
Abstract
Lasers have been used in otolaryngology for more than 40 years and are widely considered an established way of addressing laryngeal pathology, benign and malignant. Carbon dioxide (CO2) laser is considered a gold standard, but over the last 2 decades, a new technology has been developed and established in other medical specialties, not so much in Ear Nose and Throat (ENT), the diode laser. It consists of a flexible fiber that passes through a hollow guidance system and is capable of reaching certain angled spots easier than straight beam systems. Portability, lower cost, easier setup, and improved photocoagulation are just some of the many features rendering it an excellent choice for the surgeon and the patient. The few studies published worldwide for the usage and efficacy of this system show no major differences related to the oncologic outcome and survival rate of patients having an early glottic tumor between diode laser microsurgery and CO2 laser cordectomy. Nevertheless, the advantages offered by fiber-optic laser surgery render it a worthy and perhaps equal alternative for treating this kind of pathology.
Keywords
Introduction
Lasers have been used in otolaryngology for over 40 years, when carbon dioxide (CO2) laser was introduced into the Ear Nose and Throat (ENT) world. 1 The most commonly used ones, other than CO2, are argon and yttrium aluminum garnet lasers. 2 -5 Excision and tissue vaporization are their main utilities and many types of laser have been developed since. 1 Advantages such as excellent hemostasis, precision, minimal tissue edema and scar, and reduction in surgical time and in postoperative pain 2 have made them an extremely popular instrument in laryngeal surgery for both benign and oncological work.
Diode Laser in the Larynx
Semiconductor diode laser is a relatively new technology introduced in otolaryngology in the mid-90s and has since been utilized variously, but not widely (Figure 1). 2 It is a new topic of interest in otolaryngology alluring a growing number of surgeons due to the significant benefits it offers compared to other types of laser.

Diode laser fiber in use for laser cordectomy in T1a glottic cancer.
Diode laser is a portable versatile surgical laser (Figure 2) with a flexible quartz fiber-optic cable that passes through and also flexible and hollow straight or angled guidance instrument used as a probe. The whole system is held by the surgeon through an appropriate laryngeal handpiece (Figure 3) thanks to its lightweightness and provides varied results. 3,4
Diode laser 980 nm, a portable and easy-to-use surgeon-friendly apparatus.

An appropriate laryngeal handpiece is necessary for laser fiber laryngeal surgery. Alternatively, a laryngeal suction can be used.
Its mode of operation can be set to continuous or pulsed according to the treatment plan and the type of tissue or the pathology being processed. 2 It is also used in direct contact to the tissue or near contact, according to the desirable outcome. Direct contact to the target provides both photocoagulation and vaporization of the tissue, depending on the intensity of its power. A near contact mode, in which the laser tips stays a few millimeters over the target, ensures better photocoagulation by a high absorption in melanin and hemoglobin, making it an exceptional hemostatic tool. 4,5
The diode laser pump source, which transfers energy into the optical gain medium of the laser in order to fire it, is an electrical current and the active laser medium is a semiconductor, such as gallium arsenide. The light emitted is in the near-infrared range (800-1100 nm) and 3 wavelengths have been used since the development of this type of laser: 810, 940, and 980 nm2. Energy output can be set between 3 and 60 W, 1 although most clinical applications require a level of power between 5 and 25 W. 6 An accepted cutting mode of soft tissues is achieved with an energy output of 5 to 10 W and the laser set in continuous contact mode, whereas good vaporization is achieved between 10 and 15 W in continuous noncontact mode. 6 Finally, sufficient hemostasis requires 5 to 10 W of power intensity in noncontact continuous mode. 6
The advantages of this system include a much smaller size than other conventional lasers, rendering it a practical alternative for individual use, lower usage cost, and portability (Figure 2), which is a priority for most surgeons, as it can easily be transported between places inside a lightweight case. 2 Its setup on site is easy and fast—it generally takes less than 5 minutes—as well as its storage. 5 They contribute energy to a more eclectic area and ensure the conduction of a less invasive surgery, thus minimizing the procedure’s risk and improving the postoperative management in terms of pain and hospitalization. 5 Due to light absorption by melanin and hemoglobin, as well as the penetration depth of the laser beam in body tissue, photocoagulation is ideal and superior compared to the CO2 laser. 1 Its most unique feature is flexibility and, by extension, the ability to be directed around corners, therefore rendering it an excellent alternative to the standard CO2 laser in patients with difficult laryngoscopy due to anatomical or other pathological reasons. 7
Disadvantages include an occasional delayed repair of large lesions and creation of charring tissue in smaller lesions compared to the use of other conventional tools, such as scalpels. 2 It has been reported that diode laser tissue cutting is not as linear as other systems, such as the CO2 laser, and thus charring of the surrounding tissues is a much more frequent phenomenon. 6
Diode laser surgery can be used in many anatomical sites of otolaryngology, including oral cavity, nasal cavity and sinuses, pharynx, larynx, and trachea. 6 Many types of pathologies, malignant or benign, may be excise by this type of laser, with long-term results similar to other laser systems. When focused on laryngeal surgery (Figure 1), it can be used for the endoscopic treatment of supraglottic, glottic, or subglottic pathologies, including suprastomal granulomas, laryngomalacia, ventricular dysphonia, vocal polyps, glottic web, papillomas, glottic carcinoma, bilateral vocal cord immobility, subglottic cysts, subglottic stenosis, and subglottic hemangioma. 1 A systematic review conducted by Arroyo et al shows the extensive use of diode laser microsurgery for the previously mentioned pathologies since 2013. The wavelength may range between 810 and 980 nm, according to the type of the target lesion, and the energy output may vary from 3 to 60 W. Complications from its use include granulation, synechia and web formation, hemorrhage, laryngeal stenosis, as well as swelling, and development of emphysema or a tracheo-esophangeal fistula. 1
The objective of this article is to examine the efficacy of diode laser cordectomy for laryngeal cancer, especially for an early glottic carcinoma (Tis, T1, or T2). An 810-nm diode laser is used since 2008 with results comparable to those provided by CO2 laser, but offers an improved access to previously difficult-to-reach regions, like the anterior commissure. 1 A 980-nm diode laser is a new technology that has recently been introduced in daily clinical practice and is used for the treatment of early glottic tumors and benign pathology, such as vocal fold polyps, mostly since 2013. 1
The treatment plan for an early Tis, T1, or T2 glottic tumor is either surgical by endoscopic laryngeal conservation surgery or radiotherapy. Since the early 1980s, endoscopic transoral laser cordectomy consists the choice of surgical treatment compared to open partial laryngectomy, because it allows the precise excision of the lesion with minimal sacrifice of the surrounding healthy tissue, the avoidance of tracheotomy, and the preservation of an acceptable postoperative voice quality and swallowing. Radiotherapy ensures a better posttreatment voice quality than cordectomy, but may cause other complications, either short term, such as cellulitis and mucositis of healthy tissues, or long-term, such as xerostomia, thus rendering endoscopic surgery a more popular choice, when appropriately informed, for most patients. 8 It should be noted that surgery and radiotherapy hold similar results in terms of recurrence of the disease and overall survival. 9
Ferri and Armato attempted to demonstrate the safety of diode laser surgery in the treatment of an early glottic carcinoma (Table 1). Their study involved 45 patients with Tis and T1 glottic carcinoma, treated with endoscopic microsurgery by a diode laser between January 1999 and July 2005. Their mean age was 51 years and had negative lymph node extension of the disease. The type of vocal fold resection was performed according to the European Laryngological Society Classification and most patients underwent a type II cordectomy. A 60-W, 810-nm diode laser was utilized in continuous contact mode and power ranging from 5 to 60 W. Postoperative period was short, varying from 2 to 5 days of hospitalization, and mostly uncomplicated before discharge. Results showed an exceptional survival rate for the majority, as only 5 recurrences—4 regional and 1 distant—took place in T1b patients and required a more extensive intervention. 8
List of Publications Related to Dode Laser Cordectomy for Glottic Cancer.
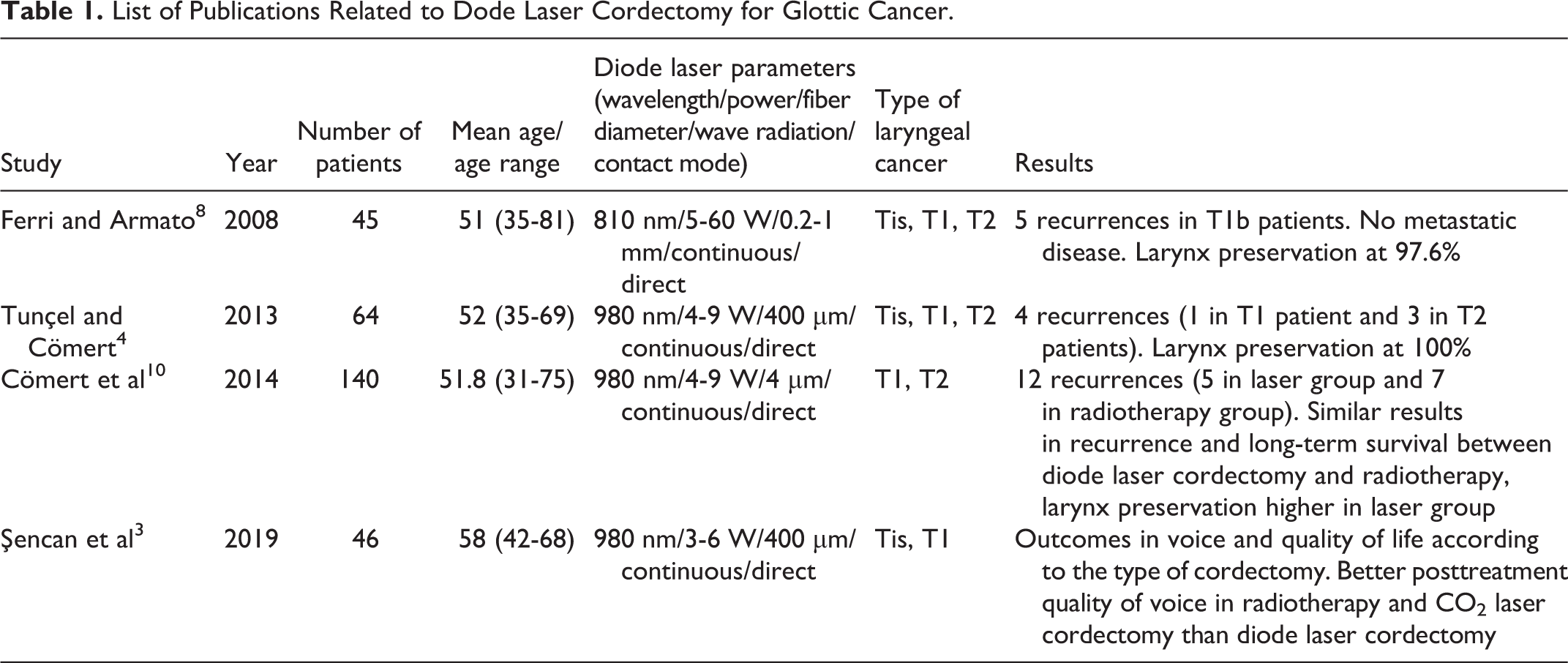
In a recent paper published in 2013, Tunçel and Cömert studied the result of diode laser microsurgery in 64 patients with previously untreated TisN0, T1N0, or T2N0 glottic carcinoma and a mean age of 52 years. A 980-nm flexible diode laser was used with power ranging from 4 to 9 W in direct contact to the target tissue. The cutting region was delimited by performing small shots around the lesion, which was later resected en block. The type of cordectomy was defined according to the staging of the carcinoma; therefore, type I was performed by resecting the mucosa of the vocal fold in Tis. Type II to III resections were used for T1 lesions of the vocal folds and type IV and V were chosen for T2 lesions. Immediate postoperative course for the majority of the studying group was uncomplicated and minor hemorrhage occurred in an extremely low percentage who underwent a major laser cordectomy for a T2 lesion, which was treated on the spot. Long-term complications such as web development in the anterior commissure, vocal fold edema, and granuloma formation were present in some cases. Results showed a minor recurrence rate of 6.2%, who afterward received an additional treatment, and preservation of the larynx was secured in all cases. 4 Although diode laser surgery holds many advantages over CO2 laser, this study reveals similar oncologic results between these 2 systems. Diode laser is a much cheaper and easy-to-use tool in terms of versatility and portability and provides the advantage of a better access to distant or angled areas not easily reached and manipulated with the direct straight beam of the CO2. 4
As mentioned above, the treatment for an early glottic carcinoma may be surgery or radiotherapy, according to the patients’ desire, after an informed discussion and consent. Cömert et al attempted to compare early oncologic results of diode laser cordectomy versus radiotherapy for the treatment of an early glottic tumor in a study performed in Ankara in 2014. One hundred forty patients with T1 and T2 glottic carcinomas were treated between January 2008 and August 2012. Patients underwent diode laser cordectomy or radiotherapy according to certain factors such as patient’s choice, disease interval, and microscopic evaluation of the larynx under general anesthesia. Patients were strongly recommended to undergo a cordectomy after the acquisition of the diode system in 2010, but were also informed about the advantage of radiotherapy in terms of voice quality outcome. Therefore, 72 patients decided to have their tumor removed surgically and 68 patients received radiotherapy. Results showed that a 6.9% of the patients in the laser group developed a locoregional recurrence, in contrast to a 10.2% in the radiotherapy group. Long-term survival rates were high in both groups, with a nonsignificant difference between them. A major difference between these 2 methods, except the advantages of diode laser cordectomy mentioned above, is the plethora of treatment options patients are left with in case of a recurrence, including possible revision cordectomy, radiotherapy, as well as open surgery. Although no significant difference was discovered in terms of long-term survival rates and recurrence of the disease, preservation of the larynx was achieved in a higher percentage in patients who underwent transoral diode laser cordectomy than those who received radiotherapy. 10
A study conducted by Şencan et al between 2012 and 2015 on 46 patients with squamous cell Tis (in situ) and T1a glottic carcinomas reveals the quality of voice outcomes postsurgically and their effect in the quality of life. Using commonly accepted questionnaires, such as the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire–Core Questionnaire module (EORTC-QLQ-C30), the Head and Neck cancer-specific questionnaire (EORTC-QLQ-H&N-35), and the Voice Handicap Index (VHI), the team was able to analyze the aforementioned effect. Patients were asked to complete these questionnaires before surgery and 6 months after, in order to analyze any difference between them. A 980-nm diode laser with a 400-mm fiber was used with power fluctuating from 3 to 6 W in continuous mode in order to remove en block the lesions. Voice Handicap Index results showed that postoperative quality of voice decreased by the extent of resection. Types I and II cordectomies had insignificant effect on the patient’s voice and types III and IV caused moderate lingual disability. The VHI postoperative score was higher than the corresponding one following CO2 laser cordectomy or radiotherapy, showing that the quality of voice was slightly worse after diode laser cordectomy than these other therapies. Nevertheless, preoperative VHI score was higher than the postoperative score, indicating that the personalized quality of voice was better after diode laser cordectomy. The QLQ questionnaires revealed a high impact in speech and social contact after a type V cordectomy. Also, significant differences in pain, swallowing problems, senses, and social eating were greater in type IV cordectomy group. Suffice it to say that, similarly to CO2 outcomes in voice and quality of life in general, the impact of diode laser cordectomy in these features is highly correlated with the size of the resected tissue. 3
Laser cordectomy is a gold-standard surgical option for treatment of early glottic carcinomas and diode laser in particular is increasingly being used as an alternative to the predominant CO2 laser. Therefore, voice and quality-of-life outcome is a topic requiring discussion, when a choice is made to administer this kind of treatment. There is a learning curve and the increasing need of perfecting the outcome of these phoniatric surgeries has led to the development of high standard devices and the improvement of surgeons’ skills.
Conclusion
Diode laser is a relatively new technology with many applications in otolaryngology. It offers many advantages compared to other systems, such as portability, lower cost of installation, and the ability to manipulate tissues that were previously difficult to reach with the usage of straight-aiming lasers, such as CO2 laser. It is a tool that has been recently introduced, but not widely used, for the excision of early glottic carcinomas. Although results so far in terms of postoperative oncologic result and voice quality show no significant improvement over other conventional methods, their general qualities render it a great alternative and perhaps an equal alternative for endolaryngeal microsurgery with a lot of potential. Surgeon’s increasing interest lies in its ability to reach spots in an angle due to its flexible fiber and administer a laser beam under these circumstances. There is a learning curve when using flexible fibers in general under anesthesia instead of a straight beam, as with any surgery, but is a quick one. Future innovations of this pioneering system may be the catalyst for further improving its treatment results, thus broadening its use by an increasing number of laryngeal surgeons.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.