
Abstract

A 43-year-old man presented with dysphagia, fever, and a generalized skin rash (Figure 1A). Chickenpox was suspected according to the presence of typical vesicles and absence of previous varicella-zoster virus (VZV) infection. Blood tests revealed abnormal liver function and immunoglobulin M antibody positivity (1.59 NovaTec Units [NTU]) and immunoglobulin G antibody negativity (0.98 NTU) against VZV. Upper endoscopy was performed because of persistent dysphagia. Multiple small target-like lesions were detected in the hypopharynx and larynx (Figure 1B). After administering antiviral agents, the symptoms improved and the patient was discharged from the hospital.
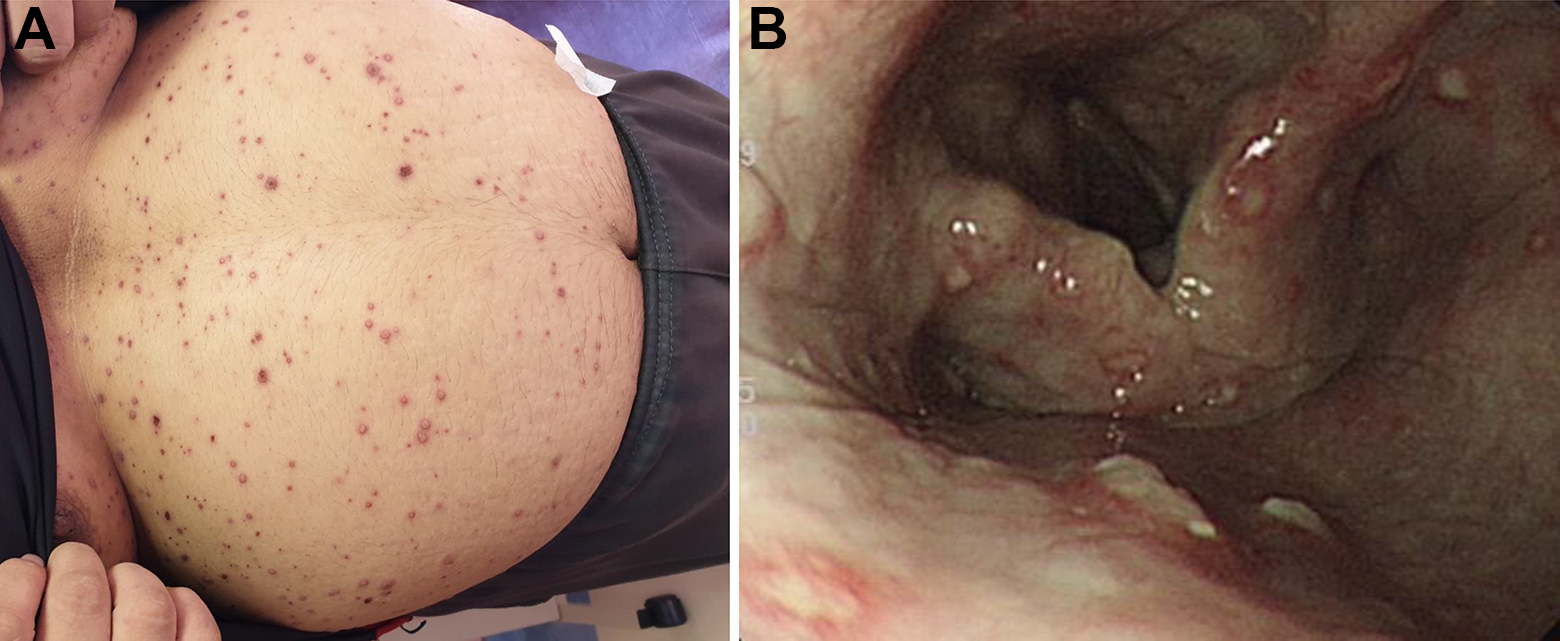
A, Vesicles are typical of infection due to varicella zoster virus. B, Upper endoscopy shows multiple small target-like lesions in the hypopharynx and larynx, which may cause dysphagia.
Chickenpox, which is prevalent globally, is caused by primary VZV infection. It is highly contagious and can be transmitted through contact with fluid from the skin vesicles of infected individuals. It is also an airborne disease, which is spread through coughing and sneezing. The clinical manifestations of chickenpox generally develop within approximately 2 weeks from exposure and include a prodrome of fever, malaise, and/or pharyngitis, followed by skin rashes, with small and itchy vesicles. In some cases, the mucous membranes in the mouth may be involved. Oral mucosal lesions begin as small vesicles, that quickly rupture and transform into slightly painful or painless, flat-based ulcers with erythematous halos, and a whitish/yellow or brown ulcer bed. 1 They can be seen on the lips, tongue, buccal mucosa, gingival, palate, and pharynx in small numbers (usually 1 to 7),2,3 with the vermilion of the lips and palate as the most common locations. 1 One study revealed that the prevalence and number of oral lesions are related to the severity of chickenpox. 1 All severe cases, which were defined as more than 200 skin lesions and a fever of more than 38 °C, presented with 5 to 30 oral lesions (average, 18 lesions). However, among mild cases, defined as fewer than 50 skin lesions and no fever, only 6 (31.5%) patients presented with 1 to 2 oral lesions. Similar presentations of oral mucosal lesions can also be seen in patients with herpes zoster (reactivation of latent VZV infection) or other viral infections, including herpes simplex virus and Coxsackie virus infections. This can sometimes lead to confusion and difficulties in clinical diagnosis. However, the characteristics of oral lesions and extraoral symptoms may help differentiate chickenpox from other viral infections. 3
Although the incidence of complications, hospitalization, and mortality have dramatically declined since the introduction of the varicella vaccine in 1995, severe complications including bacterial soft tissue infections, encephalitis, pneumonia, pharyngitis, and hepatitis have been reported occasionally, especially in adults and immunocompromised individuals. Pharyngitis and laryngitis induce sore throat and dysphagia and have a prevalence of 163 to 306 cases per 10 000 unvaccinated varicella patients, according to a previous report. 4 In one hospital cohort, laryngitis was a rare complication and only accounted for less than 1% of unvaccinated children. 5 Furthermore, gastrointestinal tract involvement has been rarely reported. The severity of gastrointestinal tract involvement varies from esophageal ulcers to gastric perforation.6,7 Although some studies suggested that gastrointestinal involvement is a manifestation of latent VZV reactivation, 8 the pathogenesis remains controversial. In our case, identification of the typical skin and oral manifestations aided the timely diagnosis and treatment of chickenpox. Upper endoscopy was performed for persistent gastrointestinal symptoms and to exclude pharyngolaryngeal and gastrointestinal complications. Multiple target-like lesions in the hypopharynx and larynx were identified. However, no remarkable lesions were noted in the esophagus, stomach, or duodenum. As visceral involvement occasionally occurs before the appearance of classic skin rashes, the contact history and pharyngolaryngeal lesions may be the only basis to diagnose chickenpox. The typical pattern of pharyngeal and laryngeal lesions in patients with chickenpox should be studied. To help reduce the severity of symptoms and theoretically to decrease the risk of complications, antiviral therapy should be administered for adult patients, regardless of their vaccination status. 9
Footnotes
Authors’ Note
Informed consent was obtained from all individual participants included in the study.
Acknowledgments
The authors thank the secretaries of the Hepatobiliary Division in Kaohsiung Medical University Hospital and Dr. Ning Ning Lee of the Otorhinolaryngology Department in More Grace E.N.T. Clinic for their help.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Ministry of Health and Welfare, Pingtung Hospital, and Kaohsiung Medical University Hospital.