
Abstract
Objective:
To investigate voice quality changes of patients treated by transoral laser cordectomy (TLC) for early glottic cancer according to the type of cordectomies.
Methods:
A total of 164 consecutive male patients with an early glottic cancer were prospectively recruited from the Department of Otolaryngology—Head and Neck Surgery of the Georges Pompidou European Hospital. Depending on the tumor characteristics, patients benefited from type I to VI CO2 cordectomy regarding the European Laryngological Society classification. The following voice quality outcomes were pre- to postoperatively assessed: voice handicap index (VHI), perceptual grade of dysphonia, roughness, breathiness, maximum phonation time, and acoustic parameters.
Results:
Fifty-five patients with Tis, T1, or T2 vocal fold cancer completed the study (mean age: 61.7 years). Of these patients, 34 and 21 composed group 1 (types I-III TLC) and group 2 (types IV-VI TLC), respectively. Voice handicap index, grade of dysphonia, and breathiness significantly improved from pre- to 3- and 6-month posttreatment in group 1. In group 2, only VHI significantly improved from pre- to 3- and 6-month posttreatment. Acoustic and aerodynamic measurements did not change throughout the postoperative course. Patients with types I to III TLC exhibited better postoperative voice outcomes compared to those treated by types IV to VI TLC.
Conclusion:
Irrespective to the types of TLC, the subjective voice quality of patients treated by CO2 laser cordectomy for early glottic cancer significantly improved from pre- to 3- and 6-month posttreatment. The usefulness of aerodynamic and acoustic measurements as postoperative outcomes of voice quality changes remain controversial and require future studies considering multidimensional assessment of voice.
Introduction
The first report of transoral laser cordectomy (TLC) for early stage glottic carcinoma was published by Strong 1 in 1975. Since then, the technique evolved and it is currently worldwide used. 2 -4 Transoral laser cordectomy exhibited lower morbidity, similar survival, and better patient postoperative functional outcomes than conventional surgical approaches. Nowadays, radiation and TLC are considered as the standard therapeutic approaches for early glottic cancer. 5,6 Clinical studies reported that radiation is associated with similar survival outcomes compared with surgery, but the superiority of radiation over TLC about the voice quality assessment is still controversial. 7,8
To date, a few studies investigated voice quality evolution from pre- to post-TLC therapy. 9 -14 Overall, there was an important heterogeneity between studies about the pre- to posttreatment evolution of voice quality functional outcomes; the voice quality measurements reaching stability 6 months after TLC. Moreover, the majority of studies were characterized by a limited number of patients, and the use of nonexhaustive voice quality measurements. The consideration of the types of cordectomies was also lacking in the majority of clinical studies. 9 -14 However, the type of cordectomies may have an important impact on voice quality outcomes. In our practice, we observed that limited TLC (type I-III cordectomies) report better functional outcomes than extended TLC (type III-VI). The aim of this study was to investigate voice quality changes of patients treated by TLC for early glottic cancer according to the type of cordectomies.
Materials and Methods
Patients and Setting
A total of 164 consecutive patients with an early glottic cancer were prospectively recruited from the Department of Otolaryngology—Head and Neck Surgery of the Georges Pompidou European Hospital, Paris, France. The following inclusion criteria were considered: male sex (to rule out gender-related voice differences), histologically confirmed early stage tumor, 15 and availability to undergo voice quality assessment postoperatively for the 12-month postoperative period. Patients with previous history of voice disorders or radiation therapy were carefully excluded. The local ethics committee approved the study protocol and the informed consent was obtained for all patients.
Transoral Laser Cordectomy
After adequate laryngeal exposition, the laryngologist carefully reassessed the vocal fold lesion with a rigid 0° or 30° endoscope. A Sharplan CO2 laser with an AcuSpot micromanipulator (Alternup Medical factory, Tel Aviv, Israel) was used in continuous mode (1-5 W, 270 µm spot sizes, Sharplan Laser, Tel Aviv, Israel) for all patients. Lesions were completely removed (“en bloc” resection) on the basis of the computed tomography-scan features and peroperative visual character of the lesion. The type of cordectomy used depended on the size, the location, and the stage of the lesion. Transoral laser cordectomy was classified according to the European Laryngological Society Classification 16,17 as subepithelial (type I), subligamental (type II), transmuscular (type III), total (type IV), extended (type Va), and anterior (type VI), encompassing the anterior commissure and anterior part of both vocal folds. None of the patients required tracheotomy. Oral intake was started 24-hour after the surgery. Patients were discharged after 24- or 48-hour hospitalization. A voice rest of 10 days was advised for all patients. Patients received proton pump inhibitors for a 3-month duration to control the impact of laryngopharyngeal reflux on the vocal fold healing. 18
Note that 4 patients underwent a “second look” procedure, which revealed in situ carcinoma (n = 1) and granulation tissue (n = 3). For these patients, the time of voice quality evaluation was adjusted in relation to their last surgery.
Multidimensional Voice Quality Analysis
Patients benefited from videolaryngostroboscopy, subjective and objective voice quality assessments at baseline (preoperative time), 3-, 6- and 12-month post-TLC. The validated French version of the Voice Handicap Index (VHI) was used as patient-reported outcome questionnaire of voice quality. 19 Perceptual voice quality evaluation was based on the blinded rating of Grade, Roughness, and Breathiness (GRB) evaluation system by 2 experienced laryngologists. 20 Laryngologists were blinded regarding the type of cordectomy. The perceptual voice quality assessment was based on connected speech and reading text.
The objective voice quality evaluations included aerodynamic (maximum phonation time [MPT]) and acoustic analyses. Patients were recorded during sustained/a/phonation (3 trials) at comfortable intensity and pitch level with a high-quality microphone (AKG 550) placed 4 cm of the mouth. The MPT value consisted of the best duration of 3 trials. Acoustic analysis was conducted through the Multi-Dimensional Voice Program (Kay Elemetrics, Lincoln Park, New Jersey). The following parameters were measured: fundamental frequency (F0), jitter, shimmer, and noise-to-harmonic ratio (NHR). Voice quality outcome changes were evaluated from pre- to postoperative time according to the type of cordectomy (type I-III or IV-VI).
Statistical Analysis
Statistical analysis was performed with Statview software (version 5.0, SAS Institute, Inc). Wilcoxon rank test was used to analyze changes in VHI, GRB, MPT, and acoustic parameters through the 3 to 12-month postoperative course. Mann-Whitney U and Friedman tests were used for comparisons between subgroups of patients. A value of P < .05 was considered as statistically significant.
Results
Of the 164 patients, 55 completed the study (mean age: 61.7 years, range: 28-85 years). Tumors were classified as Tis in 20 (36.4%) patients, cT1a in 27 (49.1%) patients, cT1b in 3 (5.4%) patients, and cT2 in 5 (9.1%) patients. The following cordectomies were performed: type I (n = 17); type II (n = 10); type III (n = 7); type IV (n = 3); type Va (n = 13), and type VI (n = 5). Thirty-four and 21 patients composed group 1 (types I-III) and group 2 (types IV-VI), respectively (Table 1). Both groups were comparable. There were no other recurrences and no additional treatment (radiation) during the following period. The multidimensional voice quality data from pre- to post-TLC are available in Table 2. The pre- to posttreatment treatment voice quality outcome changes (statistical analyses) of groups 1 (types I-III) and 2 (types IV-VI) are described in Tables 3 and 4, respectively.
Group Characteristics.
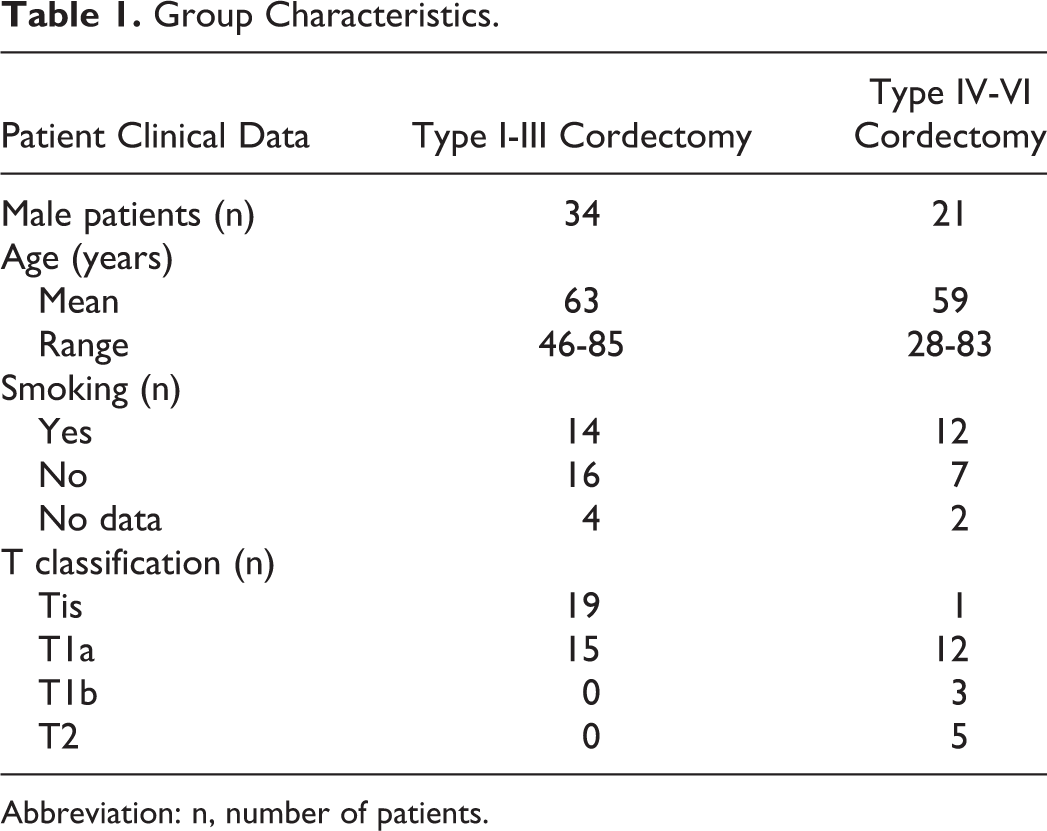
Abbreviation: n, number of patients.
Pre- to Posttreatment Multidimensional Voice Quality Evolution.
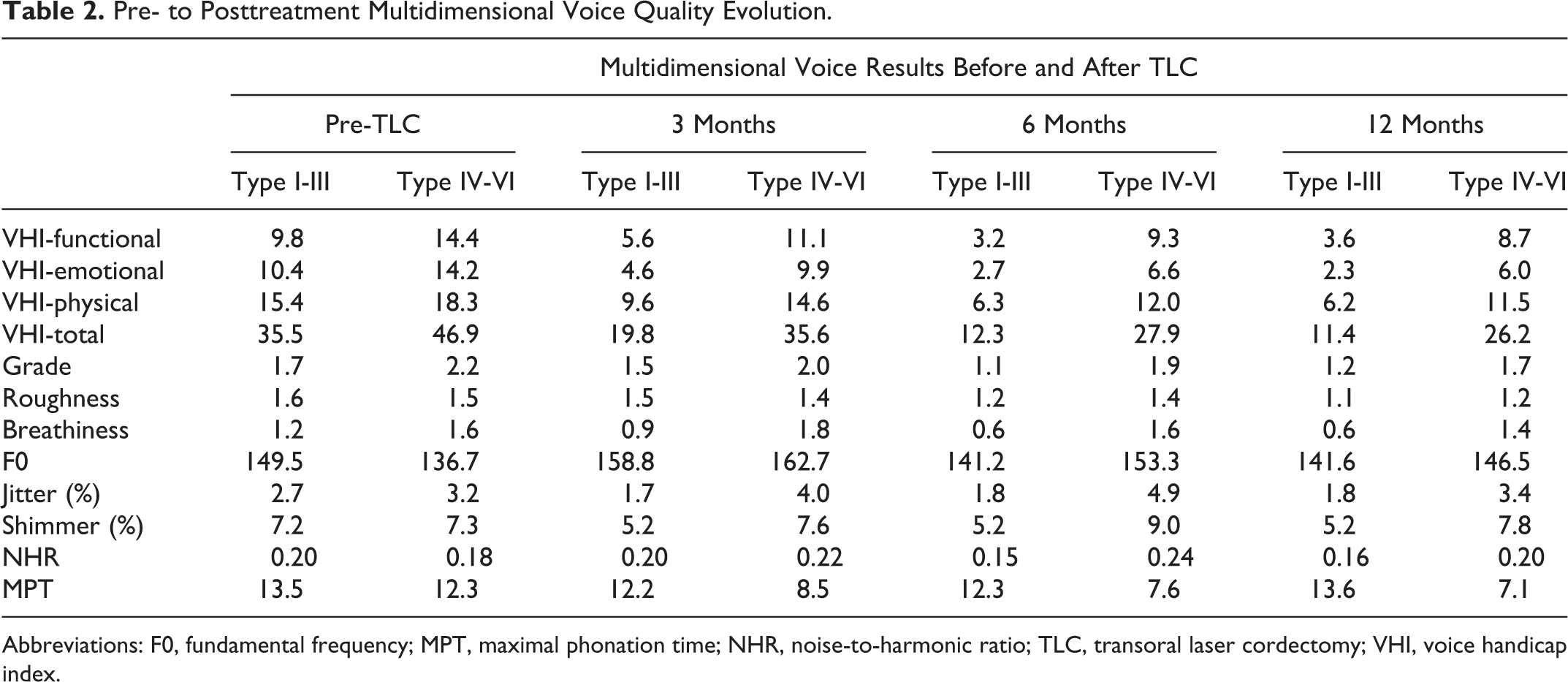
Abbreviations: F0, fundamental frequency; MPT, maximal phonation time; NHR, noise-to-harmonic ratio; TLC, transoral laser cordectomy; VHI, voice handicap index.
Longitudinal Comparison of Voice Outcome in Patients After Cordectomy Type I to III.
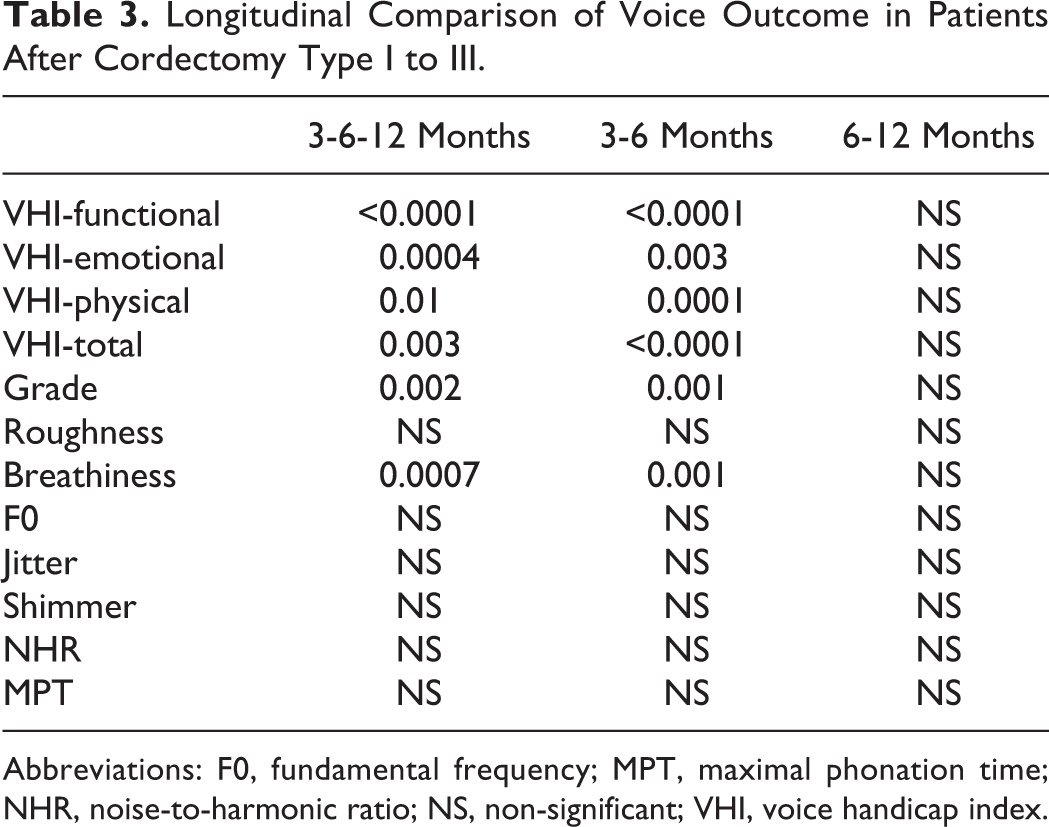
Abbreviations: F0, fundamental frequency; MPT, maximal phonation time; NHR, noise-to-harmonic ratio; NS, non-significant; VHI, voice handicap index.
Longitudinal Comparison of Voice Outcome of Patients After Cordectomy Type IV to VI.
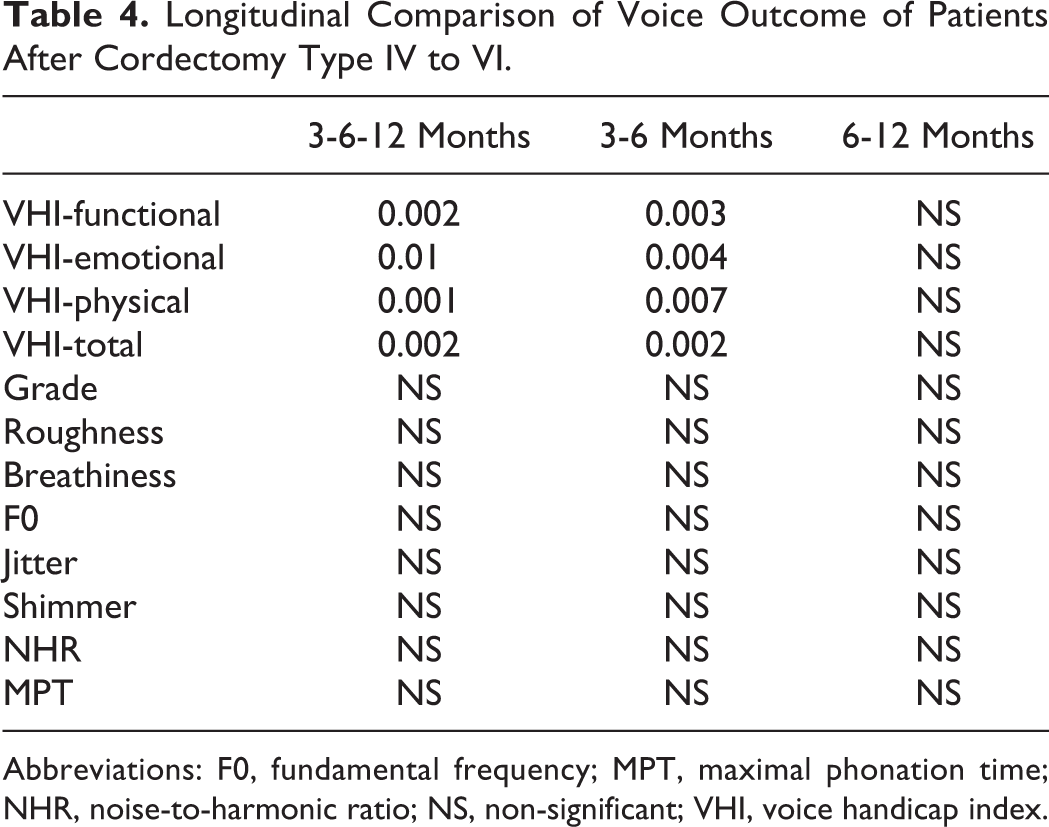
Abbreviations: F0, fundamental frequency; MPT, maximal phonation time; NHR, noise-to-harmonic ratio; NS, non-significant; VHI, voice handicap index.
Overall, VHI, grade of dysphonia and breathiness significantly improved from pre- to 6-month posttreatment in patients who benefited from types I to III TLC (Table 3). Only VHI sub- and total scores significantly improved from pre- to 6-month posttreatment in patients who benefited from types IV to VI TLC (Table 4). Objective voice quality measurements did not improve throughout postoperative period in both groups.
The group comparison revealed that group 1 (types I-III TLC) had better 6-month values of VHI, grade of dysphonia, breathiness, MPT, jitter, shimmer, and NHR compared to group 2 (types IV-VI; Table 5). Similar findings were found for 12-month group comparison at the exception of the grade of dysphonia (P = .05) and the NHR mean values (P = .06).
Comparison of Voice Outcome in Patients With Cordectomy Type I-III or IV-VI.
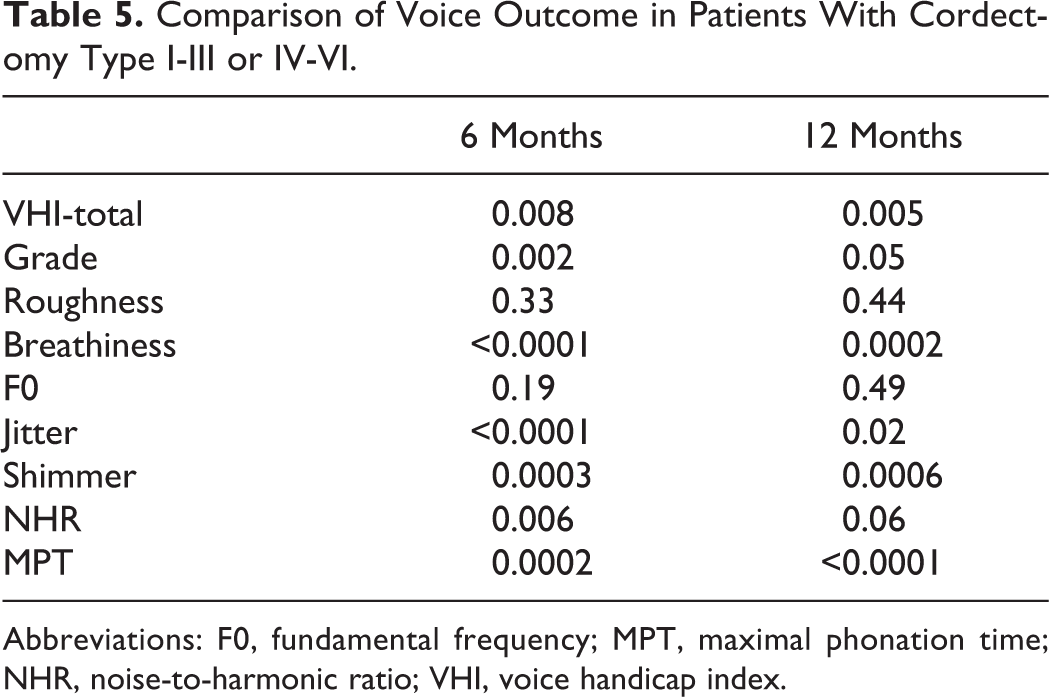
Abbreviations: F0, fundamental frequency; MPT, maximal phonation time; NHR, noise-to-harmonic ratio; VHI, voice handicap index.
Discussion
The dysphonia related to malignant disease is known to significantly impact emotional, physical, functional, and economic aspects of the patient life. The VHI was initially developed for evaluating both patient subjective feeling and disability from their voice disorder. 19 Nowadays, VHI is considered as one the best patient-reported outcome questionnaire for the assessment of voice function. 21 -24
The main finding of this study is the usefulness of VHI as postoperative outcome for patients who benefited from cordectomy, irrespective of the type of cordectomies. In other words, patients have considered that the tumor resection through TLC significantly improved their voice; supporting the occurrence of substantial subjective voice quality impairments before TLC. Our results are supported by the longitudinal study of Chu et al 10 who found significant improvements of VHI in a cohort of 25 patients treated by CO2 cordectomies. Similarly, Keilmann et al, 13 reported a trend of postoperative improvement of VHI scores in 16 patients who benefited from different types of cordectomies. However, because the VHI is based on (subjective) self-evaluation, the postoperative score may be influenced by the individual patient’s amount of voice use, level of vocal effort, and, particularly, the satisfaction of being successfully treated for a malignant disease.
Moreover, we observed a significant improvement of perceptual dysphonia and breathiness from pre- to 6-month posttreatment in patients treated by types I to III cordectomies. In the same vein, Chu et al and Galletti et al reported significant improvements of perceptual voice quality evaluations throughout the postoperative period. 10,25 The blinded rating used in this study is a strength for avoiding subjectivity of the rater about the knowledge of the time of the voice recording. The lack of blinded assessment in the previous studies limits us in the literature comparison. Because perceptual voice quality assessments are still subjective and depend on the method, the use of both aerodynamic and acoustic measurements makes particularly sense for exhibiting subtle abnormalities in the vibration process of the vocal folds. Thus, our data did not report significant pre- to post-TLC improvements of aerodynamic and acoustic measurements, corroborating findings of some studies. 10,12 However, other authors reported significant improvements, 9,13 or worsening 11 of objective voice quality evaluations. The inconsistencies between studies are related to the heterogeneity regarding the patient inclusion criteria (sex, age, history, cofactors), and the methods used for the measurement of acoustic parameters. Thus, previous reports demonstrated that depending on the time interval over which the acoustic parameters are measured, the clinically demonstrated effect of a treatment/posttreatment course may or may not be statistically demonstrated. 26,27 These data and the discrepancies between our results and those of the literature strengthen the need of standardization of acoustic measurement methods. This point is important for future studies that aim to compare the impact of treatment on voice quality evolution of patients with early glottic cancer. Indeed, the type of treatment may substantially change the biomechanical properties of vocal folds, by the removal of some critical vocal fold layers, such as the Reinke space. Thus, the excision of tumor, margins (eg, a part of the vibrating mucosa), associated with the resection of the vocal ligament or muscle, leads to a fibrosis process and scar formation, which definitively strongly modifies the normal physiologic function of the vocal fold. 14,28,29 Both aerodynamic and acoustic measurements may be useful for understanding the microfunctioning of the vocal folds. Precisely, the use of subjective and objective voice quality assessments could help the speech pathologist to following patients throughout the voice rehabilitation. In that way, the differences in voice quality outcomes between patients with types I to III cordectomy and those with types IV to VI cordectomy suggest the development/use of different programs of voice rehabilitation considering different approaches of both intensity and frequency of speech therapy sessions.
The main strength of this study is the use of the multidimensional European Laryngological Society protocol, which considers patient-reported outcome questionnaire, perceptual, aerodynamic, and acoustic assessments for the voice quality evaluation. 30 To our knowledge, only a few studies assessed voice quality of patients treated with TLC with patient-reported outcome questionnaire, perceptual analysis, aerodynamics, and acoustic measurements. 10,13 Because the subjective and objective voice quality evaluations do not assess similar aspects of voice, it is still important to consider multidimensional assessment for the evaluation of voice quality.
This study has many weaknesses that have to be addressed in future trials. First, we did not record the videolaryngostroboscopical findings, which would provide additional information about the voice quality recovery/changes after treatment. Second, we only considered males in the inclusion of patients, which was related to the fact that sex of patients substantially impacts the assessment and reliability of acoustic measurements. This weakness is balanced by the fact that, in practice, the high majority of patients with head and neck cancer are male. Furthermore, in the future, it would be interesting to conduct similar study for female patients in order to investigate potential gender-related differences, which would be due to vocal fold anatomical and histological differences, 31 as well as gender-related differences in the postoperative inflammatory process. 32
Conclusion
The subjective voice quality of patients who benefited from CO2 laser cordectomy for early glottic cancer significantly improved from pre- to 6-month posttreatment. The improvement was better in types I to III cordectomy patients compared with those who benefited from types IV to VI cordectomy. The VHI is the most indicative tool of voice changes. Future studies are needed to investigate the usefulness of subjective and objective voice quality evaluations in the postoperative course of patients operated for early glottic cancer.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.