
Abstract
Objective:
To study the potential changes of health-related quality of life (HRQL), voice quality, and communicative function up to 24 months following radiotherapy for patients with laryngeal cancer.
Methods:
A total of 28 patients with laryngeal cancer, treated by curatively intended radiotherapy were included in this prospective longitudinal descriptive study. Patients were followed pre-radiotherapy, 12 months, and 24 months post-radiotherapy. At each time point, voice recordings and patient-reported outcome instruments (European Organization for Research and Treatment of Cancer Quality-of-Life Questionnaire Core30, Head and Neck35, Swedish Self-Evaluation of Communication Experiences after Laryngeal Cancer) were completed. Perceptual analysis using the Grade-Roughness-Breathiness-Asthenia-Strain was performed using the voice recordings.
Results:
Voice quality remains inferior to the voices of healthy controls both before and up to 24 months post-radiotherapy, demonstrating no statistically significant changes during the study period. Self-perceived communicative function revealed a trend toward improvement. Health-related quality of life remains mostly at stable levels, however, with statistically significant deterioration regarding dry mouth and sticky saliva. Generally, patients reported inferior scores compared to a normal population.
Conclusion:
This study demonstrated no statistically significant changes over time in HRQL and perceptual voice quality at pre-radiotherapy compared to 24 months post-radiotherapy. However, the values remain inferior to the voices of healthy controls or a normal population.
Introduction
Laryngeal cancer afflicts approximately 180 patients annually in Sweden. 1 In both early and advanced stages, the disease is often managed with organ-preserving treatments such as radiotherapy. Tumor control and survival for this patient group is high. However, organ-preserving treatment may not always be synonymous with function-preservation. Both the tumor itself and subsequent oncologic treatment affect voice, vocal communication, and health-related quality of life (HRQL).2-5
Patients with laryngeal cancer following radiotherapy often present with a mild to moderate dysphonia.2,6 The voice problems have been shown to persist up to 5 years post-radiotherapy in 50% to 95% of patients, and are typically characterized by a rough, breathy, and strained voice quality.7-9 The patient’s self-perceived voice and communication as well as HRQL are important components in the multidimensional assessment post-radiotherapy. 10 However, many HRQL instruments contain only a few or single statements regarding voice and communication, making instruments specifically addressing communicative ability vital to assess rehabilitative needs in this patient population.4,11,12 At diagnosis, general HRQL and communication function for head and neck cancer patients are significantly reduced compared to the normal population. 13 Immediately after post treatment, there is a deterioration of HRQL, which returns to pretreatment levels at 12 months post-radiotherapy, with the exception of treatment-specific side-effects including salivary function.5,8 A previous study by Karlsson et al of patients with irradiated laryngeal cancer during the first 12 months following radiotherapy 8 demonstrated improvement of voice quality immediately after radiotherapy, albeit with a statistically significant deterioration between 6 and 12 months.
Previously, laryngeal cancer management has focused primarily on survival rates and tumor control but has evolved to incorporating functional and HRQL outcomes. Several studies evaluating the functional outcomes exist, but are unfortunately retrospective in design, do not use combinations of multidimensional assessment tools nor do they include pretreatment measures or normative comparison. 3 The aim of this study is to follow-up and investigate the changes in perceptual and patient-reported outcomes (PRO) up to 24 months post-radiotherapy for patients with laryngeal cancer.
Method
Study Population
Data were collected at Sahlgrenska University Hospital, Gothenburg, Sweden. All patients diagnosed with laryngeal cancer treated curatively with radiotherapy ± chemotherapy from March 2000 to December 2011 were eligible for inclusion. Inclusion criteria were Swedish language competency to independently answer the questionnaires. Eighty-nine patients were available for inclusion. Comorbidity was measured using the Adult Comorbidity Index Evaluation-27 (ACE-27).14,15
Study Design
In this prospective descriptive longitudinal study, patients were followed at 3 time points: pretreatment, 12 months post-radiotherapy, and 24 months post-radiotherapy. At each visit, the voice was recorded and PRO instruments, as described below, were answered. A total of 28 patients out of 40 had data available at all 3 time-points. Twelve patients had dropped out of the study end point (24 months) and were thus not included in the analysis. Reasons for drop-out were terminated participation (n = 6), laryngectomy (n = 3), missed recording (n = 1), and deceased (n = 2).
Oncologic Treatment
All patients received radiotherapy with curative intent according to regional treatment guidelines and was either hyperfractionated (n = 10) or conventional (n = 18). Conventionally fractionated radiotherapy was administered once daily in 2 to 2.4 Gy fractions totaling 62.4 to 68 Gy. Hyperfractionated radiotherapy consisted of 1.7 Gy doses given twice daily to a total of 64.6 Gy. Most patients with T2 to T3 tumors also received irradiation to the lymph nodes to a total of 40.8 Gy (1.7 Gy twice a day, 5 days a week n = 13) or 46 Gy (2.0 Gy once a day, 5 days a week n = 4). No patient received chemotherapy.
Voice Recordings
Voice recordings included reading of a standard passage and the maximum sustained vowel /a/. A headset microphone (Sennheiser MKE 2-p) was set at a distance of 12 cm from the corner of the mouth. Recordings were made at a sampling frequency of 44.1 kHz with a Panasonic Professional Digital Audio Tape (DAT) Recorder SV-3800. Prior to analysis, all recordings were transferred from a DAT to a computer hard drive as an audio file (.wav) using the program Swell Soundfile Editor, version 4.5 (Saven Hightech).
For perceptual rating, samples from the voice recordings were cut using Swell Soundfile Editor (4.5). The rating samples included the first 2 sentences of the standard passage and the recorded prolonged vowel /a/ and were saved as audio files (.wav). Fifteen percent of samples were randomly reduplicated for intra-rater reliability calculations. All samples were then randomly compiled with anchor samples interspersed, at every 20 voice samples, into the final rating file for perceptual analyses.
Perceptual Analyses
Perceptual ratings were conducted by 2 experienced speech-language pathologists. The raters attended a half-day’s consensus training based on the format of Iwarsson and Petersson. 16 The raters were blinded to patient status and voice sample information. The rating protocol used the Grade-Roughess-Breathiness-Asthenia-Strain (GRBAS) scale 17 which is a commonly used voice evaluation protocol in studies concerning laryngeal cancer.18-20 The GRBAS consists of 5 voice qualities: grade, roughness, breathiness, asthenia, and strain. Each voice quality is rated on a 4-point scale, where 0 = normal, 1 = mildly impaired, 2 = moderately impaired, and 3 = severely impaired. The vocal fry parameter (rated on a 4-point scale mirroring the GRBAS) was added to the rating protocol as it has also been reported in irradiated voices.21,22
Patient-Reported Outcomes
Swedish Self-Evaluation of Communication Experiences after Laryngeal Cancer (S-SECEL)
The Swedish Self-Evaluation of Communication Experiences after Laryngeal Cancer (S-SECEL) covers communication experiences and dysfunction in patients with laryngeal cancer. 11 It has demonstrated high reliability, convergent and discriminant validity, and satisfactory internal consistency.12,23 The S-SECEL consists of 35 items in 3 domains (general, environmental, and attitudinal) and a total score domain, totaling 34 questions and 1 separate question not included in the scoring. Each item is rated on a 4-point scale ranging from 0 (never) to 3 (always) and recalls the last 30 days. The cumulative subscale scores range from 0 to 15 for general, 0 to 42 for environmental, 0 to 45 for attitudinal, and 0 to 102 for total, where a higher score indicates greater perceived communicative dysfunction. 12 For the S-SECEL, threshold values indicating the need for vocal rehabilitation have been proposed, where scores exceeding 20 points corresponds to the need for vocal rehabilitation. 24
European Organization for Research and Treatment of Cancer QLQ-C30 and EORTC QLQ-H&N35
The European Organization for Research and Treatment of Cancer (EORTC) has developed questionnaires specifically investigating the HRQL for patients with cancer. The Core-30 questionnaire (EORTC Quality-of-Life Questionnaire [QLQ]-C30 version 3.0) includes 30 items addressing patient functioning and symptomatology over the last week. 25 The head and neck module (H&N35) includes an additional 35 items which cover symptoms specific to H&N cancer. 26 Calculated scores for each item or domain range from 0 to 100. On functioning domains and Global QOL domains, a higher score indicates better functioning whereas on symptom domains or single items, higher scores represent increasing symptom burden. For the EORTC QLQ-C30 and H&N35, a difference of 10 points may be considered clinically significant. 27
Statistical Analyses
The SPSS version 25.0 for Mac was used for analyses. Mean values and standard deviation were used for descriptive purposes. Nonparametric, 2-tailed tests were used and the significance level was set at P < .05. For continuous data, calculation of differences over time was carried out with the Friedman analysis of variance. In cases of significant results, additional analysis was performed with pairwise comparisons in order to identify between which study occasions the changes occurred. For ordered categorical data, change over time was calculated with the Sign test. The magnitude of changes was analyzed using effect sizes (ESs). Effect size of within-group change was calculated as mean change between follow-up and pre-therapy (baseline) divided by the standard deviation of change. Effect size was interpreted according to Cohen standard criteria, where size is classified as trivial (0-<0.2), small (0.2-<0.5), moderate (0.5-<0.8), or large (≥0.8). Inter- and intra-rater reliability was calculated using percent exact agreement and weighted κ, which was interpreted using Landis and Koch guidelines. 28
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Regional Ethical Review Board in Gothenburg, Sweden. Parts of this study population have been described previously.8,29
Results
The patient characteristics are listed in Table 1. The results of the perceptual voice analyzes with the GRBAS revealed that at 24 months post radiotherapy, roughness and strain were the qualities that occur most frequently (Table 2). There were no statistically significant changes during the study period for any of the GRBAS parameters. However, a tendency of deterioration in strain was found, since only 4% were rated as having “no strain” at 24 months compared to 29% at baseline. Regarding breathiness, a tendency toward improvement was observed, as no patients were rated as having “severe breathiness” at 24 months and only 12% have “moderate breathiness,” compared to 7% and 21%, respectively, at baseline. The Weighted κ for inter-rater reliability was 0.45, indicating moderate agreement, and the percent exact agreement was 48%. The weighted κ for intra-rater reliability was 0.59, indicating moderate agreement and percent exact agreement 70%.
Patient Demographics at Baseline (Pre-Radiotherapy).
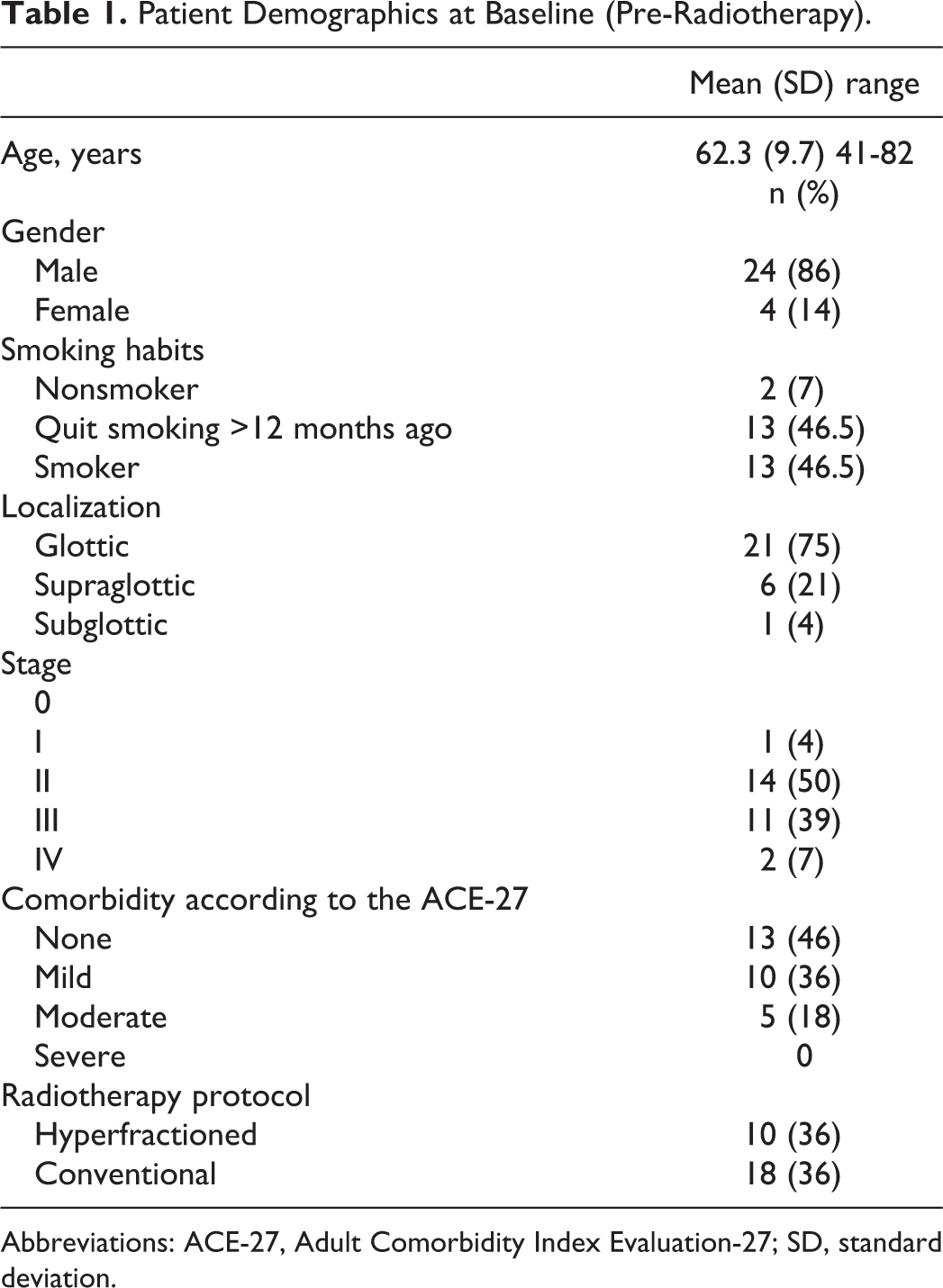
Abbreviations: ACE-27, Adult Comorbidity Index Evaluation-27; SD, standard deviation.
Perceptual Evaluation According to the Grade-Roughess-Breathiness-Asthenia-Strain (GRBAS) at Study Occasions.a
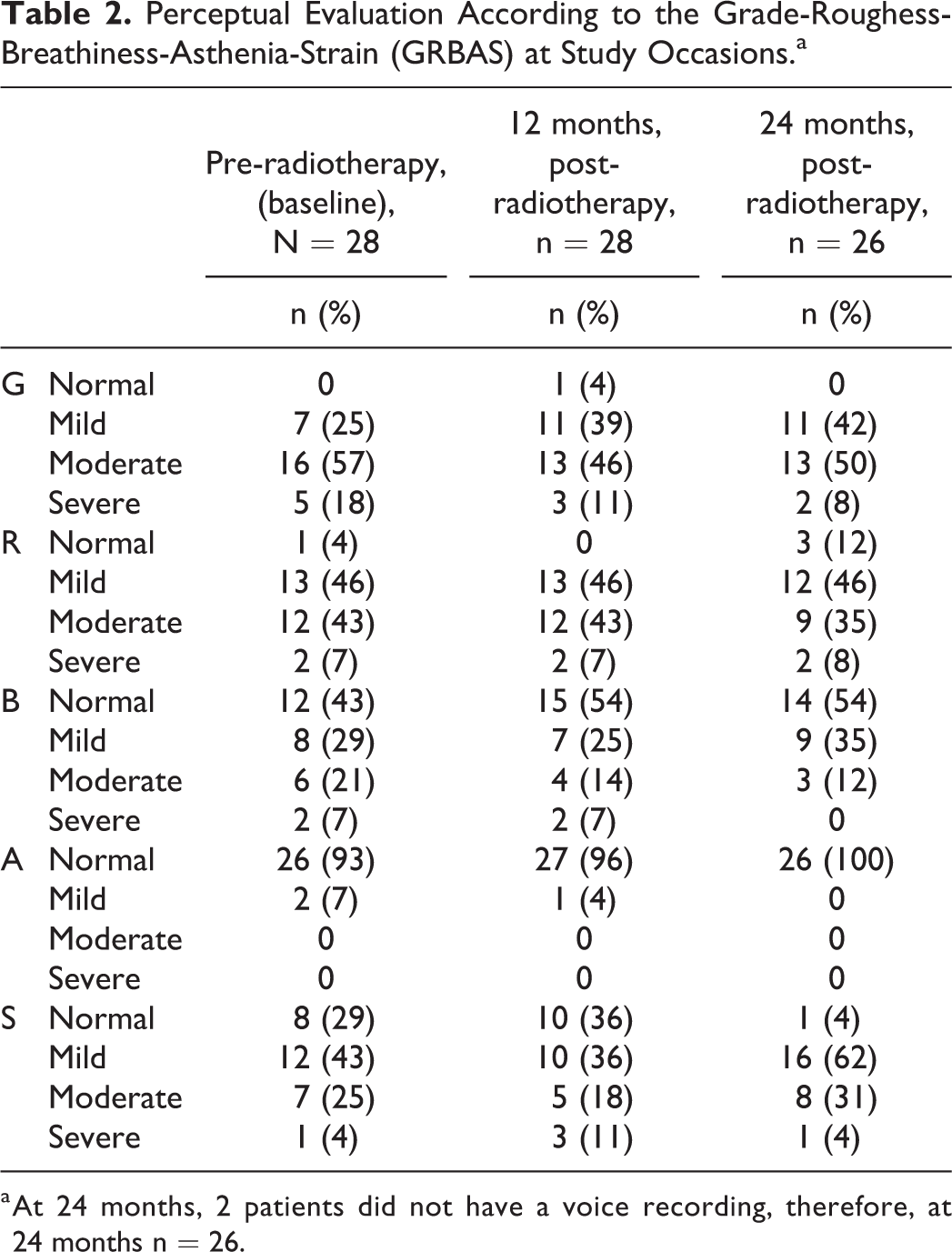
a At 24 months, 2 patients did not have a voice recording, therefore, at 24 months n = 26.
Table 3 lists the data reported in terms of communicative function as measured by S-SECEL at each study time point. No statistically significant changes occurred during the study period in any of the S-SECEL domains. However, when looking at the mean total score at baseline was 22.7, with a tendency for improvement to 16.3 points at 12 and 24 months post-radiotherapy. The latter value is below the cutoff score (<20 points) of the S-SECEL indicating no communicative dysfunction. 21 All changes demonstrated a small ES.
Mean Values (SD) for S-SECEL Scores Pre-RT, 12 Months Post-RT, and 24 Months Post-RT Including P Values and Effect Sizes for Changes at Follow-Up Compared to Baseline (Pre-RT).a
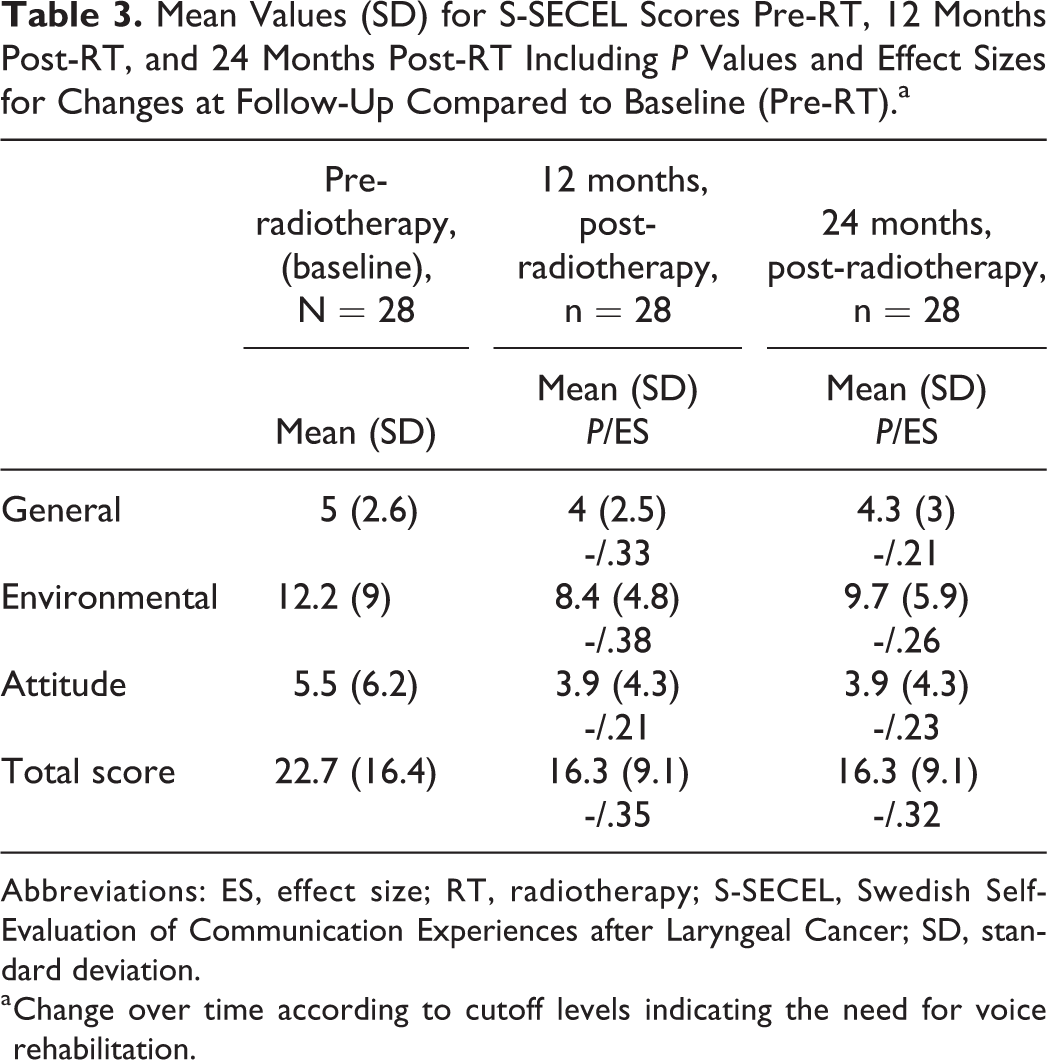
Abbreviations: ES, effect size; RT, radiotherapy; S-SECEL, Swedish Self-Evaluation of Communication Experiences after Laryngeal Cancer; SD, standard deviation.
a Change over time according to cutoff levels indicating the need for voice rehabilitation.
The results of the EORTC QLQ-C30 are reported in Table 4. There was a general trend where all domains improved, that is, the mean values of all functional and symptom domains were better at 24 months post-radiotherapy compared to baseline (pre-radiotherapy). Statistically significant differences are found in 4 of the 15 domains, mainly among the function domains.
EORTC QLQ-C30 Scores Pre-RT, 12 Months Post-RT, and 24 Months Post-RT Including P Values and Effect Sizes for Changes at Follow-Up Compared to Baseline (Pre-RT).a
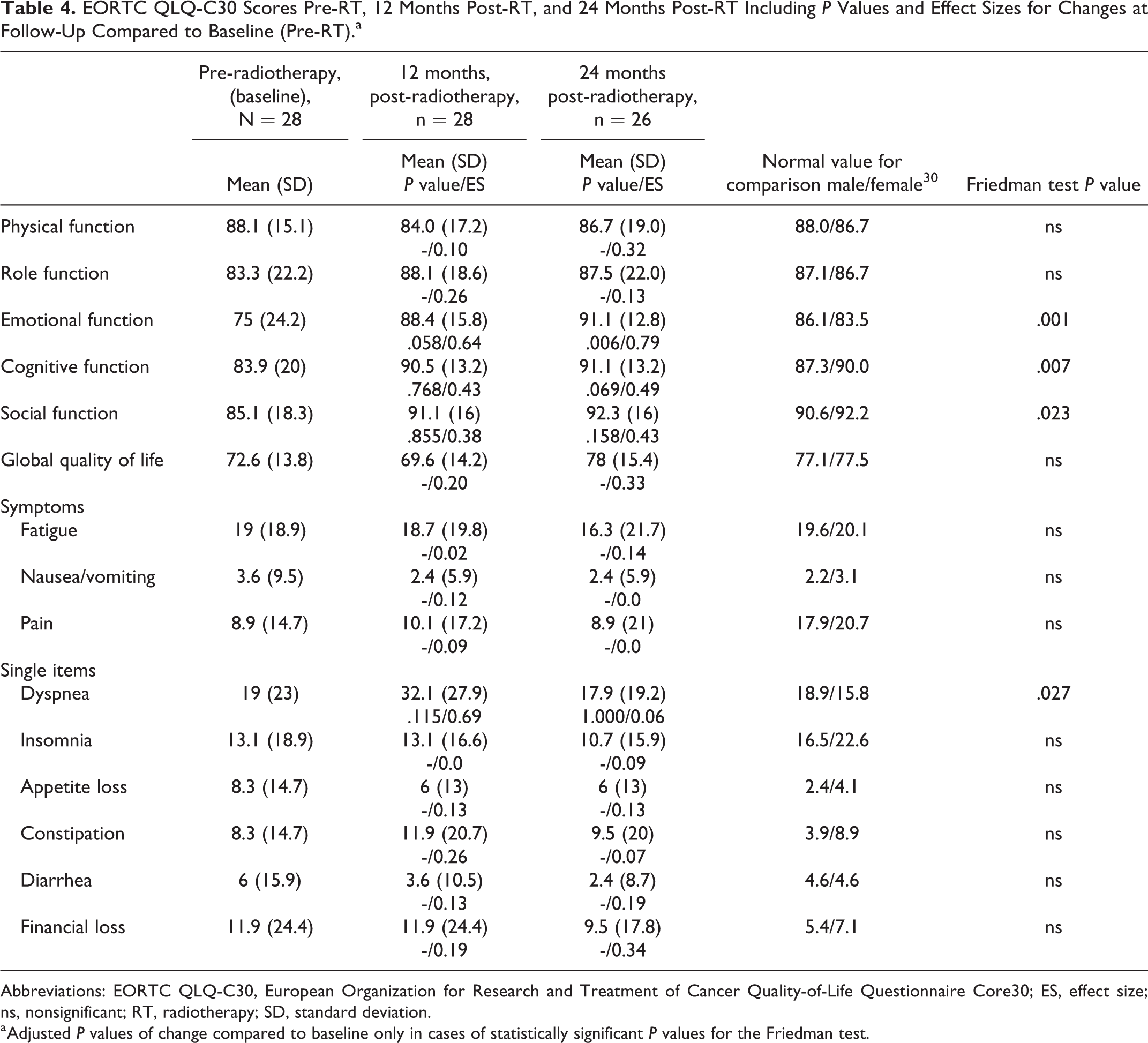
Abbreviations: EORTC QLQ-C30, European Organization for Research and Treatment of Cancer Quality-of-Life Questionnaire Core30; ES, effect size; ns, nonsignificant; RT, radiotherapy; SD, standard deviation.
a Adjusted P values of change compared to baseline only in cases of statistically significant P values for the Friedman test.
Results of the EORTC QLQ-HN35 are reported in Table 5. Statistically significant differences are found in the single item domains dry mouth, sticky saliva, and pain killers. However, a follow-up analysis reveals that only a statistically significant deterioration was found in the dry mouth when comparing 24 months to baseline. No statistically significant differences were found in the symptom domains. However, small to moderate ESs of improvement are found in a majority of the domains. The domain senses demonstrated a trend toward deterioration over time, with a small ES when comparing the 24 months follow-up and baseline. Remaining domains and single items obtain similar results at all 3 study occasions.
Mean Values (SD) for EORTC HN35 Scores Pre-RT, 12 Months Post-RT, and 24 months Post-RT Including P Values and Effect Sizes for Changes at Follow-Up Compared to Baseline (Pre-RT).
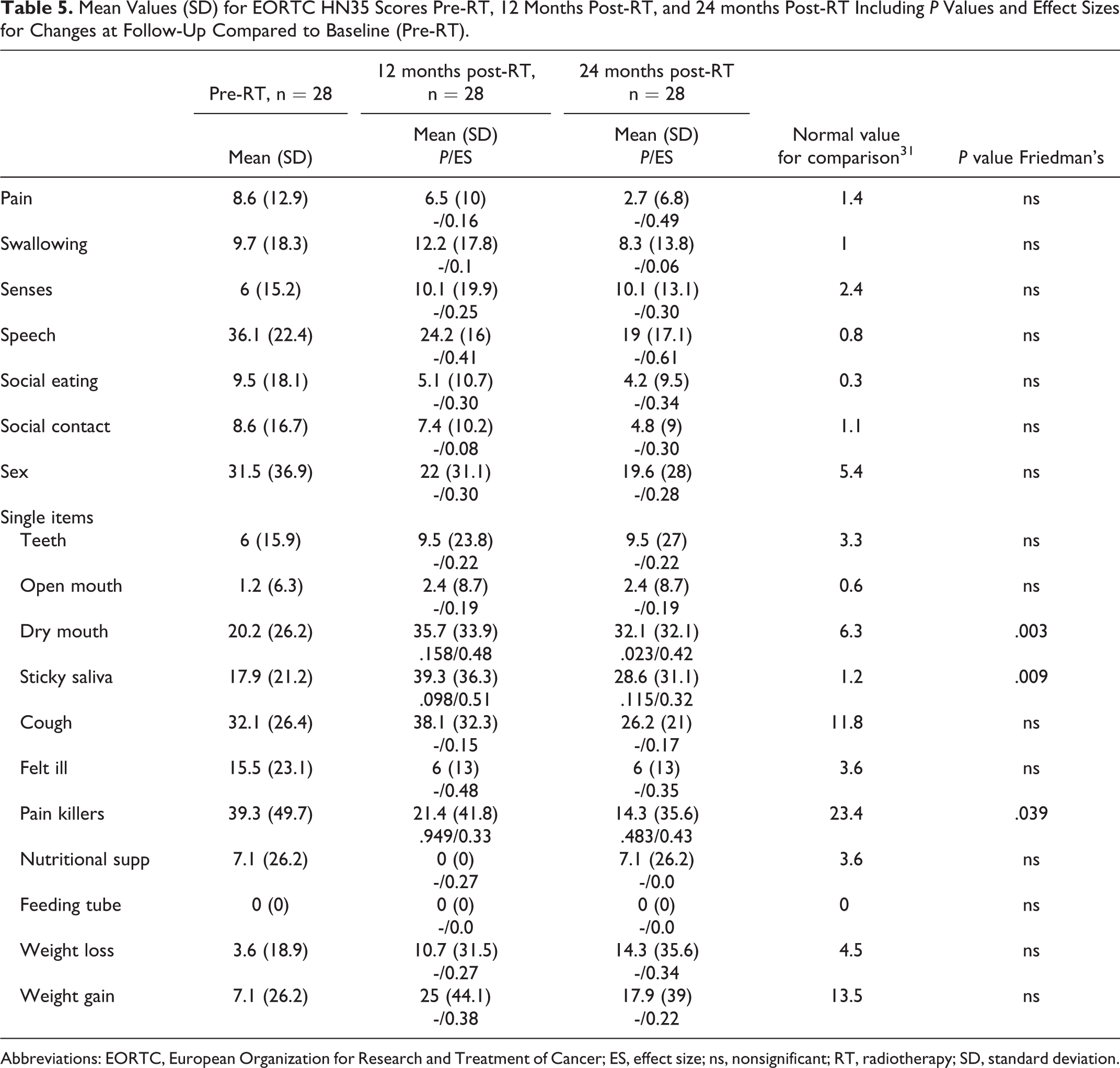
Abbreviations: EORTC, European Organization for Research and Treatment of Cancer; ES, effect size; ns, nonsignificant; RT, radiotherapy; SD, standard deviation.
Discussion
This study aimed to describe the subjective and objective changes of voice and HRQL over time in a laryngeal cancer cohort, from pre-radiotherapy up to 24 months post-radiotherapy. The results revealed no statistically significant changes occurring over time regarding the perceptual evaluation using GRBAS. The functional domains of the EORTC QLQ-C30 demonstrated some improvement over time. Several domains remained unchanged, while some domains of the H&N35, such as the dry mouth and sticky saliva deteriorated over time. Even though statistically significant improvements occurred in several domains, the values at 24 months post-radiotherapy still differ substantially and are far inferior to that of published normal values.30,31 Over time, only a few statistically significant changes are seen in this study, while in most of the variables, whether it be in the perceptual measures of the GRBAS or the PRO; S-SECEL, EORTC QLQ C30, or the H&N35, several of the values remain similar to baseline also at 24 months. This is probably due to the initial voice function and HRQL being affected by the tumor itself and the receiving of a cancer diagnosis, whereas after treatment, the values inferior to healthy controls could be explained by side effects of the radiotherapy treatment. If so, no significant numeric change would be observed albeit the reason for the low scores vary at the time points.
The results of the GRBAS demonstrated that the most common voice qualities at 24 months post-radiotherapy were strain and roughness. The results regarding roughness remain around the same levels, where 50% present with moderate to severe roughness at 12 months, compared to 43% at the 24-months follow-up. This is in line with a previous study, indicating that the voice quality for patients treated for laryngeal cancer remains relatively stable from 12 months up to 10 years. However, these values are still inferior to those of a normal population. 32 Karlsson et al demonstrated that the parameter roughness deteriorated between 6 and 12 months following radiotherapy, results which are not seen in the present study. This indicates that the deterioration of voice quality, that is, roughness, is temporary, and a spontaneous recovery can be expected over time. 8 However, Millgård and Tuomi 29 reported the GRBAS values of a vocally healthy control group, where all of the vocally healthy subjects presented with either normal or mild roughness and strain, indicating that the patients with laryngeal cancer in the present study demonstrate values inferior to those of vocally healthy subjects regarding voice quality prior to, and up to 2 years post radiotherapy.
The high prevalence of roughness and strain could be explained by the tumor itself which may hinder the glottic closure. Following treatment, vocal folds often present with scarring, inflammation, edema, fibrosis, and impaired vocal fold function.7,33 Additionally, the patients in the present study report values indicative of dry mouth and sticky saliva far inferior to the values of a normal population, which also could affect and contribute to poor vocal function. 34
As shown by the S-SECEL results, the communicative function remains relatively stable over time. However, compared to the suggested threshold value of the total domain, values above 20 points should indicate the need for voice rehabilitation. 24 At 12 and 24 months respectively, the mean values are below this threshold, indicating that the communicative function improves slightly, albeit no statistically significant change is demonstrated. Similarly, the values of the speech domain of the H&N35 indicates a trend of improvement, where the mean score at baseline is 36.1 compared to 24.2 and 19 at 12 and 24 months, respectively, a difference that would be deemed as clinically significant. 28 The trend toward change seems to be most prevalent during the first year following radiotherapy, similar to previous studies.32,35
In general, the scores of the EORTC QLQ-C30 are similar to the results of a normal population at all occasions, except for pain, which is actually better for the patients with laryngeal cancer. 30 This might be an indication that the EORTC QLQ-C30 does not cover the specific aspects and important areas for patients with laryngeal cancer. When comparing EORTC QLQ H&N35 values to that of a normal, 31 the patients in this study report inferior values at all time points, in almost all domains. In order to cover the potential changes over time and survey areas of interest for patients with laryngeal cancer, questionnaires covering more specific items such as communication, swallowing and nutrition, as well as social aspects and xerostomia-related matters should be used for this patient group.
This study is limited by the large drop out, where only approximately 75% of the original study population remained at 24 months post-radiotherapy. Another limitation to this study is the heterogenity of the sample, including different laryngeal localization and stages of the tumors, which may affect the results. A larger number may have resulted in the possibility of subgroup analyses for example regarding tumor stage, sex, and radiotherapy protocol. Additionally, the inter- and intra-rater agreement of the perceptual analyses are only moderate, which needs to be taken into consideration when interpreting the results. A better agreement might yield a different result regarding the perceptual voice evaluations.
Conclusion
This study demonstrated no statistically significant changes over time in HRQL and perceptual voice quality at pre-radiotherapy compared to 24 months post-radiotherapy. However, the values remain inferior to the voices of healthy controls or a normal population. This indicates that the patient with laryngeal cancer might need support regarding several areas such as nutrition, swallowing, voice rehabilitation, before, during, and up to 24 months post-radiotherapy.
Footnotes
Acknowledgments
This study was supported by the Assar Gabrielsson foundation, the Swedish Cancer Society, the Research and Development Council (FoU) in Region Va¨stra Go¨taland, the Sahlgrenska University Hospital, and the Medical Faculty of Gothenburg University, Sweden.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.