
Abstract
Tracheal metastasis from papillary thyroid carcinoma (PTC) is an unprecedented and rare entity. We present the case of a 65 year-old lady who suffered from dyspnea and a thyroid goiter that turned out to be PTC. A magnetic resonance imaging (MRI) scan of the lungs revealed a huge tracheal mass causing obstruction of the tracheal lumen. She underwent a surgical tracheostomy and diode laser debulking of the tumor. Following this, she had a total thyroidectomy and postoperative radioiodine ablation and radiotherapy. She remains well under close and regular follow-up. A secondary tracheal tumor usually comes from a lymphatic spread of the primary tumor, whereas the vascular route is rarely reported. Endoscopic minimally invasive laser tracheal surgery with adjuvant radiotherapy appears to be equally effective to more aggressive tracheal resections.
Introduction
Papillary thyroid carcinoma (PTC) has an indolent nature and usually metastasizes through the lymphatic system to distant locations such as lungs, bones, and brain. 1 Endoluminal tracheal metastasis from PTC is extremely rare with very few reports in the literature, as it usually invades the trachea by infiltration. 1 Its presentation may vary from asymptomatic to dyspnea and bleeding of the mass resulting in hemoptysis. 2 Surgery either in the form of aggressive resection or endoscopic removal followed by radiotherapy and radioactive iodine are some of the options to address this unusual and difficult-to-treat pathology.
Case Report
A 65-year-old lady presented to the endocrine surgeons with a thyroid goiter and a 6-week history of increasing dyspnea. Magnetic resonance imaging (MRI) of her neck showed the thyroid goiter and a tracheal mass obstructing more than 90% of the tracheal lumen (Figure 1). Two attempts to obtain diagnosis with a flexible bronchoscopy from the chest physicians were nondiagnostic. She was referred to the otolaryngology team for diagnosis and management of the tracheal tumor. She underwent a scheduled semi-emergency tracheostomy under local anesthesia. Following this, a 980 nm diode laser flexible fiber was used via a laryngeal handpiece and a 40-cm Rigid 0° endoscope to remove the tracheal lesion (Figure 2) under general anesthesia. The entire lesion was almost completely removed (Figure 3) and multiple biopsies were sent. Histopathology showed carcinoma with a papillary configuration, consisting of finely or more thickly connected vascular shafts, coated by a layer of oval cells with clear or pale-colored cytoplasm, with overlapping enlarged nuclei. Papillary and glandular forms showed partial, mild to moderate positivity in thyroglobulin (Figures 4 and 5). She had an uneventful recovery and was discharged the following day. She subsequently underwent a total thyroidectomy and central neck dissection. Histopathology confirmed the previous findings of PTC with a tracheal metastasis. Her rare case was discussed at a Multidisciplinary team meeting. The decision was made to undergo postoperative radioiodine treatment followed by radiotherapy. She remains well 9 months from diagnosis and under regular follow-up.

Magnetic resonance imaging of the neck (sagittal view) showing the tracheal tumor almost completely obstructing the airway (large arrow) and the thyroid mass pushing against the trachea (2 arrows).
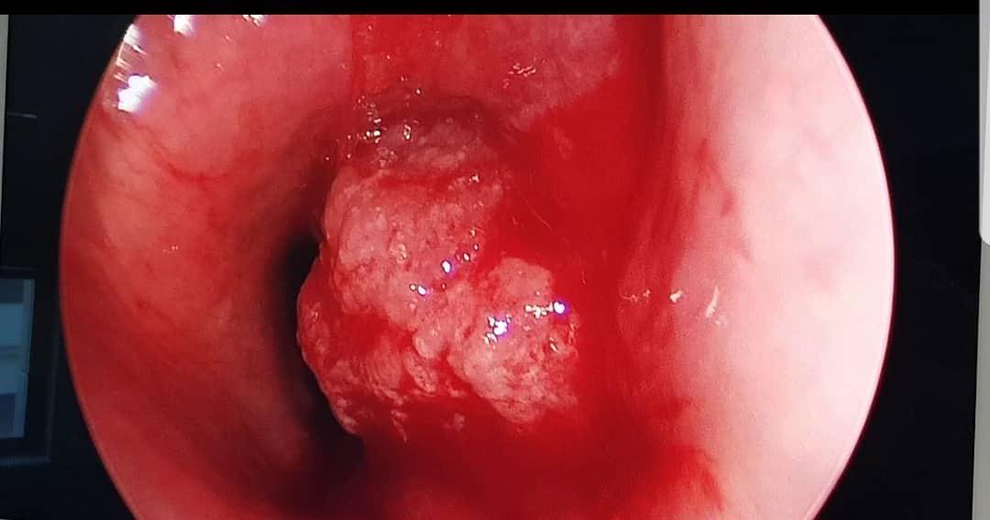
Endoscopic view of the tracheal metastatic tumor with an almost complete endoluminal obstruction.

End of diode laser debulking procedure with adrenaline-soaked neuropatty in place.
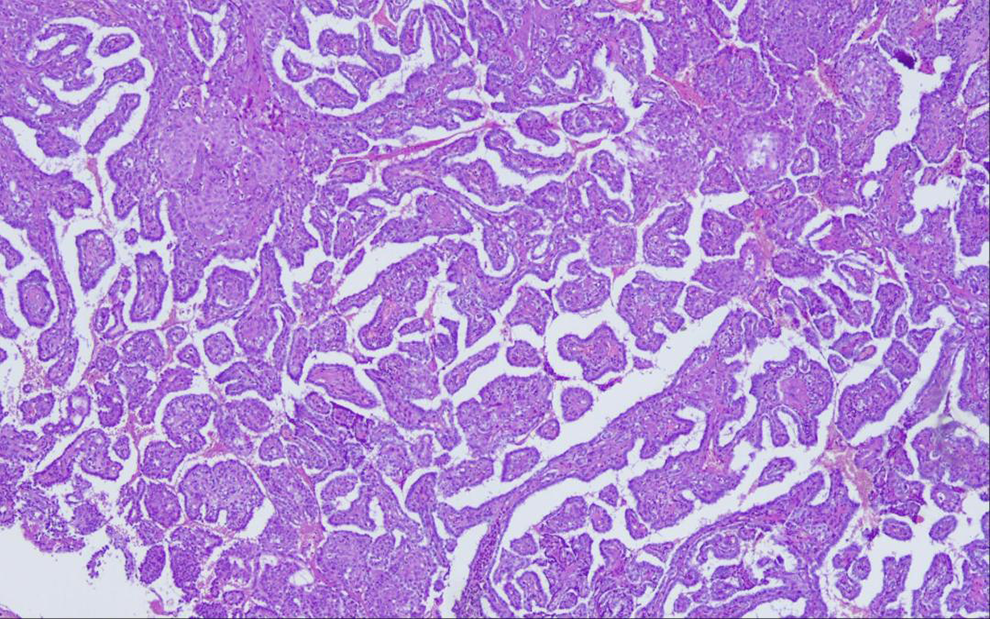
(H&E stain, ×20) Carcinoma with a papillary configuration, consisting of finely or more thickly connected vascular shafts, coated by a layer of oval cells with clear or pale-colored cytoplasm, with overlapping enlarged nuclei.
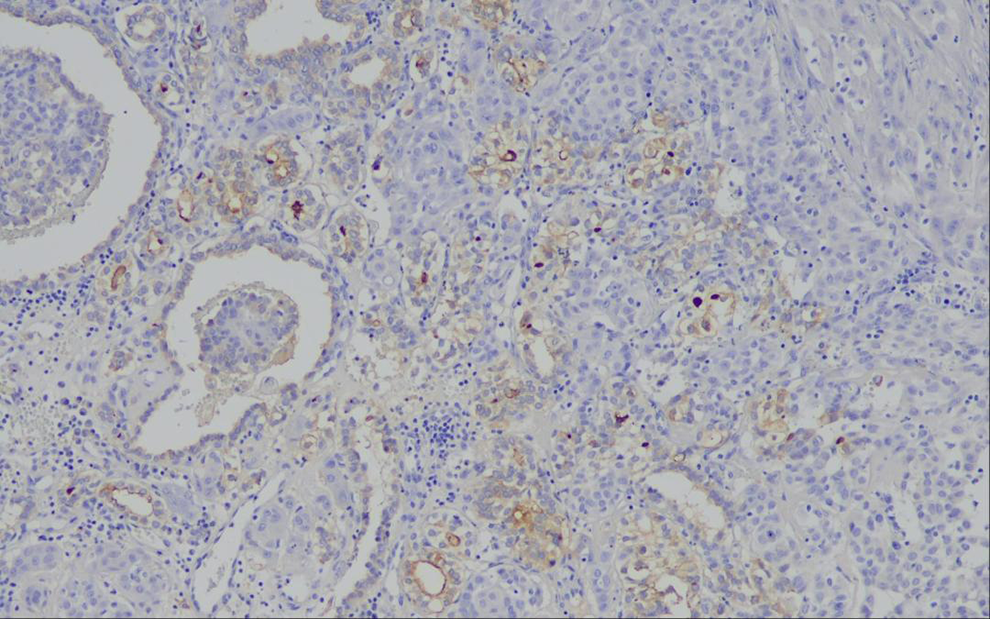
Papillary and glandular forms showed partial, mild to moderate positivity in thyroglobulin (×20)
Discussion
A secondary tracheal tumor is more common in the literature and in clinical practice than a primary one and may originate from local or distant sites, either with direct infiltration from a nearby organ, such as the thyroid gland, or with a metastatic pattern through the lymphatic and the circulatory system. 3 Kiryu et al stated that primary sites of tracheal masses may include a variety of organs, more often breasts, colon, and kidneys. In their research, they created a useful classification system of the histological development of such tumors. 4
Thyroid cancer, in general, invades the trachea in 1% to 8% of all cases 5 and PTC usually infiltrates the trachea directly. 6 Metastatic nature of PTCs normally takes advantage of the lymphatic system and spreads to lymph nodes, whereas vascular invasion is uncommon and involves the brain, the lungs, bones, and other soft tissues. 6 Thus, a tracheal mass derived from a PTC is an extremely rare entity.
Such a tumor manifests with a variety of symptoms that range from an asymptomatic tracheal involvement to a massive airway obstruction and intraluminal bleeding which causes hemoptysis. 2 Its presence is a poor prognostic indicator remarkably decreasing long-term survival. The mass is diagnosed by a combination of radiological and endoscopic means, for example, ultrasonography, MRI, and flexible bronchoscopy.2
Surgical management of these patients, such as shaving of the tumor from the outside of the trachea, window, or tracheal resection and total laryngectomy, is still controversial as conservative treatment with radioiodine and external beam radiation renders significant results. 2,7 Mossetti et al performed radical resections of tracheal masses with minor complications in 8 patients. 8 Kim et al question the effectiveness of surgical resection of the tracheal mass in a big study involving 1919 patients with thyroid cancer, 65 of which (3.39%) had a tracheal involvement. 9 A paper published by Shenoy et al designates the need for a more conservative approach in accordance to the extent of the resection and limit it to shaving of the mass followed by radioiodine treatment and external beam radiation in order to eliminate the residual microscopic traces of the disease. 10
Conclusion
The rare case of tracheal metastasis from PTC indicates thyroid carcinoma’s big diversity. A multidisciplinary approach is a necessity for the management of these patients as its treatment carries a huge perplexity and a clear-cut decision is not often easy to make. New studies supporting endoscopic minimally invasive techniques rather than big tracheal resections with adjuvant therapy provide enough data for a better overall prognosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.