
Abstract
Objectives:
To illustrate some of the common dilemmas in tympanostomy tube care and describe time-tested ways to address them.
Methods:
Computerized literature review.
Results:
Issues including the correct diagnosis of recurrent acute otitis media, tympanostomy tube types and techniques for tube placement, management of tube clogging and otorrhea, and methods for tube removal and patching are illustrated.
Conclusions:
Tympanostomy tube placement is the most common surgery performed in children requiring general anesthesia. While some elements of tympanostomy tube care have been addressed in clinical studies, much of clinical practice is guided by shared experience.
Introduction
Most residents and young otolaryngologists are familiar with the American Academy of Otolaryngology—Head and Neck Surgery, Inc (AAO-HNS) guidelines for tympanostomy tubes and with the mechanics of tube placement in the operating room. This issue of the Ear, Nose, and Throat (ENT) Journal aims to provide advanced knowledge of tympanostomy tube care-based best-evidence, including both clinical studies when available, and expert opinion where high-quality research is lacking.
This article is designed as a photo essay, including images to help guide young otolaryngologists through some of the dilemmas they will encounter during a career of caring for children with tympanostomy tubes. Some of the approaches to tympanostomy tube care described are based on prospective controlled studies. As often, they reflect the collective experiences of pediatric otolaryngologists—especially of those of Charles D. Bluestone and Sylvan E. Stool, to whom the article is dedicated.
What Is Recurrent Acute Otitis Media?
Acute otitis media (AOM) is difficult to diagnosis especially in the young, sometimes uncooperative children most commonly affected by the disease. 1 There is no reliable patient symptom or any single physical sign that assures correct diagnosis. 2 In a feverish, crying child, vascular engorgement can produce the “red eardrum” that might lead a pediatric provider to diagnose AOM and prescribe an antibiotic (Figure 1, video https://www.youtube.com/watch?v=zNv93t4xUJQ).
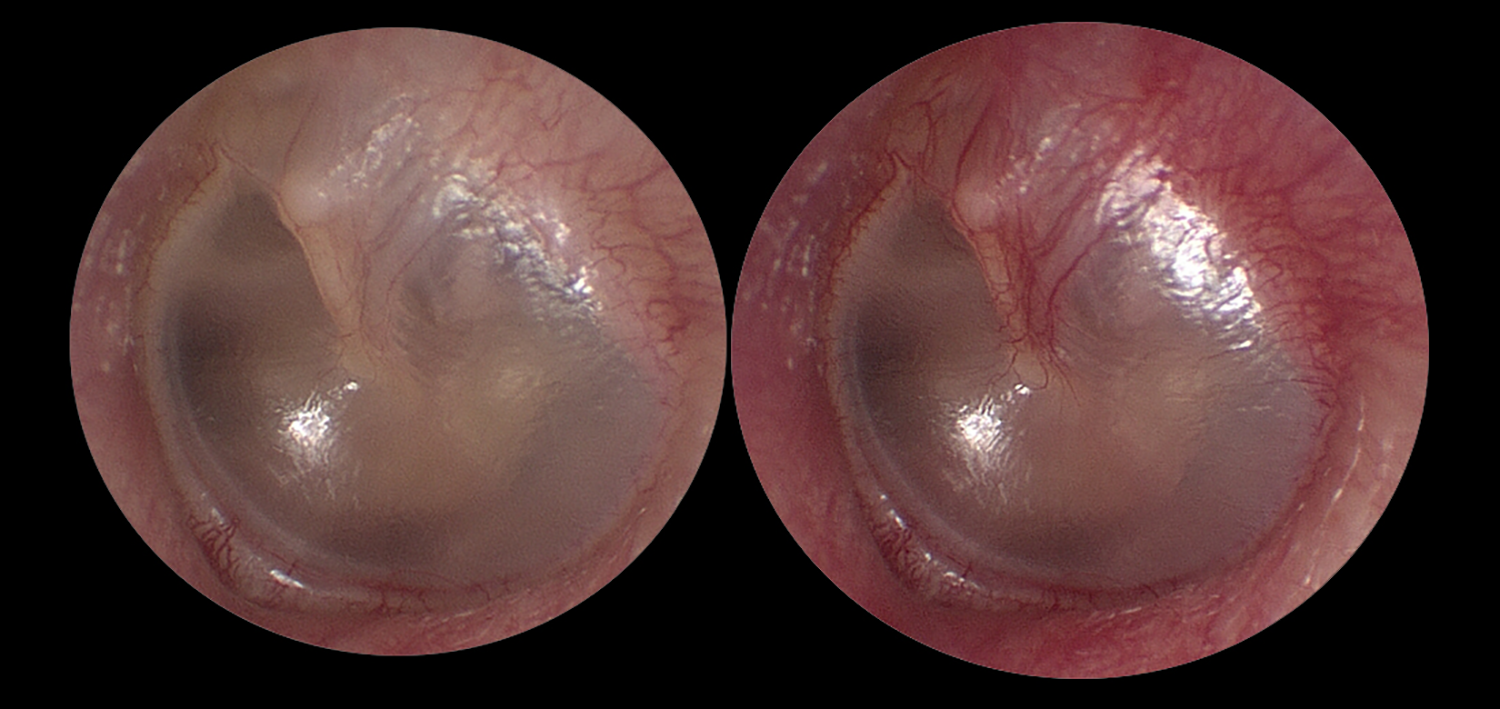
Left tympanic membrane. Left-normal TM. Right-same TM after modified Valsalva with vascular engorgement sparing the pars tensa. TM indicates tympanic membrane.
Concerns about the overdiagnosis and overtreatment of suspected AOM have led to specific changes in society guidelines. The American Academy of Pediatrics 3 requires the presence of a bulging of the tympanic membrane (TM; Figure 2) in its clinical practice guideline specifically to address overtreatment of red eardrums and otitis media with effusion.
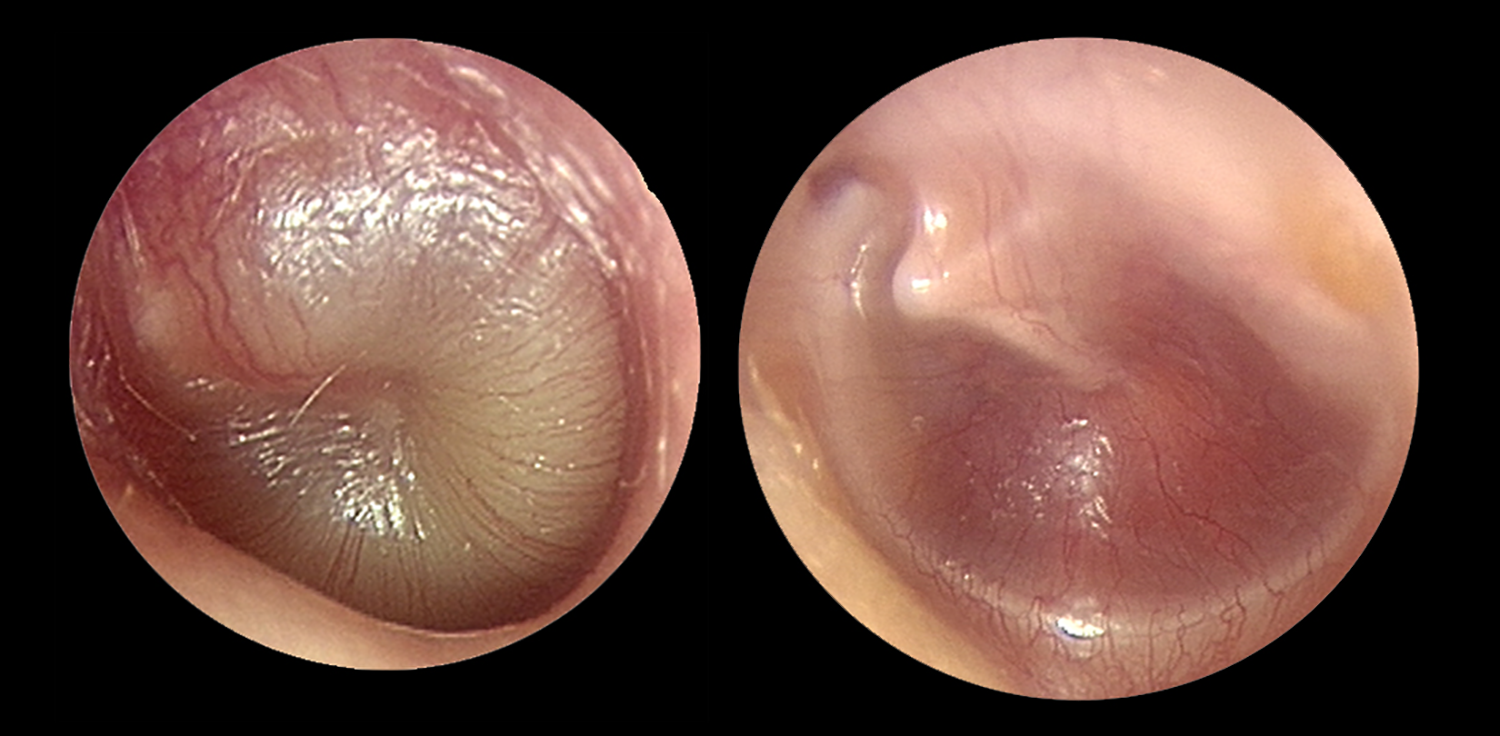
Left, bulging acute otitis media. Right, retracted drum in otitis media with effusion. Both show vascular engorgement involving the pars tensa.
The AAO-HNS guideline on tympanostomy tubes in children recommends deferring tube placement in children who present with normal ears at initial consultation 4 —even when there is a documented history of recurrent AOM. Studies show incomplete adherence to these guidelines. 5 -8 When a child presents with a history of 10 episodes of AOM, has multiple drug allergies, and gastrointestinal symptoms complicating antibiotic use, tympanostomy tubes are often recommended even when middle ear effusion is absent. Noncompliance with guidelines in such a setting is not always wrong. The modest reduction in incidence of AOM with tympanostomy tubes 9 -11 is enhanced by their other positive effects—decreased severity of AOM symptoms, improved diagnosis of AOM (no drainage, no infection), and sparing of systemic antibiotics thanks to effective ototopical treatments. Quality-of-life improvement 12,13 must be weighed against the known risks of surgery and general anesthesia. 14
The Best Tympanostomy Tube/The Best Way to Place It
There are 3 materials (fluoroplastic, silicone elastomer, or metal) and 2 basic designs (short-term, longer-term) used in the majority of tympanostomy tubes. 15,16 Armstrong II, Paparella I, Donaldson, Shepard, Sheehy, and Reuter bobbins are the dominant short-term tympanostomy tubes in the world. They share a grommet design with 2 flanges of varying size separated by a short shaft. The different designs and materials have slightly different rates of occlusion (clogging), infection, duration of function, and rates of persistent perforation after extrusion. 17 -19 None is clearly superior (Figure 3).
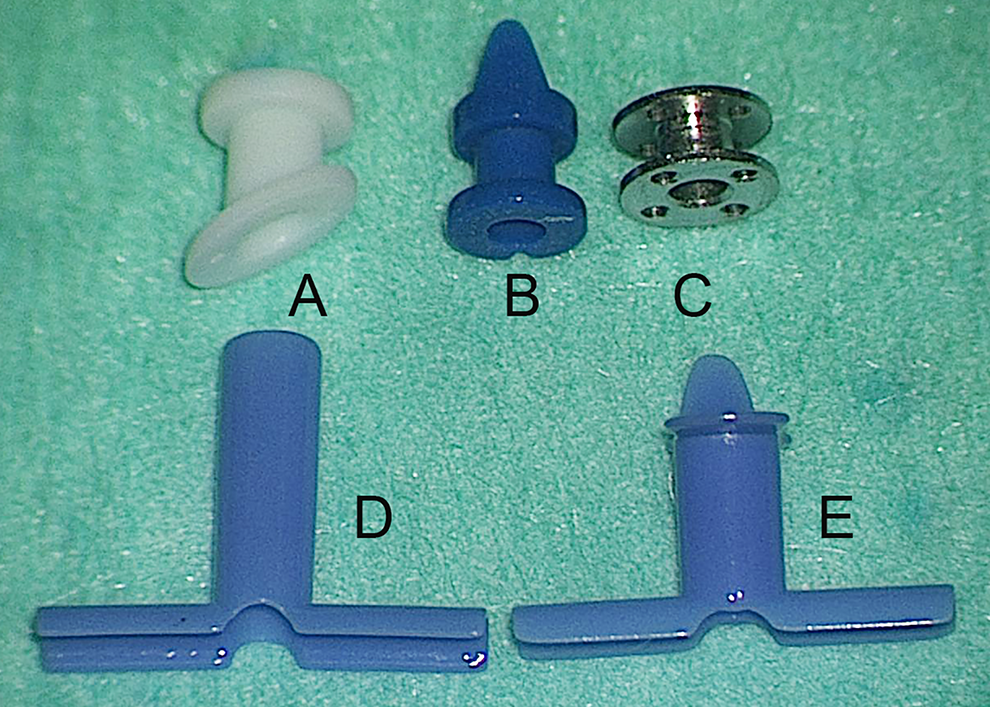
Tympanostomy tubes—first row short-term grommets; second row long-term tubes. A-Armstrong beveled grommet; B-Paparella I grommet; C-Reuter bobbin; D-Goode T-tube; E-butterfly tube.
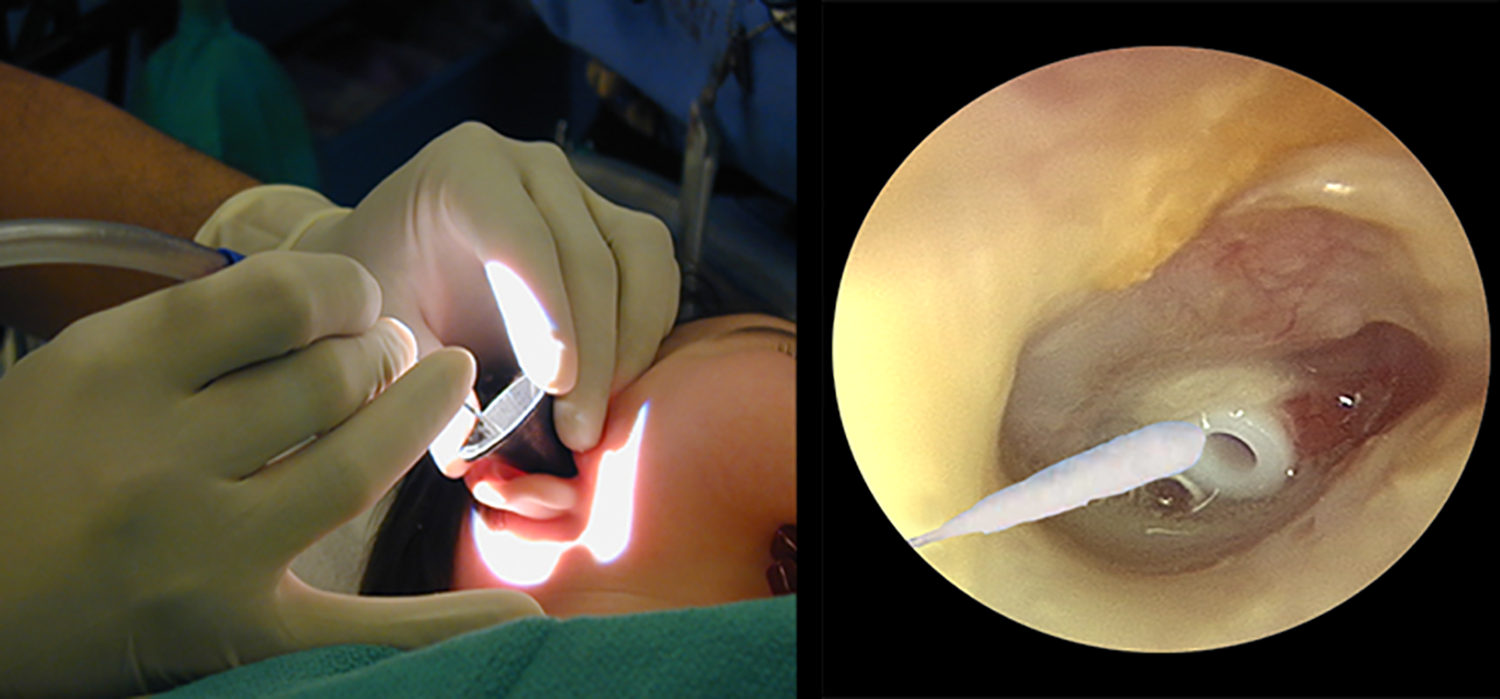
Short-term tubes are usually placed under general anesthesia in young children. They are typically placed through a radial incision in the pars tensa, either anteriorly or posteroinferiorly (to avoid damaging the stapes and incus long process; Figure 4). While different surgeons employ minor technical variations in tube insertion, use of a pick for final tube positioning is associated with low-rates of accidental middle ear insertion. 20 If (when) a tube is partially or completely inserted into the middle ear, do not attempt to remove it with alligator forceps, rather reach past it with a right-angle hook and tease it back into correct position (Figure 5).
Placing a grommet type tube.
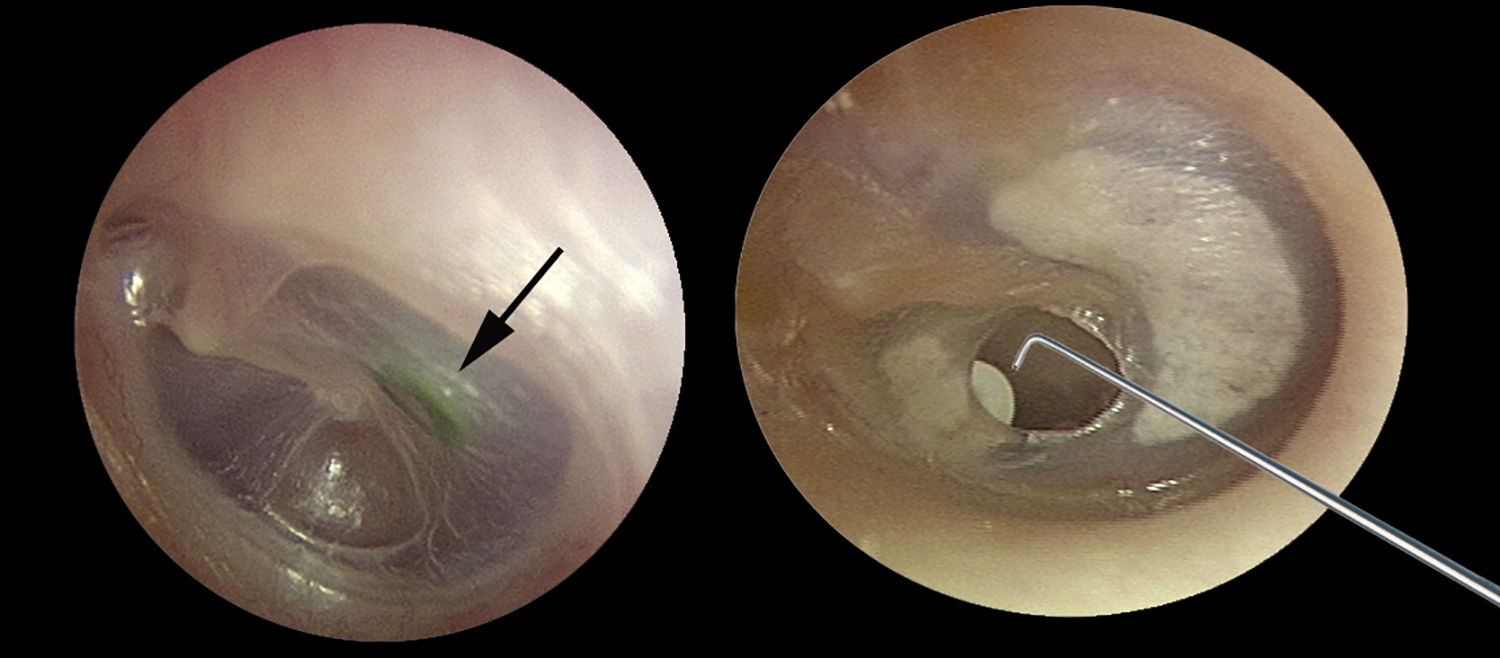
Left, green tube lost in middle ear (arrow); right, recovery of displaced tube with right angle hook.
Grommet tubes typically extrude about a year after placement. Migrating squamous epithelium accumulates under the outer flange of the tube and eventually forces the inner flange through the TM and into the ear canal (Figure 6).
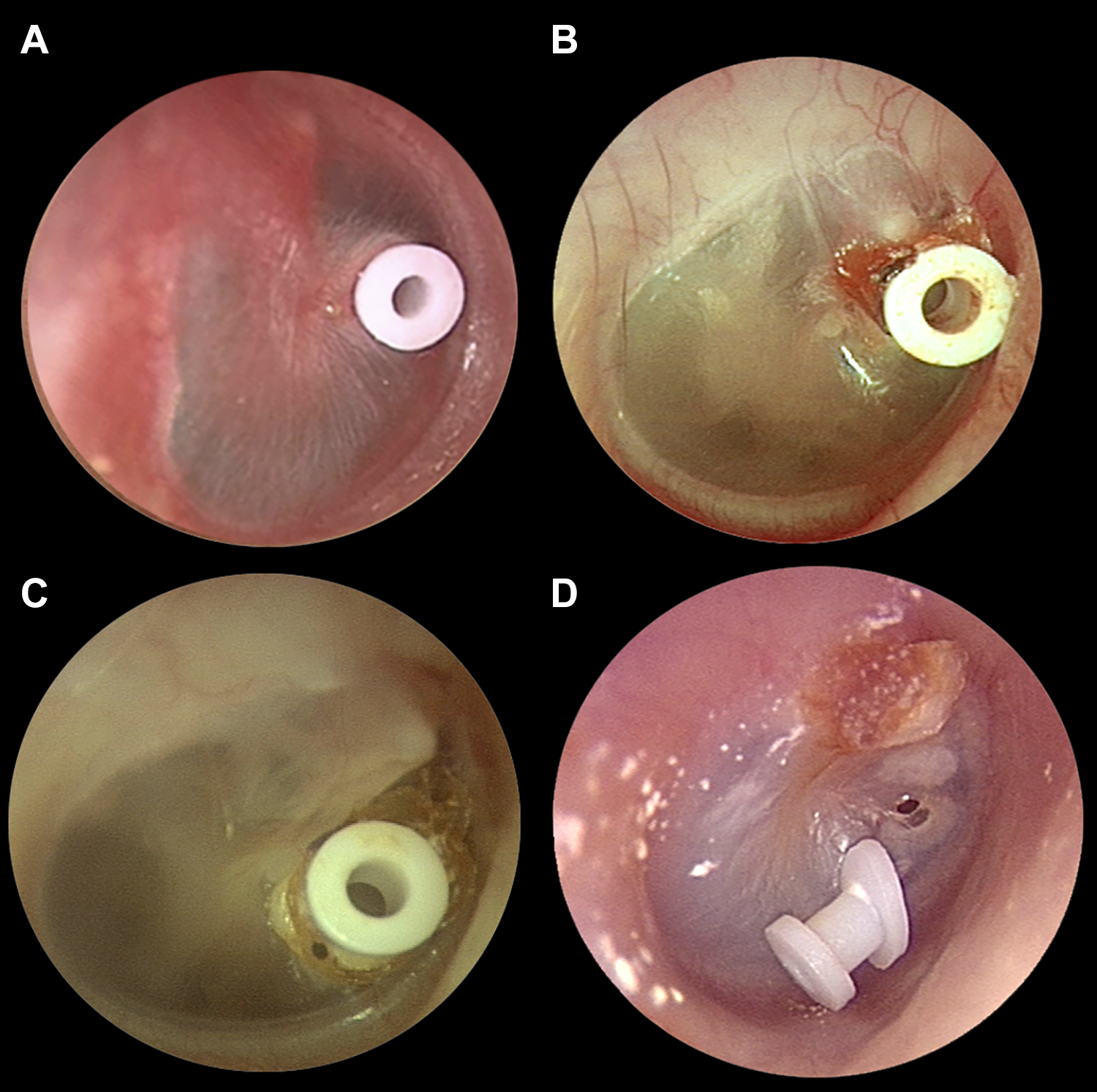
A, Newly placed tube flush to TM; (B) aging tube, lifted by squamous debris; (C) extruding tube with inner flange coming through drum; (D) recently extruded tube with TM perforation closing behind it. TM indicates tympanic membrane.
Long-term tympanostomy tubes resist forces of extrusion with a larger inner flange (Per-Lee, Paparella II), no outer flange (Armstrong I), or both (Goode T-tube). These long-term tubes have higher rates of granulation tissue formation and of nonhealing perforation 21,22 than short-term designs. Long-term tubes are often chosen when short-term tubes have extruded prematurely, or when there is atelectasis or significant retraction of the drum and long-term intubation is desired (Figure 7).
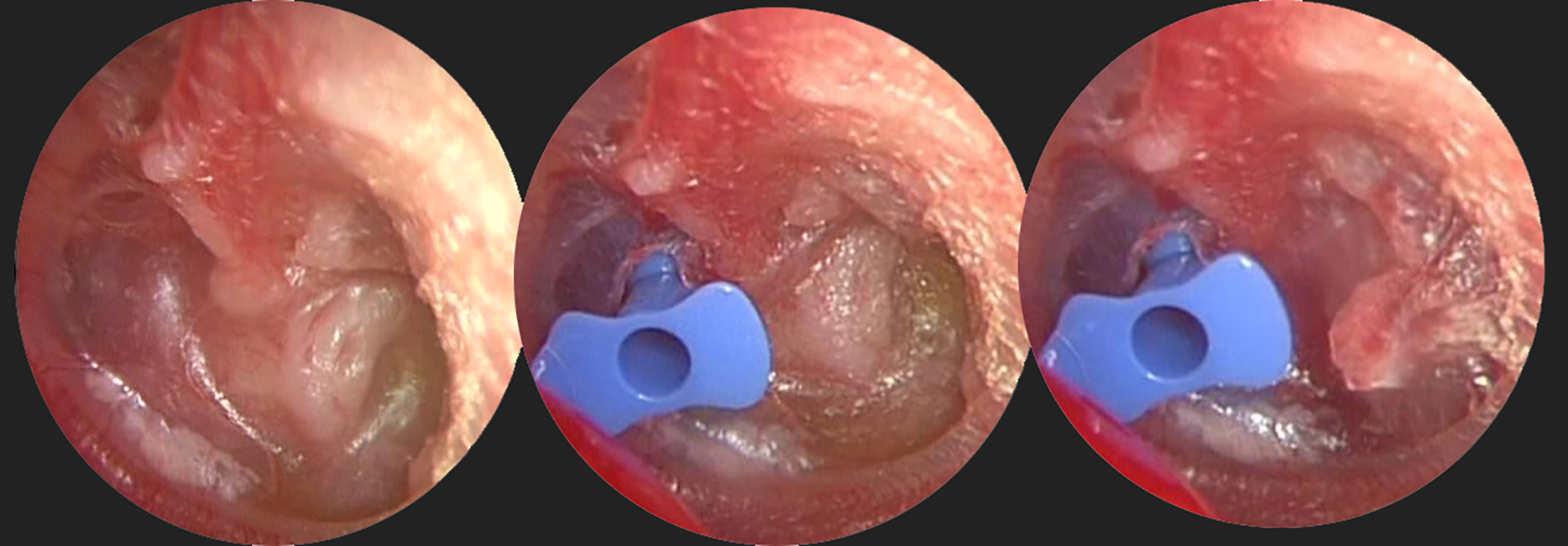
Left, atelectatic drum with middle ear effusion and retraction into the sinus tympani; middle, placement of long-term butterfly tube; right, mechanical reduction of the deep retraction pocket after tube placement.
Tympanostomy Tube Otorrhea
Approaches to the management of tympanostomy tube otorrhea are addressed in detail elsewhere in this issue. Most episodes of acute tympanostomy tube otorrhea can be treated with ototopical drops. There appears to be an advantage to steroid containing drops, especially when granulation tissue surrounds the draining tube (Figure 8).
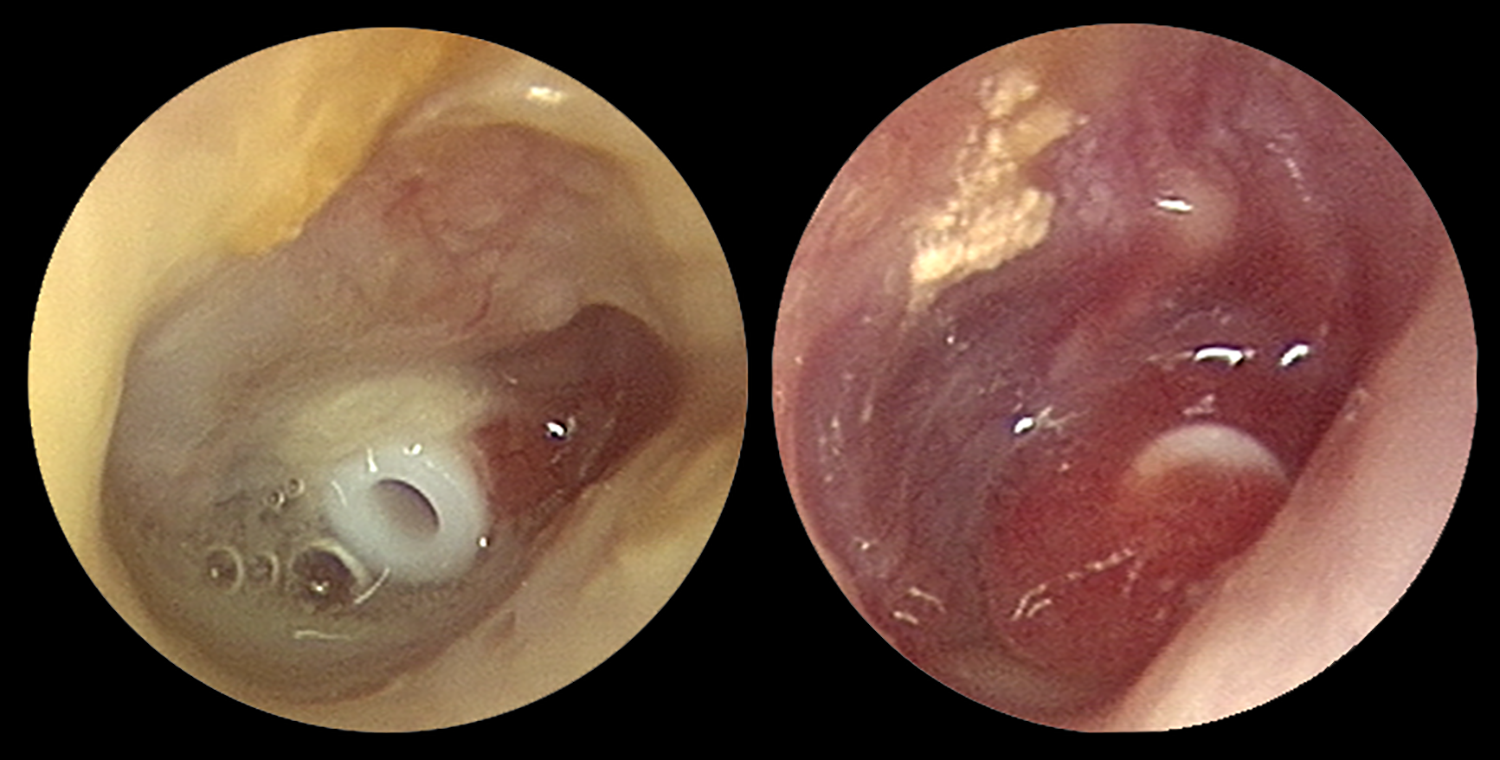
Left, acute tube otorrhea; right, tube otorrhea with granulation.
If otorrhea persists after initial treatment, aural toilette (cleansing of the ear canal with suction) under the operating microscope and culture of the discharge at the tube orifice can help guide subsequent therapy with systemic or topical agents (Figure 9).
Left, aural toilette; right, culturing the tube orifice with a urethral swab.
Tube Clogging
When the lumen of a tympanostomy tube becomes clogged, it renders the tube temporarily ineffective. Clogging can occur immediately after tube placement (especial in ears with effusion at surgery), later following an episode of otorrhea, or as part of the normal extrusion process. Some clogs can be dissolved with ototopical drops 23 or peroxide solutions. 24 Clogs in recently placed tubes (<6-9 months) can be extracted or medial displaced into the middle ear under the operating microscope. Restraint is advisable during this maneuver, completed with a curved pick. Clogs in extruding tubes are not amenable to mechanical removal (Figure 10).
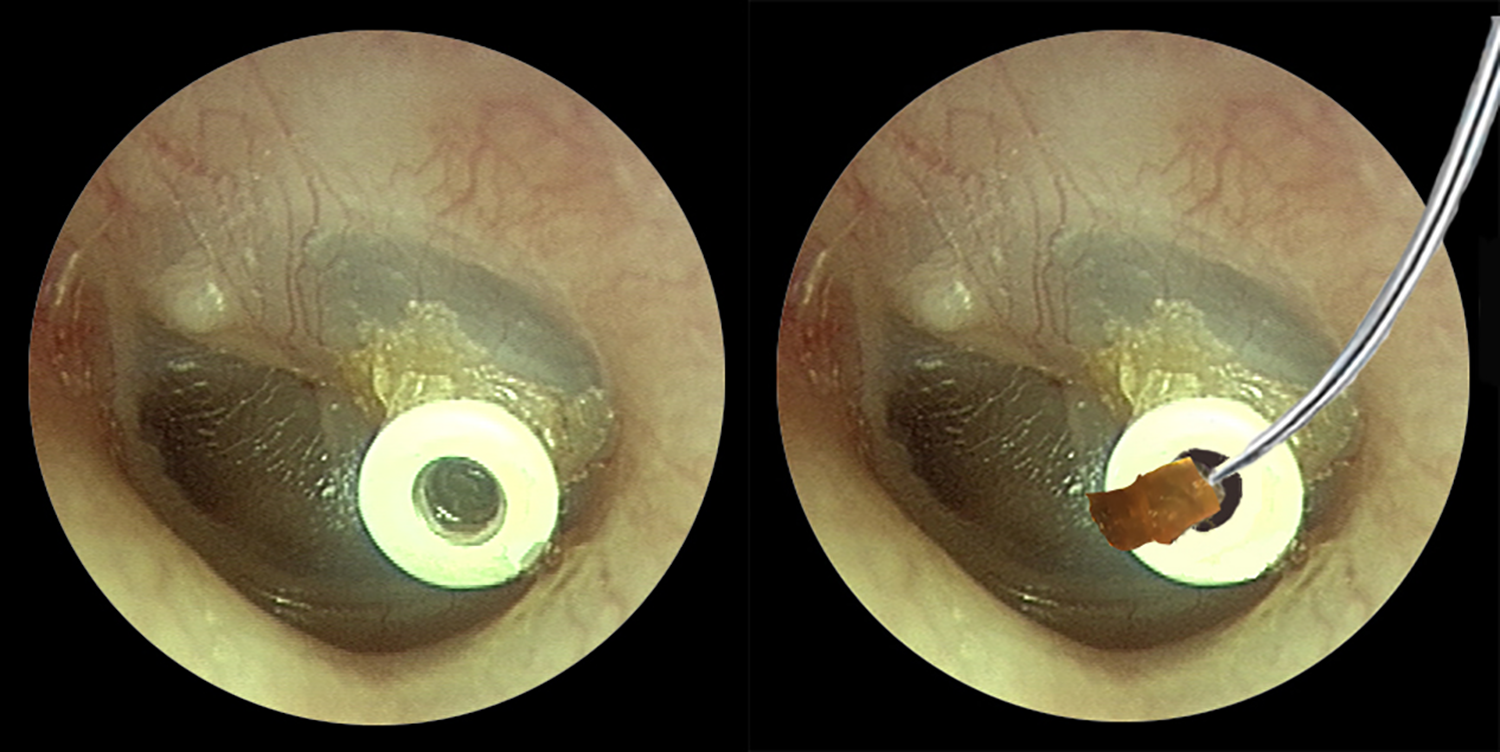
Left, a clogged tube; right the clog can be displaced into the middle ear or, as here, removed like a champagne cork.
Tube Removal
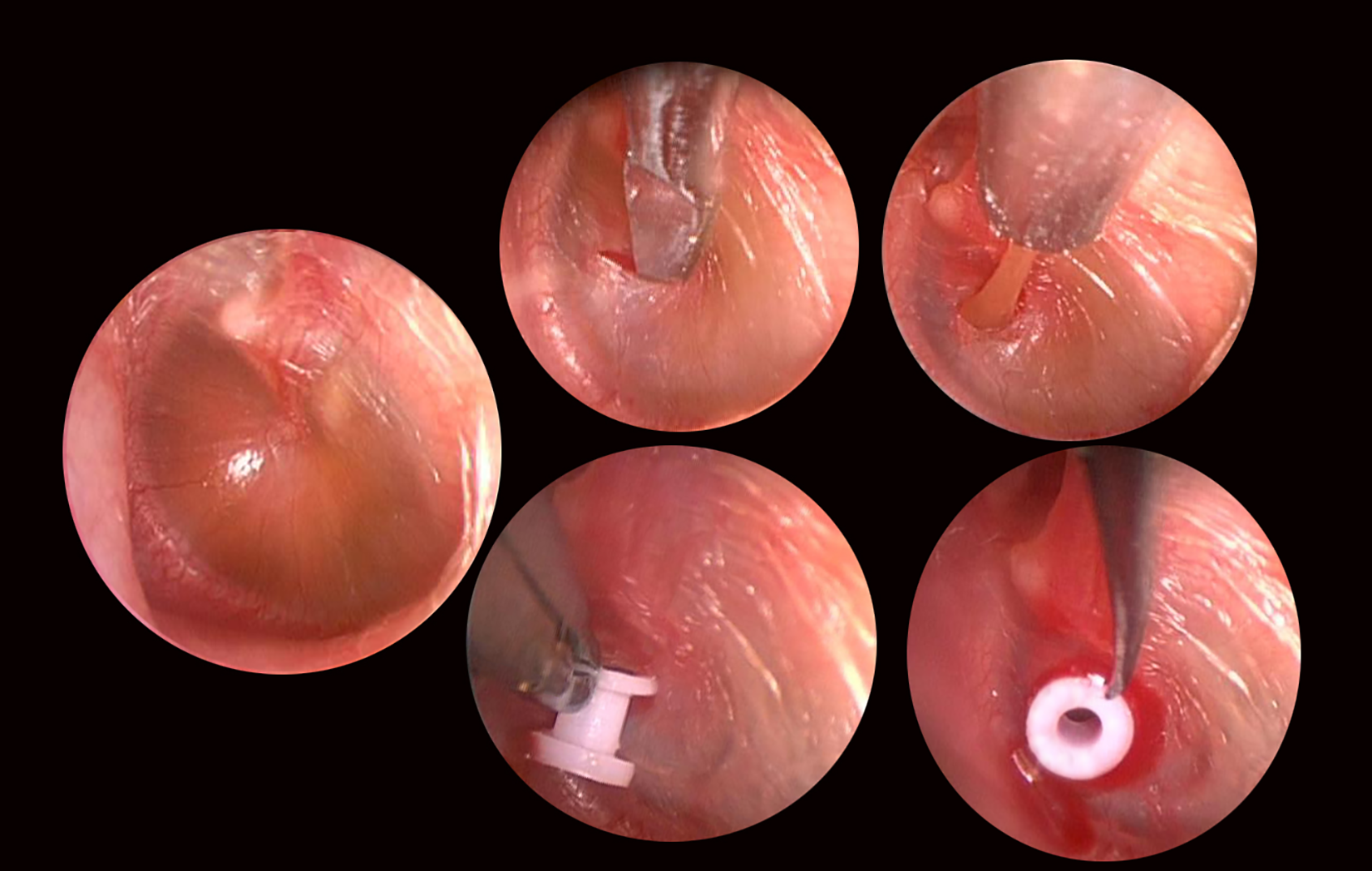
The optimal timing and methods for removal of retained tympanostomy tubes is addressed separately. Patch materials including paper, 25 gelatin film, 26 and porcine acellular submucosa 27 (collagen matrix) are often used after tube removal and freshening of the resultant perforation (Figure 11).
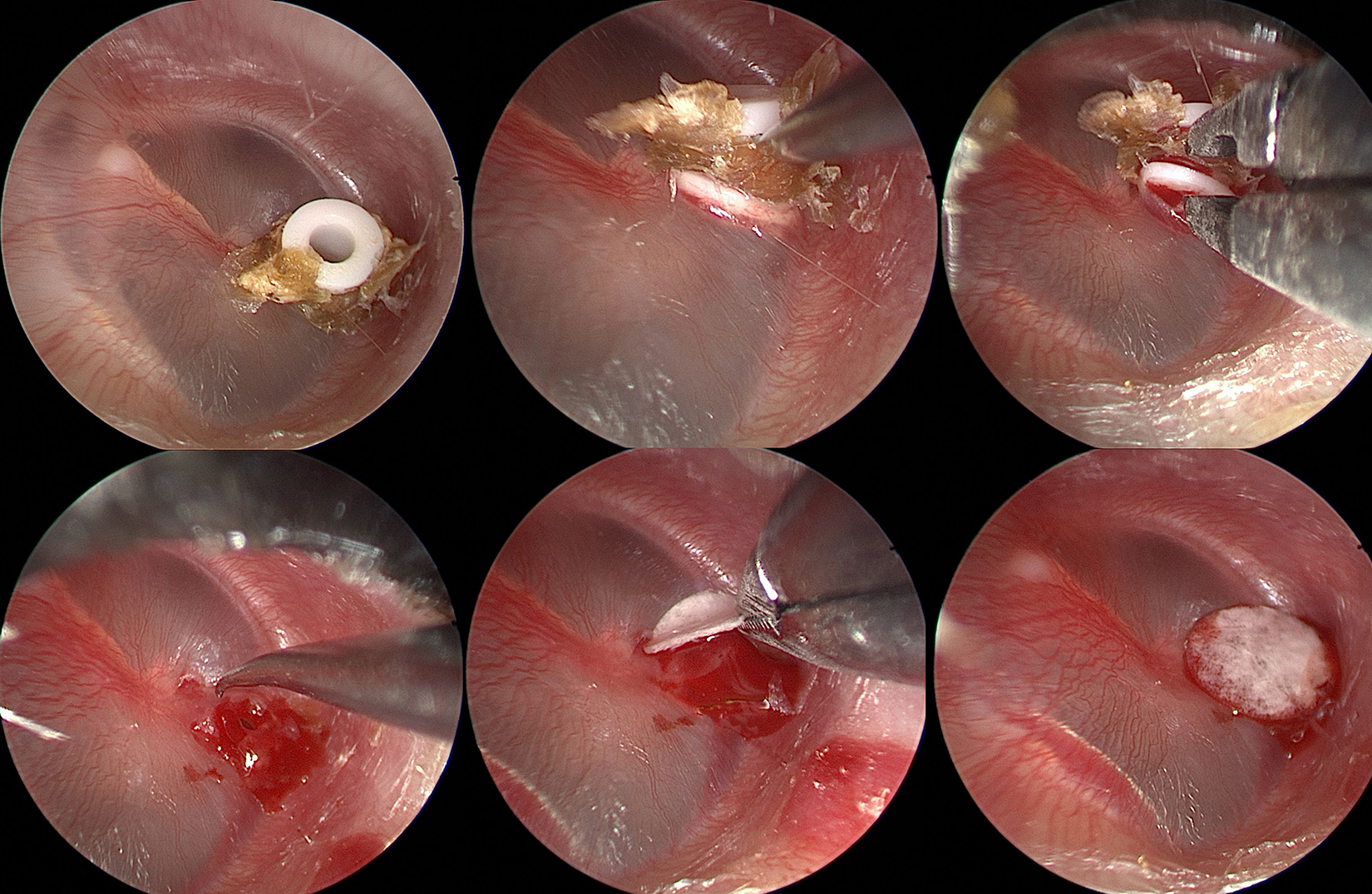
Top left to bottom right—retained tube with squamous debris is elevated with a pick and removed with cup forceps. The resultant perforation is rimmed with a pick and a collagen matrix patch is applied.
Conclusion
Tympanostomy tube placement is the most common surgery performed in children requiring general anesthesia. While some elements of tympanostomy tube care have been addressed in clinical studies, much of clinical practice is guided by shared experience. This article illustrates some of the techniques that have proved effective during years of pediatric otolaryngology practice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.