
Abstract
Congenital cholesteatoma is a whitish mass in the middle ear medial to an intact tympanic membrane. It is often without symptoms and therefore incidentally diagnosed. Pediatric congenital cholesteatoma generally starts as a small pearl-like mass in the middle ear cavity that eventually expands to involve the ossicles, epitympanum, and mastoid. The location, size, histopathological type, and extent of the mass must be evaluated to select the appropriate surgical method. Although microscopic ear surgery has traditionally been performed to remove congenital cholesteatoma, a recently introduced alternative is endoscopic surgery, which allows a minimally invasive approach and has better visualization. Here, we report the first known case of a patient with congenital cholesteatoma in the anterior epitympanic recess and discuss the utility of an endoscopic approach in the removal of a congenital cholesteatoma in the hidden area within the middle ear.
Introduction
Congenital cholesteatoma (CC) is a whitish mass that develops in the middle ear medial to an intact tympanic membrane in patients with no history of perforation or otorrhea or of otologic surgery. 1 According to the literature, the range in prevalence of CC is from 4% to 24% of cholesteatomas in children and 2% to 5% of all cholesteatomas. 2 It is most commonly report as an incidental finding. The reported ratio of CC in males versus females is 3:1. 3 The treatment goals for CC are complete surgical removal and the prevention of recurrence. The complete removal of a cholesteatoma is essential because the recurrence rate is high even when a small piece of the cholesteatoma matrix remains in the tympanum. 4 In the management of pediatric CC, transcanal endoscopic ear surgery (TEES) has been shown to provide a good alternative to traditional microscopic ear surgery. 5
Here, we report the first known case of a patient with CC in the anterior epitympanic recess and discuss the utility of the endoscopic removal of CC in hidden areas within the middle ear.
Case Presentation
A 4-year-old female infant was referred to our hospital on January 19, 2019, after her local doctor incidentally detected a whitish mass in the tympanic membrane of her left ear. She had no otologic symptoms and the results of brainstem electric response audiometry were normal. Otoscopic examination revealed a whitish soft tissue mass behind the annulus of the intact tympanic membrane, within the anterosuperior quadrant (Figure 1A). A computed tomography (CT) scan of the temporal bone showed a soft tissue density extending from the anterior epitympanic recess to the eustachian tube (Figure 1B). However, there was no bony erosion in the tegmen or destruction of the ossicles. These findings suggested that the CC was limited to the middle ear.
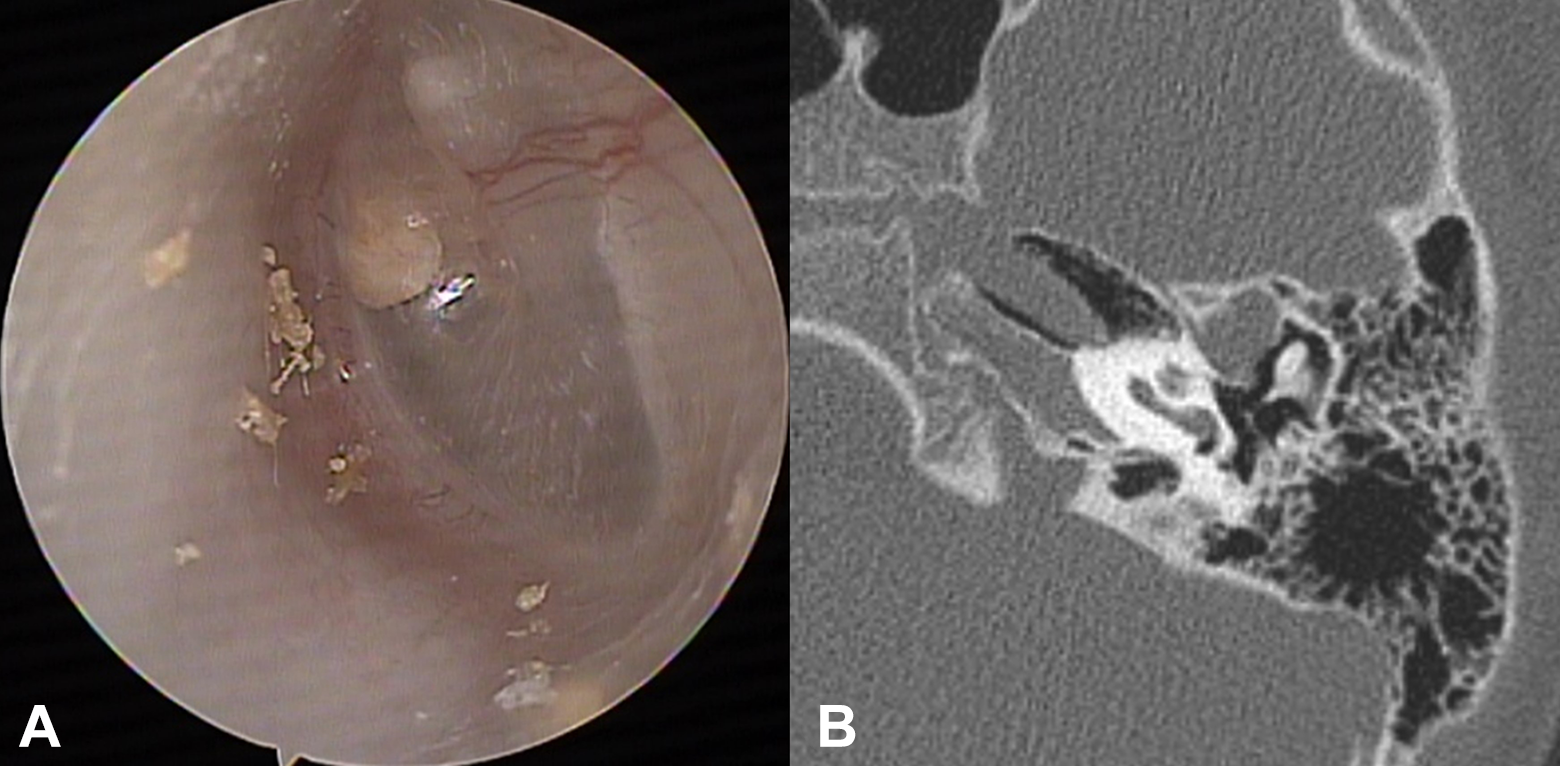
A, Otoscopic examination revealed a whitish soft tissue mass behind the annulus of an intact tympanic membrane, within the anterosuperior quadrant. B, On the computed tomography scan, an isolated soft tissue shadow was seen in the anterior epitympanic recess without destruction of the ossicles.
The patient was placed under general anesthesia and TEES was performed to remove the mass. A tympanomeatal flap was raised after a skin incision along the tympanic annulus at 6-o’ and 12-o’clock positions with holding the 0° endoscope in the left hand and the flap was lifted forward to expose the anterosuperior mesotympanic area. The tympanic membrane was dissociated gently from the malleus with a sickle knife to completely visualize the protympanum. After the removal of the portion of the mass in the protympanum, the remainder, located in the anterior epitympanic recess, was completely eliminated under 30° endoscopy while preserving the ossicles (Figure 2).
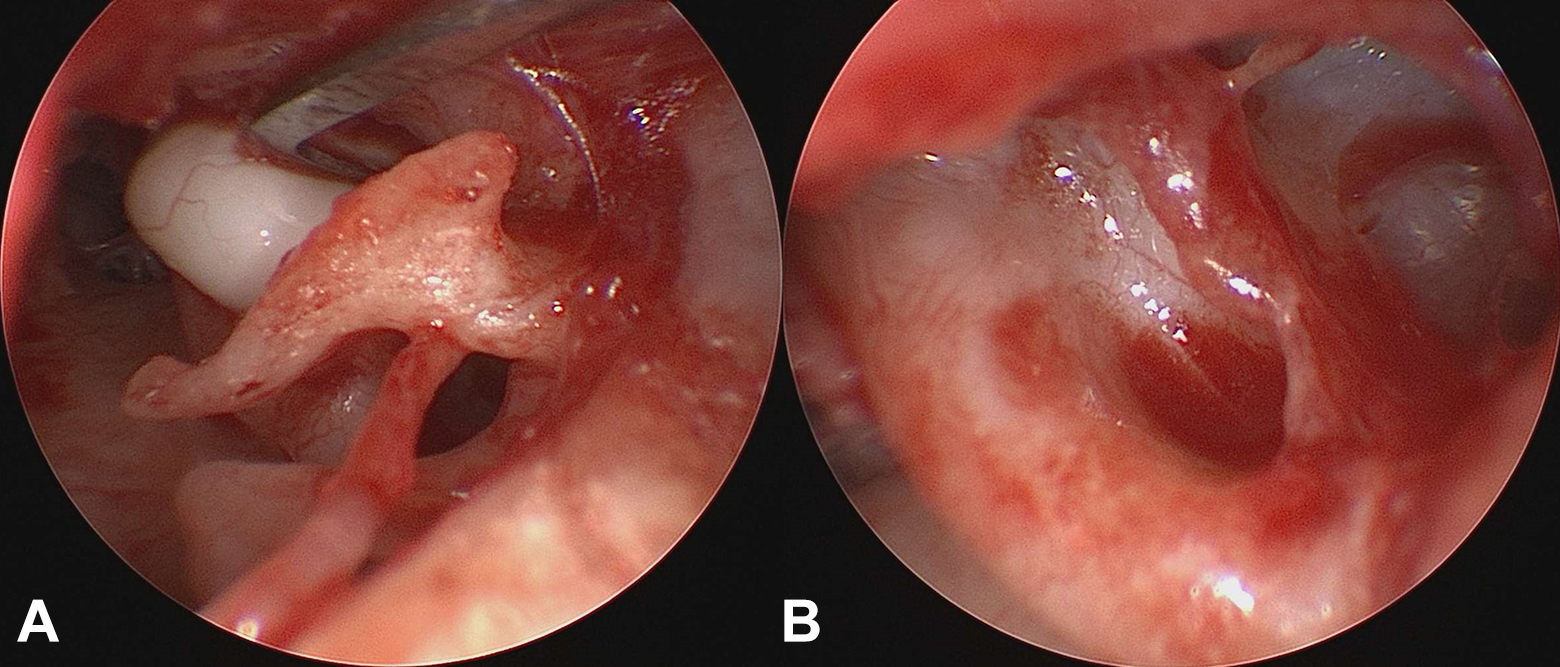
The whitish mass in the anterior epitympanic recess was completely eliminated under 30° endoscopy while preserving the ossicle.
The pathological diagnosis confirmed cholesteatoma and noted the presence of keratin debris. At 12 months after surgery, the patient had normal hearing on the pure tone audiometry and no opacification in the middle ear was observed on the CT image. We are monitoring the patient every 6 months and no recurrence of CC has been observed so far.
Discussion
The origin of CC remains uncertain, but among the possible mechanisms leading to the occurrence of epidermal tissue in the middle ear with a normal tympanic membrane, those based on the inclusion theory, the amniotic fluid contamination theory, the migration theory, and the epidermoid formation theory have been proposed.
According to a review, in 66% of patients with CC is detected in investigations of hearing loss or during the follow-up of acute otitis media or otitis media with effusion. However, in the remaining 34%, CC is incidentally diagnosed by routine otoscopy or during otologic screening. 6
Based on its histopathology, CC can be divided 2 types: the closed type, which presents as an epithelial cyst without keratin exposure, and the open type, characterized by exposure of the cholesteatoma matrix that forms part of the middle ear mucosa. 7 The most common site of CC is the anterosuperior quadrant of the middle ear, but it does not consistently remain confined there. Rather, CCs tend to grow toward the posterosuperior quadrant and the attic and then finally into the mastoid. 8
The treatment of CC is surgical, with eradication of the cholesteatoma matrix from the middle ear and the preservation or restoration of hearing. The surgical method will depend on the location, size, histopathological feature, and infiltration range of CC. Given that, in pediatric patients, it is difficult to visualize the middle ear cavity completely with a microscope through the ear canal, in traditional CC removal, a postauricular approach is preferred. However, recent advances in endoscopic technology have allowed the use of endoscopic approaches that avoid the limitations of microscopic surgery through the ear canal.
Transcanal endoscopic ear surgery provides better visualization of middle ear structures, thus facilitating the removal of CC in hidden areas within the middle ear. In addition, it is minimally invasive and obviates the need for a postauricular incision—a particular advantage in pediatric patients, in whom the external ear canal is small and preserves the mastoid tissue. 9
In the majority of patients, CCs occur in the anterosuperior quadrant, mostly as a whitish mass behind the ear drum and adjacent to the malleus. However, on otoendoscopy, the CC in our patient was seen near the annulus of an intact tympanic membrane. The CT scan revealed an isolated soft tissue shadow in the anterior epitympanic recess, without destruction of the ossicles. During surgery, however, extension of the CC to the eustachian tube, in the anterior epitympanic recess, was determined. Thus, it is likely that the CC occurred in the anterior epitympanic recess and then invaded the eustachian tube via the tensor tympanic fold. The CC was successfully eradicated using an endoscope without removing the ossicles, even though the mass was located completely in the anterior epitympanic recess. This location of a CC has not been previously reported.
Conclusion
The location, size, histopathological type, and extent of the mass in pediatric CC should be carefully evaluated to determine the appropriate surgical method. Especially in pediatric patients with CC limited to the middle ear cavity, TEES may be a good alternative to traditional microscopic ear surgery because it allows better access to hidden sites in the ear, such as the anterior epitympanum, facial recess, and sinus tympani.
Footnotes
Authors’ Note
The patient’s parents have provided informed consent for publication of the case and the accompanying images.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article This study was supported by the Bio & Medical Technology Development Program of National Research Foundation of Korea (NRF) funded by the Korean government MSIT (NRF-2019M3E5D1A02067955) and a grant (HCRI20015) Chonnam National University Hwasun Hospital Institute for Biomedical Science.