
Abstract
Objectives:
To evaluate the efficacy of indirect laryngeal biopsy forceps in the treatment of epiglottic abscess (EA).
Methods:
Twenty patients were diagnosed with EA in our department and were randomly divided into group A (indirect laryngeal biopsy forceps combined antibiotics) and group B (antibiotics only). Demographics, the degree of epiglottic and arytenoid swelling, and inflammatory cells were collected for analysis. The drainage of EA was performed under local anesthesia in conscious patients with indirect laryngeal biopsy forceps and 70° direct laryngoscopes. The length of symptomatic relief and length of hospitalization were assessed.
Results:
Ten patients were treated with indirect laryngeal biopsy forceps under the view of the 70° direct laryngoscopes combined with intravenous antibiotics, whereas the other 10 patients were treated with antibiotics only. The differences between the 2 groups had no statistical significance in age, gender, white blood cell count, neutrophils count, and the percent of neutrophils, abscess size, and scope classification at the time of diagnosis. The length of hospitalization and length of symptomatic relief was significantly lower in patients treated with indirect laryngeal biopsy forceps combined antibiotics than those treated with antibiotics only.
Conclusions:
Indirect laryngeal biopsy forceps are safe and effective method to treat EA, which shorten the hospitalization and has the advantages of cost savings and convenience.
Introduction
Epiglottic abscess (EA) is generally considered to be a rare complication of acute epiglottitis, with an incidence of 4%.1-3 Epiglottic abscess may be caused by the misuse of antibiotics, which can result in the generation and spread of antimicrobial resistance. Epiglottitis with EA is more complex and difficult to treat than pure epiglottitis. Despite the conflicting mortality reported in the studies, the potential threat of EA cannot be ignored as it may suddenly cause airway obstruction, which develops the disease into a serious or even life-threatening condition. When symptoms of acute airway obstruction occur, the EA patients need to be transferred to the operating room for further airway management and drainage, usually after tracheal intubation. Previous studies have reported several alternative or complementary treatments to antibiotic therapy include artificial airways, 4 incision and drainage,5-7 and spinal needle aspiration.8,9 However, there is no consensus on optimal methods for treating EA. In this study, we designed a randomized controlled study to assess the effect of indirect laryngeal biopsy forceps in the treatment of EA patients.
Materials and Methods
This study was performed according to the principles expressed in the Declaration of Helsinki. In this study, airway edema may be caused by the operation, which increases the risk of airway obstruction. Therefore, the necessary equipment was prepared for performing an emergency tracheostomy or endotracheal intubation. The study was approved by the local institutional review boards (Reference number 2019077). All participants or their legally authorized representatives gave informed consent.
Study Design
The participating patients diagnosed with EA were more than 18 years old, and the study took place between May 2016 and October 2019. All patients were diagnosed by the radiologist and doctor working in the laryngoscope room (Figure 1) based on laryngoscope observation and contrast-enhanced computed tomography (CT) on the day of admission. The participants were randomly assigned to either group A or B (1:1 ratio with block size 4) using a table of random digits. Patients in group A underwent drainage by indirect laryngeal biopsy forceps and antibiotics, whereas patients in group B were treated with antibiotics only. The protocol was approved by the local institutional review boards and the written informed consent was obtained from all patients for their participation. Exclusion criteria included patients less than 18 years and more than 80 years old, if the abscess was located on the laryngeal surface of the epiglottis, and if the patients could not tolerate local anesthesia by tetracaine.
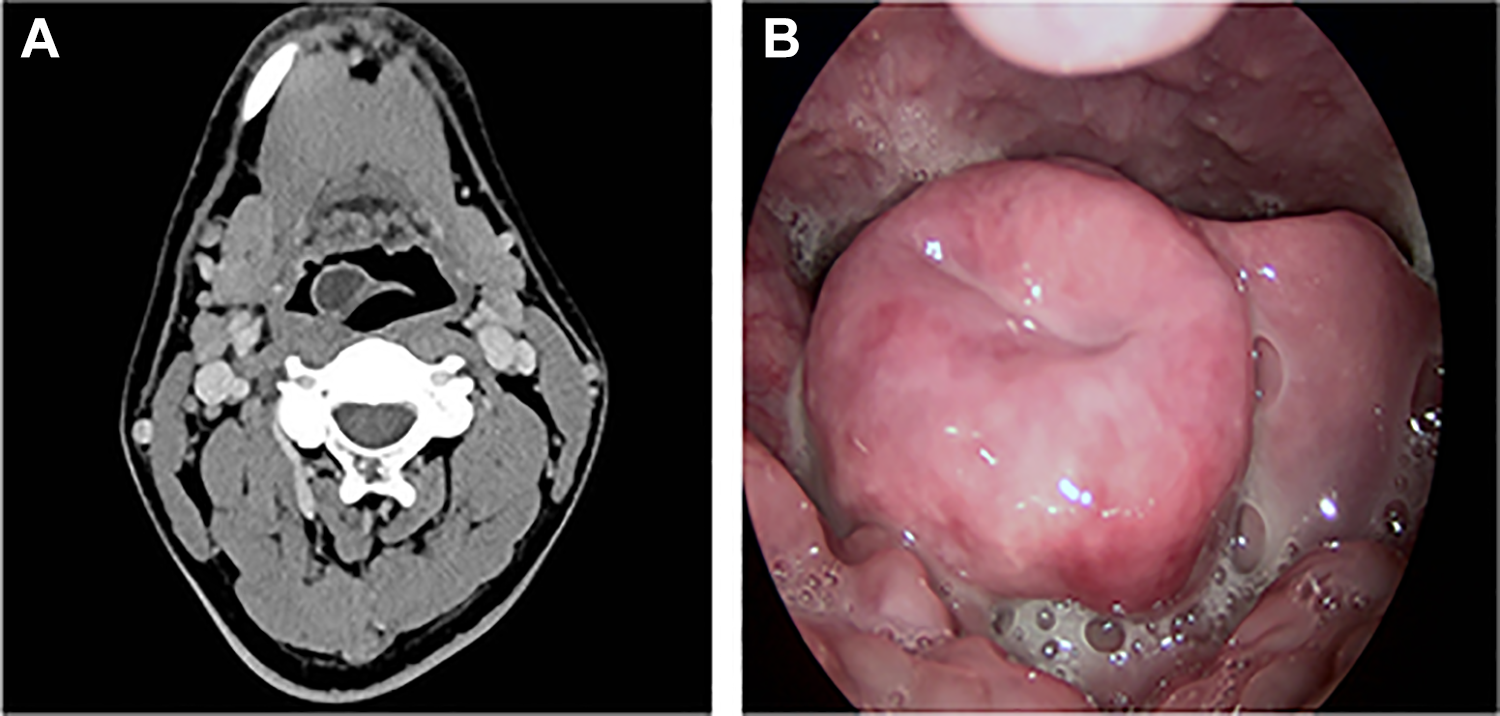
A, Axial contrast-enhanced computed tomography scan demonstrating an epiglottic abscess on the lingual surface of epiglottis. B, The laryngoscope of epiglottic abscess demonstrating epiglottic abscess on the lingual surface of epiglottis.
Treatment Protocol
A senior doctor evaluated the laryngeal aperture of patients using a laryngoscope to identify the status of the airway. Airway intervention should be performed immediately for the patients with laryngeal obstruction more than the second degree, including tracheal intubation or tracheotomy. After the airway was secured, treatments were performed in the basis of the patients’ condition. According to scope classification (SC classification) of epiglottis swelling, laryngoscope findings of patients were classified.
9
I (slight swelling): The epiglottis was slightly swollen, but entire length of vocal folds was still visible by scope. II (moderate swelling): The epiglottis was moderately swollen, with more than half of the posterior vocal folds visible by scope. III (severe swelling): The epiglottis was severely swollen, with less than half of the posterior vocal folds visible by scope.
Furthermore, the arytenoid swelling was observed and categorize as follows: The swelling did not extend to the arytenoids and the aryepiglottic folds. The swelling extended to the arytenoids and the aryepiglottic folds.
9
Procedure for Surgery
After the patients were hospitalized, oropharyngeal swabs were sent for culture. The patients received intravenous administration of third-generation cephalosporin (ceftazidime), ornidazole, and dexamethasone. Patients in group A were treated with antibiotics for 2 days; then they took a 90° sitting position and underwent the epiglottic examination with a 70° direct laryngoscope (Figure 2). After local anesthesia with 1% tetracaine was administered via oral spray for 2 seconds, 3 times, in the view of the 70° direct laryngoscope, the indirect laryngeal biopsy forceps were used to bite the abscess at the most prominent part of EA (Figure 3A and B). After the cotton piece was clamped by the forceps, wrapped around the forceps, and dampened by tetracaine, the forceps were used to press the abscess to let the pus bleed from the break (Figure 2B). The pus from epiglottic abscess was sent for culture. After the operation, the abscess was pressed by the same forceps wrapped by a cotton piece every day in the view of indirect laryngoscope (70° direct laryngoscope was not necessary) until no abscess was found. All surgeries were performed by the same doctor. Minor bleeding was controlled after gargling with ice water. After the operation, patients were placed in a general ward, and monitoring oxygen saturation and the instruments for bedside tracheotomy were needed and prepared. The intensive care unit was prepared in case.
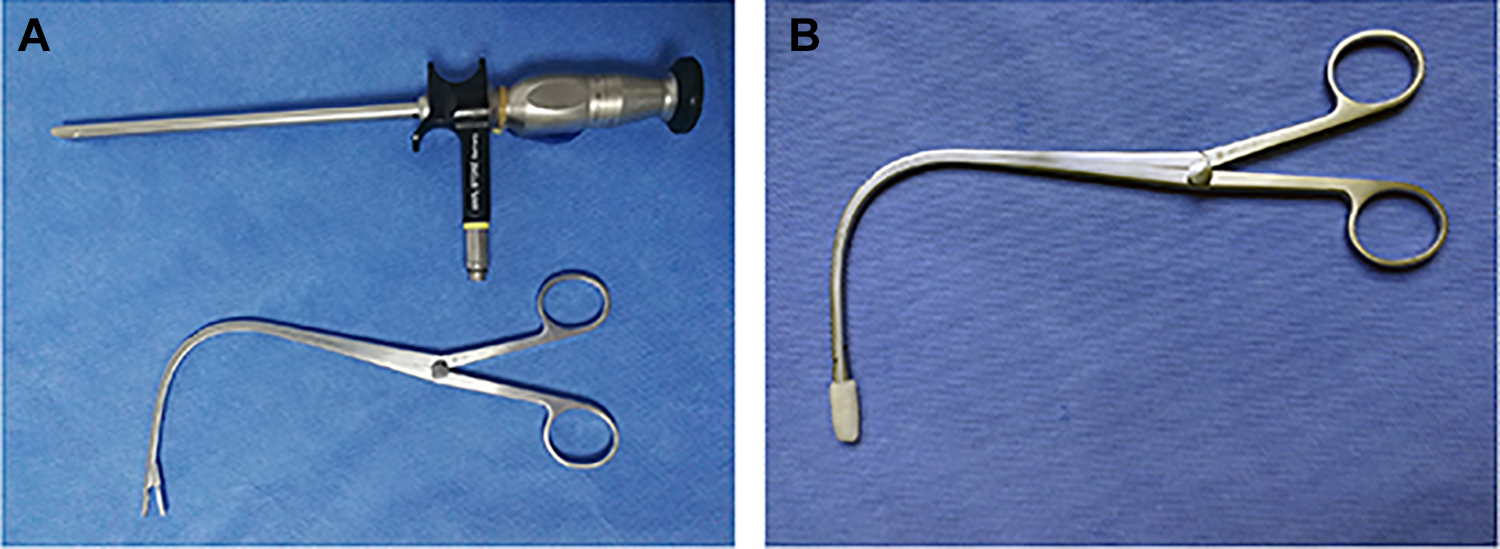
A, Treatment of EA using an indirect laryngeal biopsy forceps, and 70° direct laryngoscope. B, The indirect laryngeal biopsy forceps clamping cotton piece and wrapped by cotton piece was moistened by tetracaine. EA indicates epiglottic abscess.
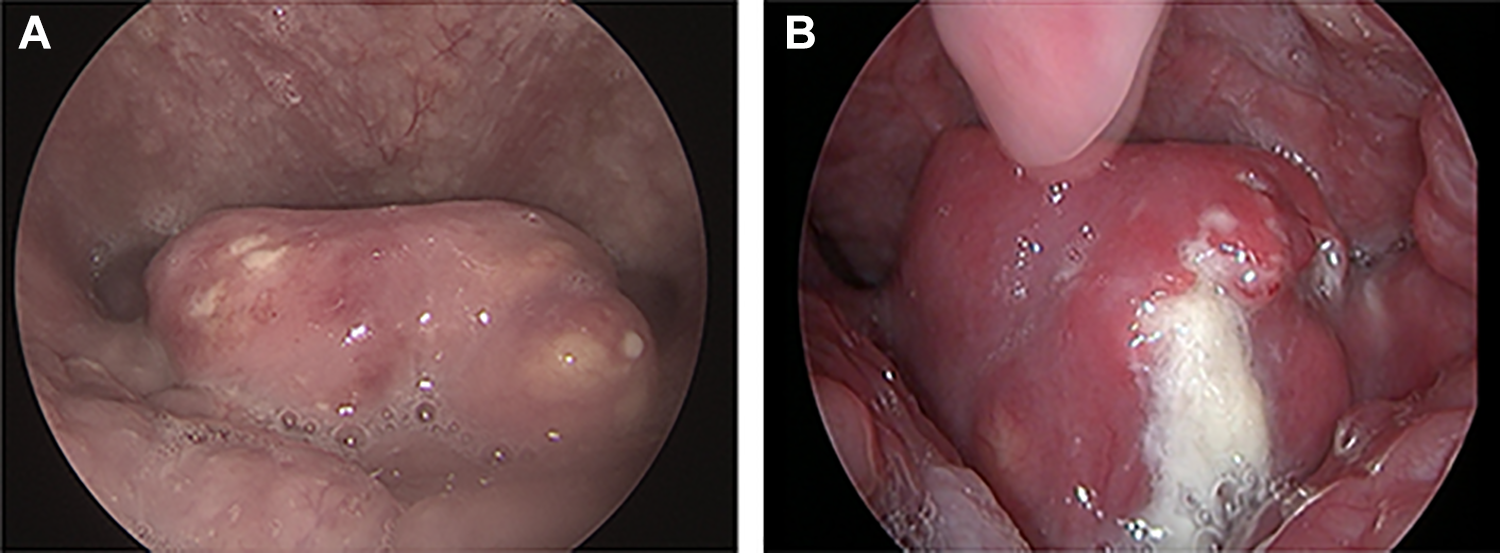
A, The most prominent part of EA which is appropriate for the bite of indirect laryngeal biopsy forceps. B, The pus is out of the EA after the bite of indirect laryngeal biopsy forceps. EA indicates epiglottic abscess.
Patient Follow-Up and Outcome Measures
All patients were evaluated for symptoms (mainly focused on sore throats and dyspnea) during hospitalization. The duration before their symptoms disappeared was recorded. Discharge criteria included a stabilized airway (SC classification group I: the entire length of the vocal folds is visible by scope; status A: swelling did not extend to the arytenoids and the aryepiglottic folds), controlled oral medications for all symptoms, and the patient toleration of soft food. 9 The discharge date was defined as the date of discharge from the hospital.
Statistical Analysis
The SPSS 20.0 program (SPSS, Inc, an IBM Company) was used for the statistical analysis. The continuous variables were analyzed with an independent t test and the categorical variables with the Wilcoxon test. All data were presented as mean ± SD. A P value less than .050 was considered to be statistically significant.
Results
At the time of diagnosis, the clinical characteristics of patients treated with indirect laryngeal biopsy forceps combined antibiotics (group A) were similar to those with antibiotics only (group B; Table 1). The severity of the symptom was examined by laryngoscope, and the epiglottis swelling at inclusion was evaluated by CT (Table 1).
Comparison of Baseline Characteristics, Symptoms, Scope Classification, and Laboratory Findings in 2 groups.
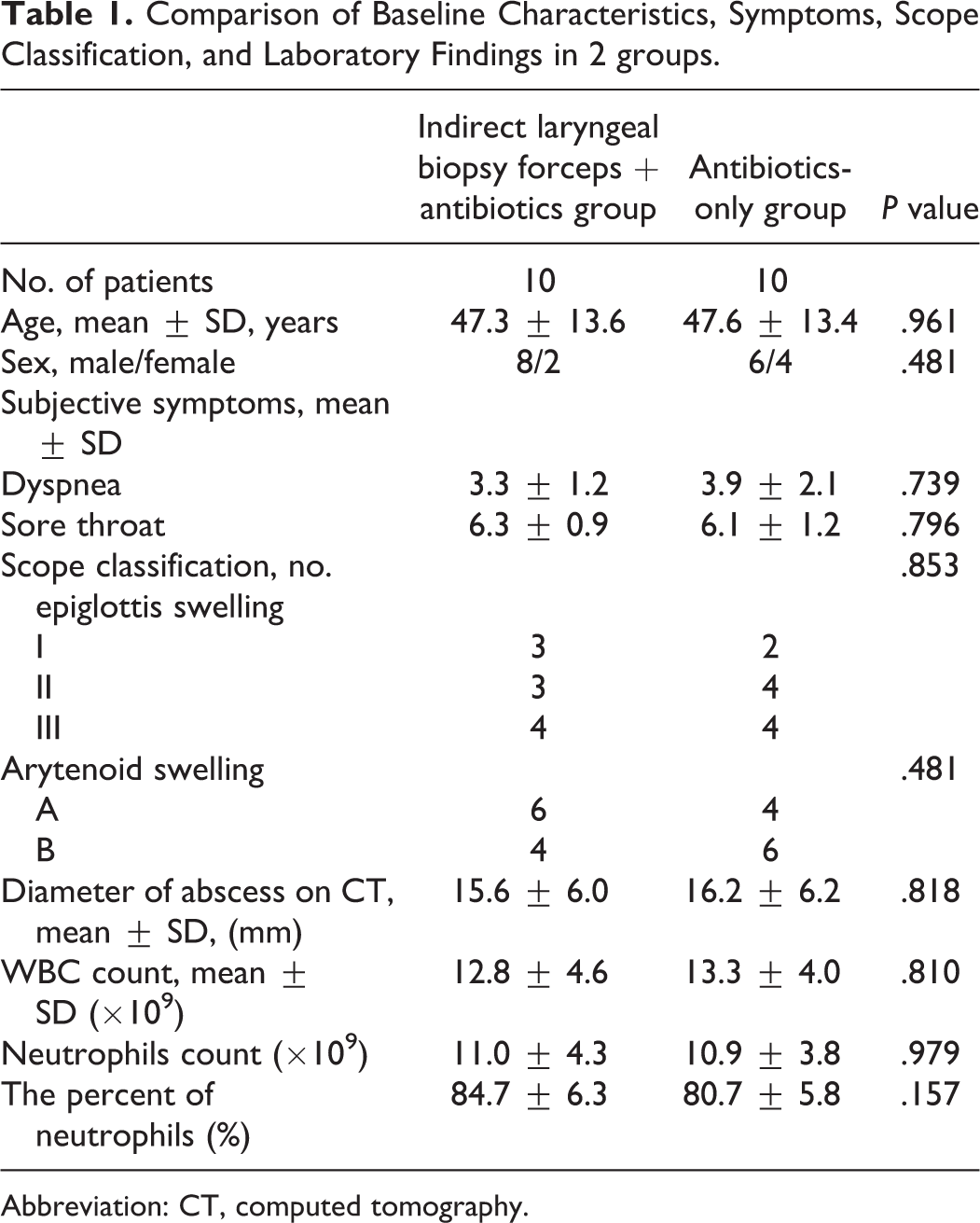
Abbreviation: CT, computed tomography.
The difference of arytenoid and epiglottic swelling between the 2 groups was not significant. The mean diameter of the abscess was not significantly different on contrast-enhanced CT between the 2 groups. Furthermore, no significant difference was found in the results of hematologic examination including the mean white blood cell count, neutrophils count, and the percent of neutrophils at the time of presentation (Table 1). However, the parameters, including the length of symptomatic relief and the length of hospitalization, were statistically and significantly different between the 2 groups (Table 2). The average length of hospitalization was 4.80 ± 2.15 days in the indirect laryngeal biopsy forceps and antibiotics group (A), and 8.30 ± 4.14 days in the antibiotics-only group (B).
Comparison of Time to Symptom Resolution and Length of Hospitalization.a
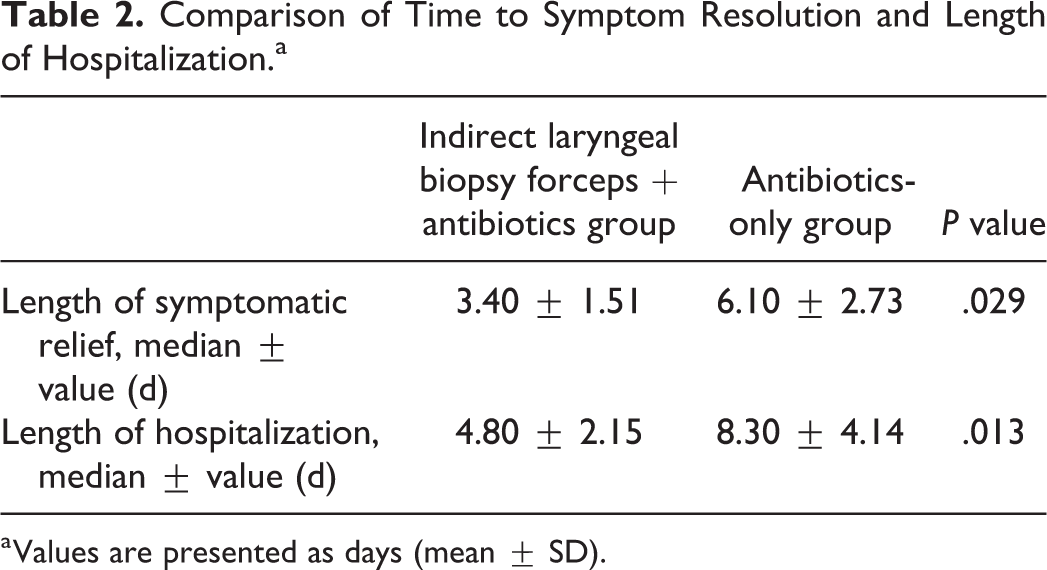
a Values are presented as days (mean ± SD).
The abscess most frequently appear on or near the lingual surface of the epiglottis. Patients had no preceding symptoms of acute pharyngitis. The oropharyngeal swab cultures showed streptococcus was isolated more frequently and that many other pathogens existed, including Pseudomonas fluorescens and Klebsiella pneumoniae. However, cultures of the pus from the abscess from all 10 patients in group A failed to yield bacteria. One patient in group B had tracheostomy because of third-degree laryngeal obstruction during the treatment by medicine in group B.
Discussion
Epiglottic abscess is a life-threatening disease which could develop a rapid and a fulminant course. The treatment of EA was immediate for airway management, incision and drainage of EA, and the use of antibiotics in previous studies.2,6,10 In a previous study, 79.2% of EA received incision and drainage under general anesthesia. 11 However, many of EA had a stable airway and localized abscess without progression. There was no consensus on how to screen patients requiring prophylactic airway intervention. 12 Thus, an appropriate and convenient method is needed for patients with stable airways and patients who have been treated by tracheotomy. Thus, the prospective randomized trial was designed to analyze the efficacy of the laryngeal biopsy forceps in the treatment of EA.
Epiglottic abscess often occurred on the lingual side or free edge of the epiglottis and can be observed and diagnosed by laryngoscope. The hidden abscess formation could be found by magnetic resonance imaging and contrast-enhanced CT.
The indirect laryngeal biopsy forceps were safe and effective in the treatment of EA. In our study, patients who were treated with indirect laryngeal biopsy forceps and antibiotics had a shorter hospital stay and shorter symptomatic relief time than those treated with medicines only. In addition to the discomfort caused by the tetracaine and a small amount of bleeding that could be controlled by gargling with ice water, there was no complication after the operation in our study. Compared to the general anesthesia, the treatment of EA by the laryngeal biopsy forceps under local anesthesia was more convenient, simpler, and less expensive, and the laryngeal biopsy forceps pressed the EA under indirect laryngoscope which was very convenient after the operation by a 70° direct laryngoscope.
The operations were not done immediately on the day of admission. After 2 days of medication, the most prominent part of the abscess was easier to be found. Then, the indirect laryngeal biopsy forceps could only cause small trauma. The cotton piece was clamped by the forceps to avoid sliding the cotton piece during the operation. The cotton piece was wrapped around the forceps when the abscess was pressed by the forceps to avoid unnecessary trauma. Lee et al 9 used spinal needle aspiration in the view of a rigid endoscope for the treatment of EA. Compared to our method, the spinal needle is a sharp instrument and can cause unnecessary damage when the patients’ epiglottis moves due to the gag reflex. Furthermore, the rigid endoscope was used every day when the operation was performed. Our surgery was simple and effective because the biopsy forceps were blunt and damage could only be caused when it bit the abscess. In addition, the indirect laryngoscope was used after the first operation. Lastly, our method was especially advanced in the treatment of multiloculated or honeycomb like EA because the abscess could be pressed by the indirect laryngeal biopsy forceps.
In this study, none of the 20 patients had diabetes mellitus or a history of foreign body ingestion, which are risk factors for EA. 13 The cultures of the pus of the abscess from all 10 patients in group A failed to yield bacteria, which was probably due to antibiotic treatments for 2 days after admission.
It is worth noting that only 1 patient with EA required tracheostomy in this study. This result contradicts the previous findings that the formation of EA was a predictor of airway obstruction.14-16 This contradiction may be caused by the pus pressed from EA, and the space in the throat cavity was enlarged. Another reason could be that patients had different levels in disease severity, which means that the EA patients in this study may not be as severe as those previous studies.
The equipment was prepared for emergency tracheostomy or endotracheal intubation during aspiration; however, none were used. The discomfort from epiglottis surgery in local anesthesia included nausea, vomiting, and coughing. In addition to the discomfort caused by the gag reflex and mild bleeding during the operation, no complication was observed after laryngeal forceps in this study. The risk of pus aspiration during the procedure was a possibility; however, aspiration did not occur in any patient. This is because of the cough reflex that still existed after the use of tetracaine. However, the preparation for any emergency tracheostomy or endotracheal intubation and close postoperative monitoring was still mandatory.
A challenge and possible limitation in this study was the small sample size, which was caused by the low incidence rate of EA. A study containing large-scale samples is required for further analysis.
Conclusion
The results of this study indicate that indirect laryngeal biopsy forceps is a safe and effective method to treat EA, which shorten the hospitalization and has the advantages of cost savings and convenience. These results provide additional options for clinical treatment of EA.
Footnotes
Authors’ Note
The authors alone are responsible for the content and writing of the paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Science and Technology Commission of Shanghai Municipality (CN) [grant number 18411965600].