence, some relevant factors were studied, including age at surgery, morphology, stage, invasion of stapes, and surgical procedure. Of these, we found that stage was the only significant risk factor affecting the incidence of recurrence of the disease (Table 6). The recurrence rate was 2.7% and 19.61% in the early and advanced groups, respectively (P = .02). Therefore, stage I or II CCs can be removed with a low risk of recurrence because these lesions are not extensive. We further explored the relationship between means of performing surgery and recurrence and found that 81.82% (9/11) of patients with recurrence had stage Ⅲ-Ⅳ disease and had undergone microscope-assisted surgery. The recurrence rate was higher after surgery between 2010 and 2013 than after 2014, likely because of the dependence on microscopy alone. From 2014, surgery was increasingly performed with a microscope and an endoscope, and the recurrence rate dropped significantly to 8.33%. In particular, angled endoscopes provide a clearer view of otherwise hidden places, enabling the surgeon to more thoroughly eradicate the lesion.30,31 Although this apparent difference was not statistically significant (P = .087), the surgery performed under microscope and an endoscope shows us the possibility of reducing the recurrence rate of CC. May be the small sample size may account for the lack of statistical significance.
Conclusions
Patients with stage I disease are mostly asymptomatic and can undergo TEA surgery with minimal damage and a good prognosis. In comparison, conductive hearing loss is the most common complaint in pediatric patients with stage Ⅲ-Ⅳ CC. The more advanced the lesion, the greater the risk of recurrence of CC. Undoubtedly, these findings emphasize the importance of early detection and management of CC and thus avoidance of advanced disease. It is recommended that this operation be performed aided by both a microscope and endoscope to facilitate complete elimination of the lesion and reduction of the recurrence rate.
Footnotes
Authors’ Note
There is compliance with ethical standard in the research. All procedures performed in studies involving human participants were in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Acknowledgments
The authors wish to thank Dr Xin NI and Dr Jie Zhang for guidance and help with this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by The Beijing Municipal Administration of Hospitals Clinical technology innovation project [XMLX201701], The Capital health research and development of special project (2016-1-5014) and The Special Fund of The Pediatric Medical Coordinated Development Center of Beijing Hospitals Authority(XTYB201828)