
Abstract
Significance Statement
This case highlights the consequences of colon interposition on phonation and swallowing. Findings in this patient included laryngopharyngeal reflux, vocal fold paralysis, poor esophageal peristalsis, failed bolus transfers, and others. The mechanical and functional differences between the colon and the esophagus can impact bolus transfer, reflux, and phonation. Further research is required to identify the mechanisms by which colon interposition can impact voice and swallowing.
Case
This 32-year-old male had a history of Marfan syndrome, abdominal aortic aneurysm (AAA), and aortic dissection. Revision surgery for AAA repair resulted in complications requiring total gastrectomy, colon interposition, and a 1-year intensive care unit stay with a tracheotomy. Following tracheotomy reversal, the patient noted hoarseness, breathiness, voice fatigue, hypophonia, odynophagia, and dysphagia with liquids. He also reported coarsening of the voice with increased use, worst at the end of the day. His dysphonia prevented him from working and partaking in his hobbies of coaching basketball and singing.
Strobovideolaryngoscopy revealed muscle tension dysphonia, laryngopharyngeal reflux (LPR), Reinke’s edema, left vocal fold paralysis with bowing and atrophy, and left arytenoid cartilage prolapse (Figures 1 –3). Esophageal manometry showed no identifiable lower esophageal sphincter consistent with gastrectomy and colon interposition. The neo-esophagus had no normal pressures or peristalsis. All swallows were weak, uncoordinated, and failed. No swallows resulted in complete bolus transfer. Twenty-four-hour pH impedance testing on 20 mg famotidine recorded 54 reflux events, 35 of which were weakly acidic. The pH recorded was less than four 5.3% of the time, and the patient’s DeMeester score was 22, both of which were elevated. Magnetic resonance imaging and computed tomography scan revealed a laterally deviated left vocal fold. Laryngeal electromyography showed only 10% recruitment of the left thyroarytenoid muscle, 10% recruitment of the left posterior cricoarytenoid muscle, and 30% recruitment of the left cricothyroid muscle. Right vocal fold neuromuscular function was normal.
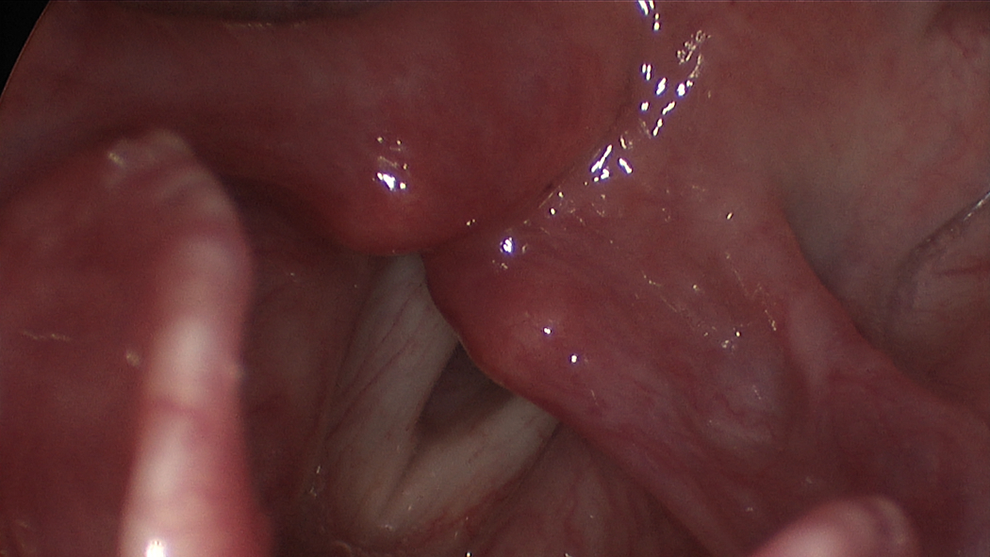
Strobovideolaryngoscopy still from the patient’s initial visit. There is significant erythema and edema of the arytenoids posteriorly, indicative of laryngopharyngeal reflux (LPR). Bowing of the left vocal fold and left arytenoid prolapse is also noted.
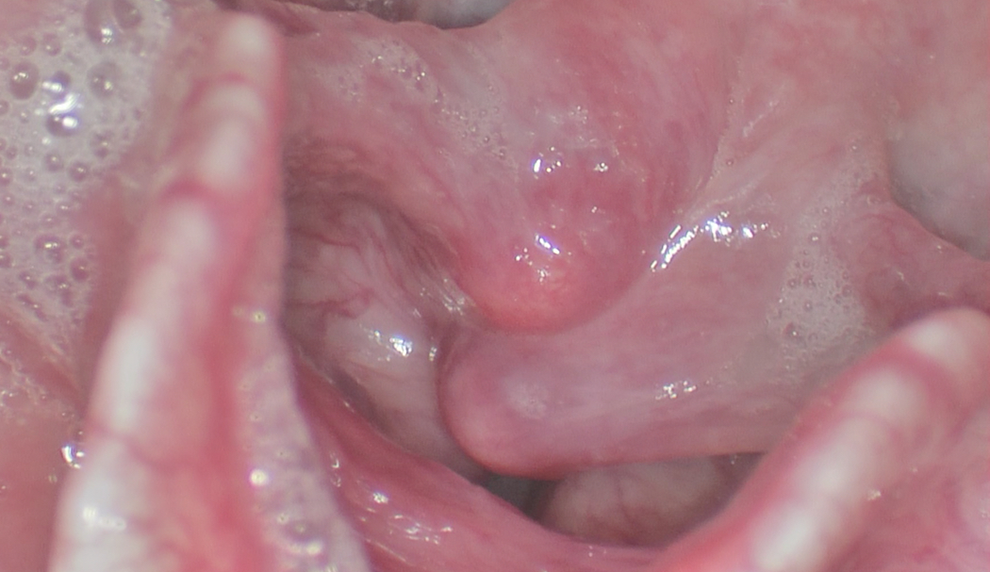
Strobovideolaryngoscopy still from the patient’s second visit, 8 months after the initial visit taken during phonation shows persistent left arytenoid prolapse.

Strobovideolaryngoscopy still from the patient’s second visit taken during inspiration shows left vocal fold bowing. The arytenoids show slightly reduced erythema because of anti-reflux therapy.
The patient underwent voice therapy that improved ease and quality of phonation. Anti-reflux therapy was prescribed. However, he continued to have moderate-to-severe roughness with low fundamental frequency and glottal fry during conversational speech. Surgical options including type I thyroplasty, vocal fold fat injection, and arytenoidopexy were discussed.
Discussion
Colon interposition allows a portion of the colon to replace the esophagus as the conduit for bolus transfer following esophagectomy. 1,2 The colon can have a peristaltic function and creates decreased severity of acid reflux compared to gastric interposition. 3 Complications of colon interposition include graft ischemia, anastomotic leak, dysphagia with or without stricture formation, ulceration due to biliary reflux, graft redundancy, gastrocolic reflux, and others. 4,5 Cense et al assessed quality of life in 14 patients with colon interposition using the San Francisco 36 (SF-36) questionnaire and the Rotterdam Symptom Checklist (RSCL). 6 They reported that patients with colon interposition scored statistically significantly lower in the SF-36 domains of general health, vitality, physical role, social functioning, and mental health when compared with patients with gastric tube reconstruction. Among these patients, the most commonly reported RSCL symptoms were early satiety after a meal, dysphagia, diarrhea, loss of sexual interest, and fatigue. 6
There is a paucity of literature describing the effects of colon interposition on the voice, swallowing, and voice and swallowing-related quality of life. DeMeester noted the possibility of recurrent laryngeal nerve injury during the procedure, with injury more likely to occur on the left side as the nerve is more medial to the esophagus on the left. 5 The vocal fold paralysis noted in our patient might have been due to such injury. The dysphagia, dysmotility, and LPR exhibited in our patient also might have contributed to his voice dysfunction. Future research should focus on categorizing symptoms of dysphonia and optimizing voice outcomes in patients with colon interposition. The rates of LPR and dysphonia in patients with colon interposition, gastric tube reconstruction, and normal esophageal conduits should be compared in order to select the best form of reconstruction for professional voice users.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.