
Abstract

An 86-year old female with a recently diagnosed upper respiratory tract infection presented to the otolaryngology clinic with a persistent dry cough, odynophagia, dysphonia, and progressive dyspnea refractory to outpatient treatment with systemic corticosteroids. The relevant history included her being an active smoker with a remote history of papillary thyroid cancer treated with total thyroidectomy and radioactive iodine. On physical examination, she exhibited inspiratory stridor with mild respiratory distress. Flexible fiber-optic laryngoscopy (FFL) revealed a submucosal prominence of the posterior pharyngeal wall abutting the epiglottis causing obstruction of the laryngeal inlet (Figure 1). Other pertinent findings on FFL included mild edema of the false vocal folds and full vocal fold mobility bilaterally. The patient was transferred from clinic to the emergency department, where a computed tomography scan of the head and neck with contrast revealed osteophytes along the anterior aspect of the cervical spine from levels C3-C7, consistent with diffuse idiopathic skeletal hyperostosis (DISH; Figure 2). Given her clinical findings, including an anticipated difficult intubation, it was recommended she undergo tracheotomy to secure her airway. The patient, however, deferred surgery and elected for observation in the intensive care unit (ICU) where she was treated with dexamethasone 8 mg intravenously every 8 hours and ibuprofen 800 mg every 6 hours. Over the course of her 2-day ICU stay, she maintained an oxygen saturation between 96% and 100% on room air and experienced moderate symptomatic improvement allowing transfer to the floor. Before considering hospital discharge, the neurosurgical team discussed definitive treatment of her airway obstruction with a cervical osteophyte reduction; however, the patient deferred surgery citing her improvement with conservative measures and her increased risk for postoperative complications given her history of thyroidectomy. On hospital day 2, the patient was discharged home with prednisone 40 mg daily for 5 days and ibuprofen 800 mg every 8 hours for 14 days. At her 2-week follow-up, the patient reported a return to her baseline respiratory status. On physical examination, she exhibited no respiratory distress or stridor; however, a repeat FFL revealed only slightly improved obstruction of her laryngeal inlet (Figure 3). The need to perform a prophylactic tracheotomy was revisited; however, the patient again deferred surgical intervention. At her subsequent 2-month follow-up, she remained at her baseline respiratory status.

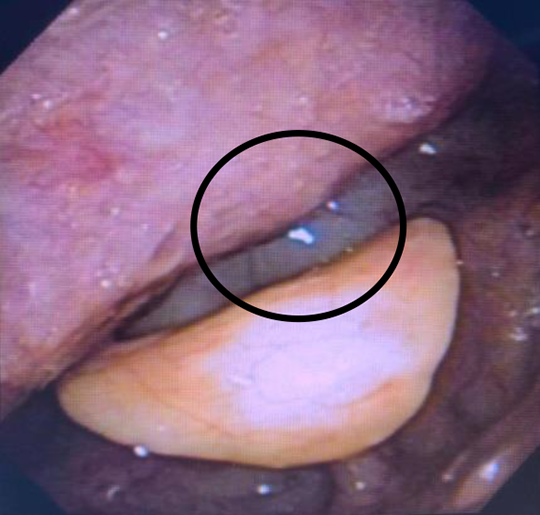
Flexible fiber-optic laryngoscopy showing submucosal prominence of the posterior pharyngeal wall abutting the epiglottis causing near-complete obstruction of the laryngeal inlet (circled).
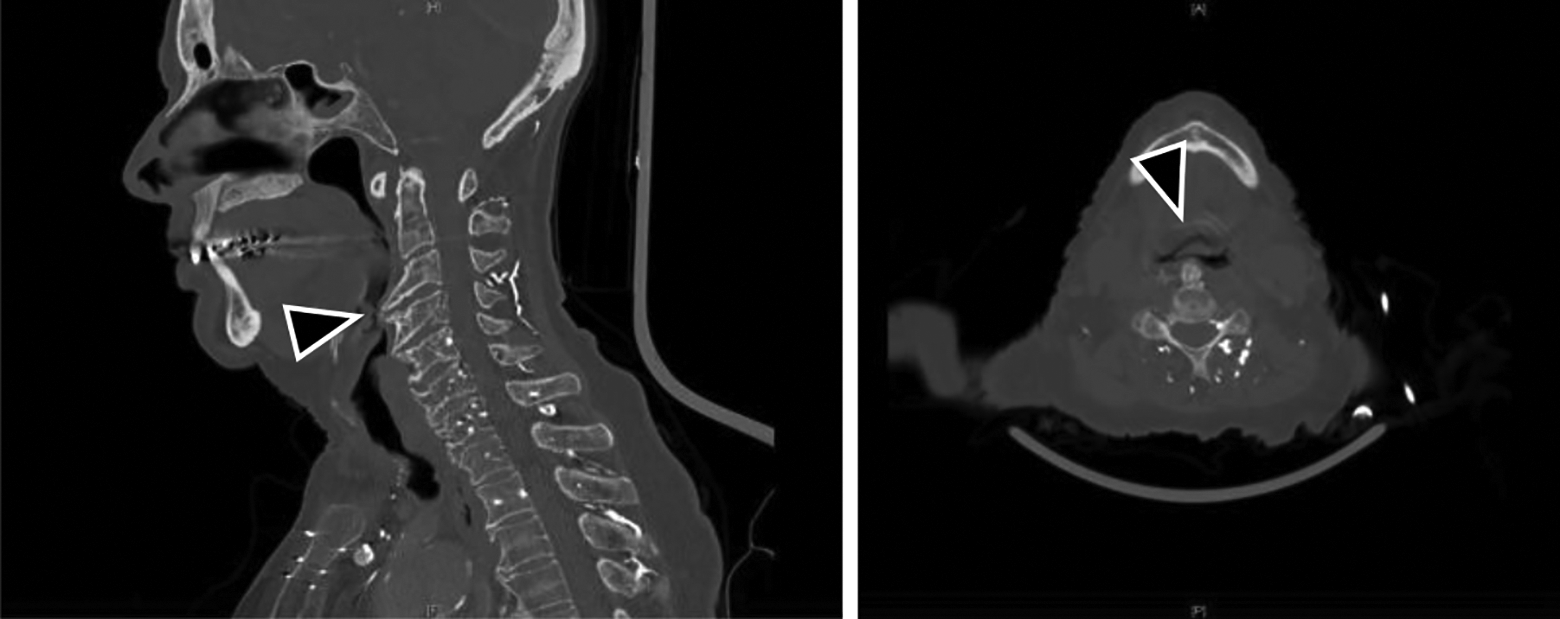
Sagittal and axial computed tomography scan of the head and neck with contrast showing protuberant osteophytes along the anterior aspect of the cervical spine from levels C3-C7 (arrowhead), consistent with diffuse idiopathic skeletal hyperostosis.
Flexible fiber-optic laryngoscopy showing resolution of laryngeal edema with continued prominence of anterior cervical osteophytes into the posterior pharyngeal wall (circled).
Diffuse idiopathic skeletal hyperostosis represents a form of degenerative osteoarthritis associated with an abnormal ossification of ligaments and soft tissue throughout the body, most notably the anterior longitudinal spinal ligament. 1 Diffuse idiopathic skeletal hyperostosis affects up to 11% of the elderly population, though many cases remain asymptomatic or go undiagnosed due its minor, chronic symptomology. 1 Symptomatic cases often occur in males, and the primarily complaint is dysphagia (75%). Concomitant airway-related complaints are less common but include dyspnea (14%), cough (3%), dysphonia (2.5%), and stridor. 2 Often times, when there are respiratory complaints associated with DISH, they are attributable to (1) osteophytes causing direct anatomic obstruction of the upper airway and/or (2) inflammation of the retropharyngeal space, anterior to the enlarged osteophytes, resulting in airway narrowing. 2 Our case demonstrates the conversion of asymptomatic DISH to symptomatic DISH by way of an overlying upper respiratory infection due to the second mechanism described in the previous sentence. To our knowledge, no such case of DISH with a superimposed upper respiratory tract causing airway obstruction has been reported in the literature.
From a practical perspective, it does not seem necessary to run diagnostic studies to identify all cases of DISH because it is often a benign asymptomatic pathology3,4; however, if DISH is incidentally discovered on diagnostic imaging, it should be understood that this patient may bet at risk for secondary sequelae such as airway compromise. This seems particularly relevant in light of the appearance of novel respiratory viruses, such as coronavirus disease 2019 (COVID-19), that cause robust inflammation of mucosal tissue. 5 Patients found to have DISH should be made aware of their pathology, and goals of care, especially with regard to airway management, should be discussed. Discussions of airway management should be centered around intubation versus tracheostomy in the case of airway compromise requiring intervention. Patients looking to avoid a permanent tracheotomy may consider surgical reduction of osteophytes but should be counseled regarding the risks of recurrent laryngeal nerve injury, dysphagia, recurrence, and other associated risks.3,6 Increased awareness of this unusual presentation of a relatively common pathology can lead to improved treatment algorithms for such patients.
Footnotes
Authors’ Note
This manuscript is exempt from institutional review board approval. The manuscript reports a patient’s encounter at a tertiary care center in New Orleans, Louisiana.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.