
Abstract
Keywords
Case
A 25-year-old man was referred to our clinic for evaluation of episodic drainage of a sinus tract in his left neck associated with swelling and pain, especially with respiratory tract infections. Physical examination revealed a cutaneous tract opening anterior to the lower sternal border of the left sternocleidomastoid. Palpation of the left neck expressed a small amount of purulent fluid. There were no abnormalities of the tonsillar fossa.
The tract was cannulated with a 4F catheter, and 8 mL of Isovue-370 (Iopamidol injection 76%) radiopaque contrast agent was instilled. A fistulogram revealed the tract extended superiorly along the anterior border of the sternocleidomastoid muscle, ending in a blind pouch near the level of the thyroid cartilage (Figure 1A). No contrast entered the tonsillar fossa. A post-procedural computed tomography (CT) scan of the neck was performed, which confirmed the tract coursing lateral to the trachea and thyroid cartilage, ending in a blind pouch at the level of the thyroid cartilage (Figure 1B).
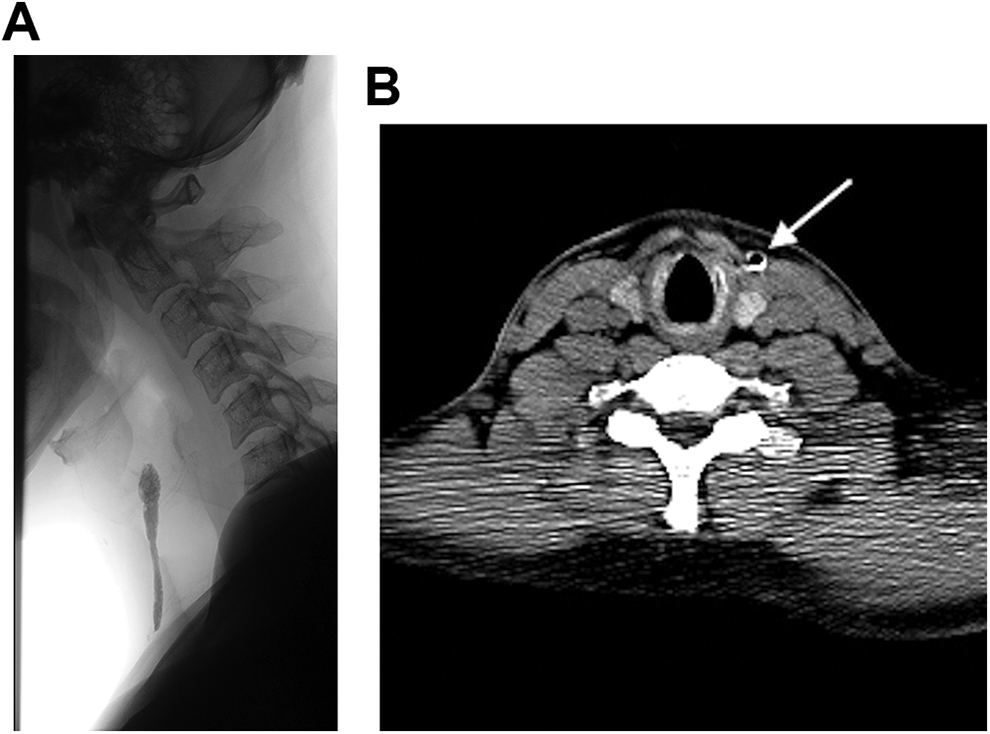
A, Lateral spot fluoroscopic exposure demonstrates contrast within the sinus tract in the anterior neck with a blind end at the level of C5-C6 vertebral body. B, Axial CT of the neck at the level of the cricoid cartilage shows the sinus tract anterior lateral to the strap muscles and medial to the sternocleidomastoid muscle in the left neck, marked by a white arrow. The sinus is filled partially by contrast (white rim) and air (dark center). The CT scan is available online as Supplemental Movie 1.
Under general anesthesia, a 24-gauge Angiocath was placed into the cutaneous sinus while instilling normal saline. A cuff of skin around the tract was incised. The tract was dissected superiorly and passed under the submandibular gland and stylohyoid muscle, entering into the tonsillar fossa. The tract was ligated, flush with the oropharyngeal mucosa, and marked with surgical clips. The gross specimen was sent for pathology evaluation (Figure 2). Histopathologic examination confirmed a branchial cleft cyst of the proximal portion, with the distal portion being nonpatent and comprised of skeletal muscle and focal fibrosis without epithelial lining or cyst wall (Figure 3). Written, informed consent was obtained from the patient for publication of this case.
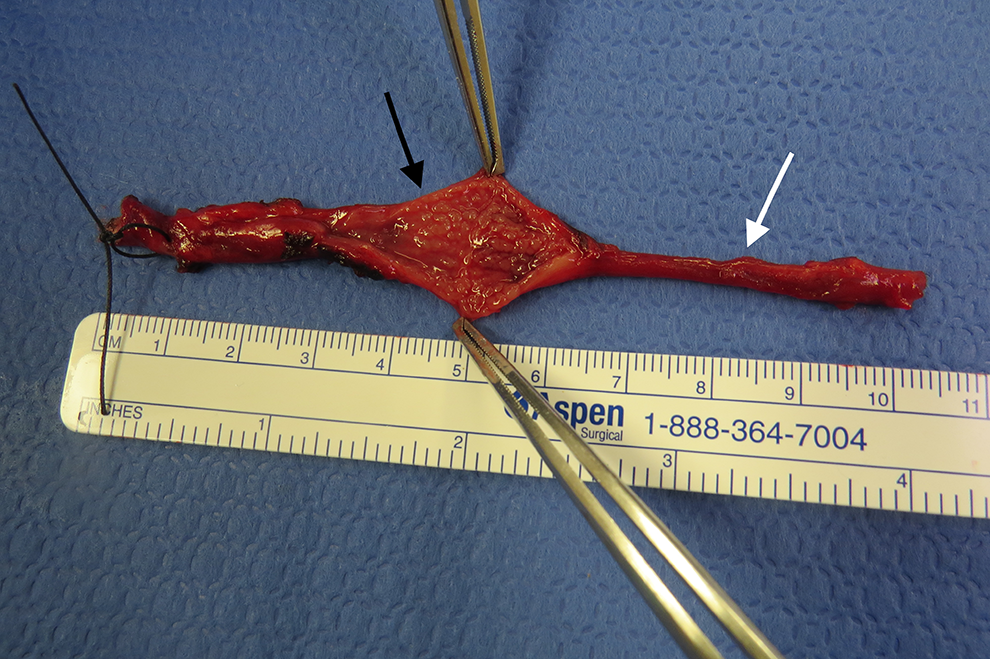
Gross specimen of branchial cleft sinus with stitch at cutaneous end. The sinus tract is incised at its widest point (black arrow), revealing a patent tract. The fibrous portion was incised with no patent tract noted (white arrow).
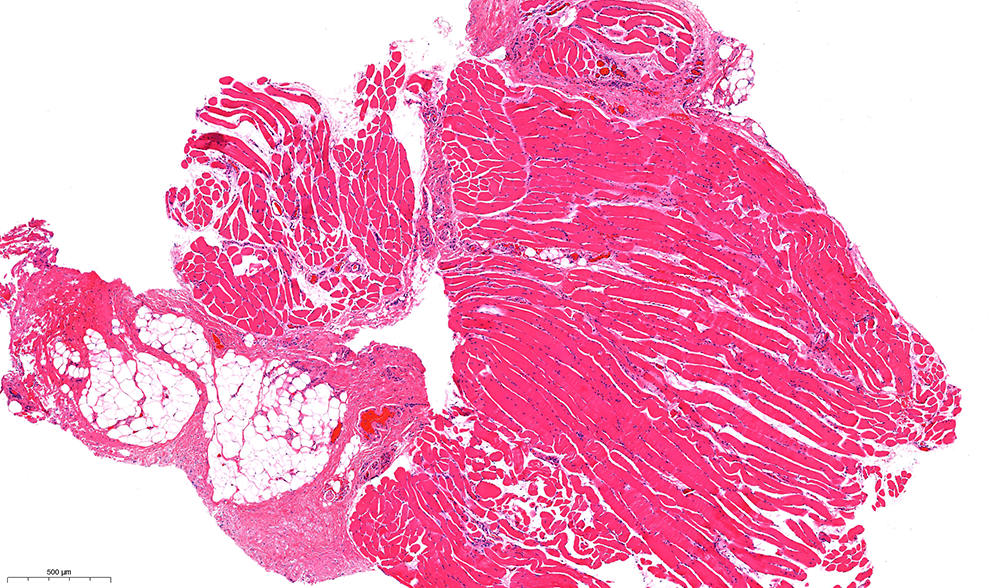
Photomicrograph of the branchial cleft sinus corresponding to the white arrow, showing skeletal muscle, focal fibrosis, and adipose tissue with no sinus tract or lining epithelium identified (40×).
Discussion
Congenital anomalies of the branchial apparatus are relatively common, accounting for approximately 17% of pediatric neck masses. 1 They frequently present as masses that enlarge in association with respiratory tract infections. If a tract opening in the skin is identified, it is highly suggestive of a branchial cleft anomaly. 2 Most commonly, they arise as fistulas or sinuses from the 2nd branchial apparatus. 3 Surgery is recommended, as branchial cleft anomalies frequently recur unless removed.
Various radiologic modalities are available to define the extent of branchial cleft anomalies. Ultrasound is the initial imaging modality of choice for some clinicians due to its low cost and ease of performance. 4 This modality may not fully define the extent of a branchial cleft fistula or sinus, however. In a review of 17 patients who underwent ultrasound for a branchial cleft anomaly, 3 (17.6%) had fistulous/sinus tracts that were not identified preoperatively. 5
Computed tomography offers detailed, 3-dimensional images of suspected branchial cleft anomalies. It has been advocated as the imaging modality of choice for diagnosis of occult sinus tracts that may be difficult to identify otherwise. 6 This modality is also useful for delineating the course of nearby structures and identifying anatomical variants. Magnetic resonance imaging (MRI) avoids the radiation associated with CT imaging but is rarely the imaging modality of choice for the evaluation of branchial cleft abnormalities, as a CT scan is more readily available, faster, and better tolerated by young children.6,7
The use of fistulograms has previously been described in the literature and was the traditional means of evaluating branchial cleft anomalies prior to the widespread use of CT and MRI.3,8 The value of this study has been disputed, with some authors arguing that such imaging is unnecessary for defining the extent of a branchial cleft anomaly. 9 Computed tomography fistulography, utilizing CT after instilling radiopaque dye into the branchial cleft tract, has more recently been described.10,11 The case reports in the literature using this technique are promising, combining the complete tract visualization of traditional fistulogram with the spatial resolution of modern CT scanners.
In the case presented in our paper, CT fistulography demonstrated a contrast-filled tract on the CT which allowed for excellent discrimination of the course of the tract in comparison to nearby neurovascular structures. Additionally, CT fistulography suggested that the tract ended in a blind pouch at the level of the thyroid cartilage rather than coursing into the tonsillar fossa as in a complete fistula. This was confirmed on postoperative histopathologic examination of the tract, which demonstrated a nonpatent cord extending from a blind ending pouch to the tonsillar fossa. This was helpful for postoperative counseling for the patient, suggesting that recurrence or persistence of a fistulous tract was less likely. Though controversy exists in the literature regarding optimal management, preoperative CT fistulography is useful in selected cases of suspected branchial cleft anomalies.
Supplemental Material
Supplementary_Video_Description - CT Fistulography and Histopathologic Correlates for Surgical Treatment of Branchial Cleft Sinuses
Supplementary_Video_Description for CT Fistulography and Histopathologic Correlates for Surgical Treatment of Branchial Cleft Sinuses by Ryan K. Thorpe, Bruno Policeni, Renee Eigsti, Xin Zhan and Henry T. Hoffman in Ear, Nose & Throat Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Hoffman reports involvement as a research consultant for iota Motion, Inc. and as an author for UpToDate. Otherwise there are no conflicts of interest to disclose for this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported in part by NIH-NIDCD grant 5T32DC000040 (RKT).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.