
Abstract
Objective:
To investigate the coronavirus disease 2019 (COVID-19) status of patients with initial sudden olfactory anosmia (ISOA) through nasopharyngeal swabs for reverse transcription–polymerase chain reaction (RT-PCR) analysis and to explore their olfactory dysfunctions with psychophysical olfactory evaluation.
Methods:
A total of 78 ISOA patients were recruited from April 6, 2020, to April 10, 2020, through a public call of University of Mons (Mons, Belgium). Patients benefited from nasopharyngeal swabs and fulfilled the patient-reported outcome questionnaire. Among them, 46 patients performed psychophysical olfactory evaluation using olfactory identification testing. Based on the duration of the ISOA, 2 groups of patients were compared: patients with olfactory dysfunction duration ≤12 days (group 1) and those with duration >12 days (group 2).
Results:
In group 1, 42 patients (87.5%) had a positive viral load determined by RT-PCR and 6 patients (12.5%) were negative. In group 2, 7 patients (23%) had a positive viral load and 23 patients (77%) were negative. The psychophysical olfactory evaluation reported that anosmia and hyposmia occurred in 24 (52%) and 11 (24%) patients, respectively. Eleven patients were normosmic. The viral load was significantly higher in patients of group 1 compared with those of group 2.
Conclusions:
Coronavirus disease 2019 was detected in a high proportion of ISOA patients, especially over the first 12 days of olfactory dysfunction. Anosmia is an important symptom to consider in the detection of COVID-19 infection.
Introduction
Since the first case of pneumonia related to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), 1 the coronavirus disease 2019 (COVID-19) has spread rapidly worldwide. The first European cases were identified in Italy on January 19, 2020. 2 As of April 4, a total of 237 544 European patients were diagnosed through laboratory testing and 25 616 people died from the COVID-19 infection. 3 Anecdotal observations were rapidly accumulated from many European otolaryngologists that sudden anosmia and dysgeusia would be associated with the COVID-19 infection. Hopkins and Kumar published a letter 4 on behalf of the British Rhinological Society describing “the loss of sense of smell as a marker of COVID-19 infection” and proposed that adults presenting with anosmia should self-isolate for 7 days. 5 Moreover, the authors identified that 16% of patients with a clinical or confirmed COVID-19 diagnosis reported loss of smell as an isolated symptom. 6 Concurrently, the Young Otolaryngologists Group of the International Federation of Otorhinolaryngological Societies (YO-IFOS) conducted the first prospective multicenter epidemiological study investigating the prevalence of smell and taste disorders in patients with COVID-19. The authors reported that 85.6% and 88.0% of patients with a confirmed diagnosis of mild-to-moderate COVID-19 reported olfactory and gustatory dysfunctions, respectively. 7 The olfactory dysfunction appeared before (11.8%), after (65.4%), or at the same time (22.8%) as the appearance of general or otolaryngologic symptoms. Females were significantly more frequently affected by olfactory and gustatory dysfunction than males. 7
As olfactory dysfunction seems to be a key symptom of COVID-19, it would be interesting to study patients with initial sudden onset anosmia to assess the rate of COVID-19 infection. We have used the term “Initial Sudden Onset Anosmia” (ISOA) in place of the “Isolated” that was previously described, 6 as we recognized that patients may present with isolated anosmia at the onset but later develop other symptoms of COVID-19 infection.
The aims of this study are to investigate the COVID-19 status of these patients using nasopharyngeal swabs for reverse transcription–polymerase chain reaction (RT-PCR) analysis and to explore their olfactory dysfunction with psychophysical olfactory tests.
Materials and Methods
The ethics committee of Jules Bordet Institute approved the study protocol (IJB-0M011-3137). Patients were invited to participate and the informed consent was obtained.
Subjects and Setting
Patients with sudden olfactory dysfunction as an isolated symptom, of as the first symptom in association with other otolaryngologic symptoms developed at a later stage, were recruited through a public call of the University of Mons (Mons, Belgium). After evaluation of inclusion and exclusion criteria, they were included in the study and their clinical data collected using a patient-reported outcome questionnaire. The following inclusion criteria were considered: patients presenting sudden olfactory dysfunction at the onset of the COVID-19, patients who are native French-speaker, and patients clinically able to fulfill the questionnaire. The following exclusion criteria were considered: patients with olfactory or gustatory dysfunctions before the COVID-19 epidemic; patients with a history of chronic rhinosinusitis or nasal polyposis; and history of nasal surgery and pregnancy. We defined our population as having an onset of anosmia within the preceding 2 weeks. This threshold was chosen according to a study demonstrating that the viral load was almost absent after 2 weeks. 8 The patient population was divided into 2 groups: group 1 including patients with a duration of olfactory disorder ≤12 days and group 2 with patients with a duration of olfactory disorder >12 days.
Clinical Outcomes
The online patient-reported outcome questionnaire was created with Professional Survey Monkey. Participants could complete the survey only once. The selection of the relevant outcomes of the questionnaire was carried out by the COVID-19 Task Force of YO-IFOS, which includes otolaryngologists from North America, Europe, and Asia. 9 The demographic and clinical outcomes consisted of the assessment of nasal obstruction, rhinorrhea, postnasal drip, throat pain, facial pain, ear pain, dysphagia, and dysgeusia, the latter being defined as the impairment of the following four taste modalities: salty, sweet, bitter, and sour.
Olfactory and Gustatory Outcomes
The olfactory and gustatory questions were based on questions from the smell and taste component of the National Health and Nutrition Examination Survey. 10 This population survey was implemented by the Centers for Disease Control and Prevention to continuously monitor the health of the adult citizens in the United States through a nationally representative sample of 5000 persons yearly. 10 The questions characterized the variation, timing, and associated symptoms of both olfactory and gustatory dysfunctions.
Nasopharyngeal Swabs for RT-PCR
The nasopharyngeal swabs were performed by 2 otolaryngologists (M.K. and S.S.). Specimens were immediately sent to the laboratory LHUB-ULB (Laboratoire Hospitalier Universitaire Bruxelles). The microbiological confirmation of SARS-CoV-2 was performed by RT-PCR. Viral RNA extraction was performed by m2000 mSample Preparation SystemDNA Kit (Abbott) using 1000 µL manually lysed sample (700 µL sample + 800 µL lysis buffer from the kit) eluted in 90-µL elution buffer. A quantitative RT-PCR internal control was added at each extraction, and qRT-PCR was performed using 10 µL of the extracted sample in the RealStar SARS-CoV-2 RT-PCR Kit from Altona-diagnostics with a cutoff set at 40 cycle threshold (Ct).
Psychophysical Olfactory Evaluation
The identification of anosmia, hyposmia, or normosmia was made using the “Sniffin Sticks” test (Medisense). Sniffin tests are validated olfactory identification tests to evaluate the olfactory performance of patients. 11 A total of 16 pens were presented to the patient at 30-second intervals. The patient had to characterize the smell by choosing 1 of 4 options. The test was scored out of a total of 16 points and was categorized into 3 groups: normosmia (score between 12 and 16), hyposmia (score between 9 and 11), and anosmia (score 8 or below). Tests were performed on the same day as completion of patient-rated olfactory and gustatory outcomes.
Statistical Analyses
Statistical analyses were performed using the Statistical Package for the Social Sciences for Windows (SPSS version 22.0; IBM Corp). The relationship between Ct (inversely reflecting viral load) and the duration of olfactory dysfunction was assessed by Spearman rho test. A level of significance of P < .05 was used.
Results
A total of 78 patients with sudden olfactory dysfunction as an isolated symptom, or as the first symptom followed by associated otolaryngologic symptoms at a later stage, completed the study. Table 1 describes the demographic and epidemiological characteristics of patients. The mean age of patients was 40.6 ± 11.2 years (21-67). There were 46 (59%) females and 32 (41%) males. The following ethnicities composed the cohort: Caucasian 73 (93.6%), North African 4 (5.1%), and Sino-African 1 (1.3%). The most prevalent comorbidities of patients were gastroesophageal reflux disease (11.5%), allergic rhinitis (9%), asthma (5%), and hypertension (5%). Overall, 86% of patients were nonsmokers.
Demographic and Epidemiological Characteristics of ISOA Patients.a
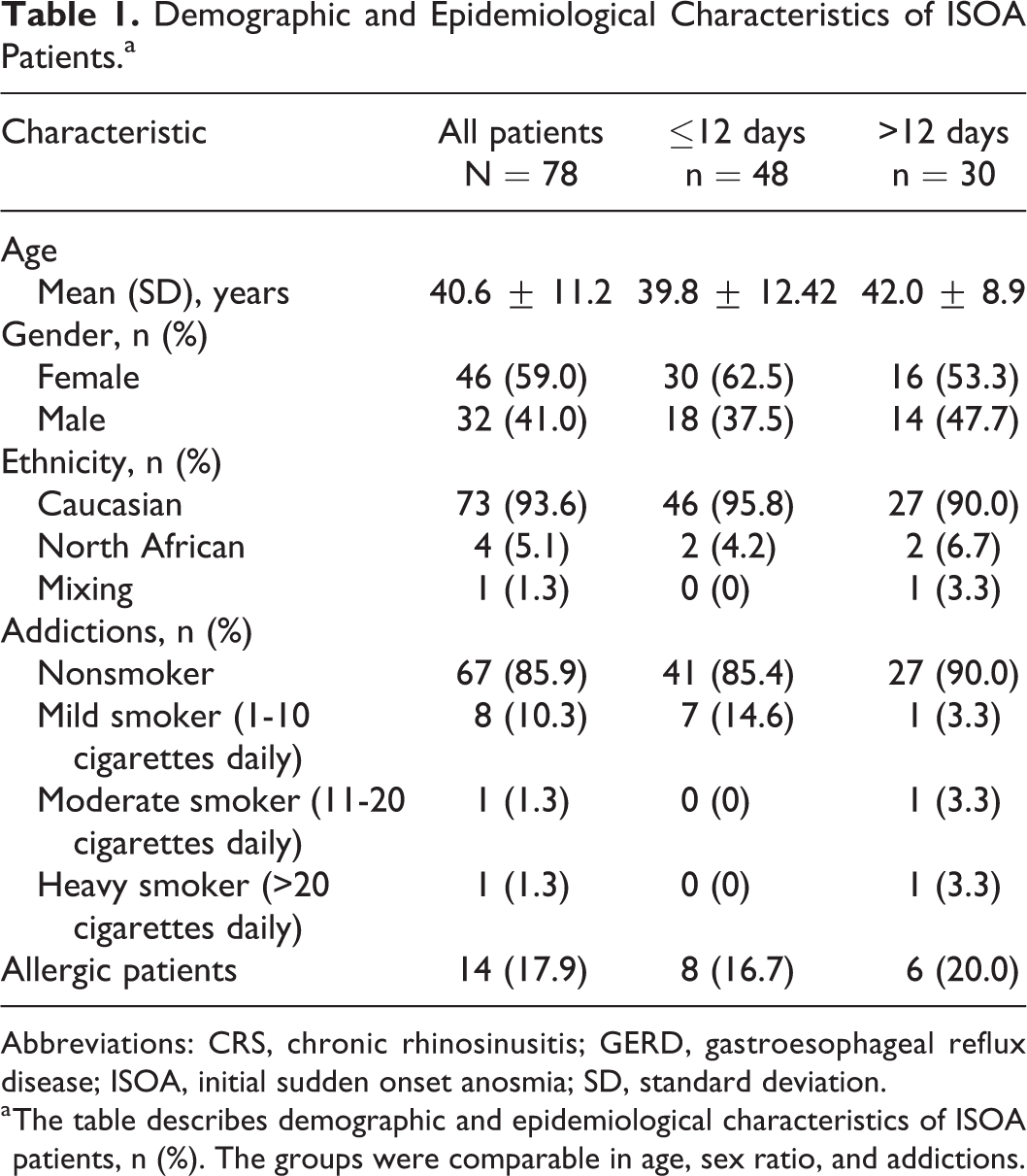
Abbreviations: CRS, chronic rhinosinusitis; GERD, gastroesophageal reflux disease; ISOA, initial sudden onset anosmia; SD, standard deviation.
a The table describes demographic and epidemiological characteristics of ISOA patients, n (%). The groups were comparable in age, sex ratio, and addictions.
Clinical Outcomes
The additional otolaryngologic complaints are described in Table 2. The most prevalent otolaryngologic symptoms occurring throughout the clinical course of the disease were: dysgeusia (67.9%), postnasal drip (46.2%), and nasal obstruction (46.2%). A total of 35 patients (44.9%) presented sudden olfactory dysfunction without nasal obstruction or rhinorrhea. Cacosmia and phantosmia were reported by 57 (73.1%) and 38 (48.7%) patients, respectively. The aroma perception was reduced (n = 18), disappeared (n = 29), or distorted (n = 5) in 23.1%, 37.2%, and 6.4%, respectively.
Ear, Nose, and Throat Symptoms in ISOA Patients.a
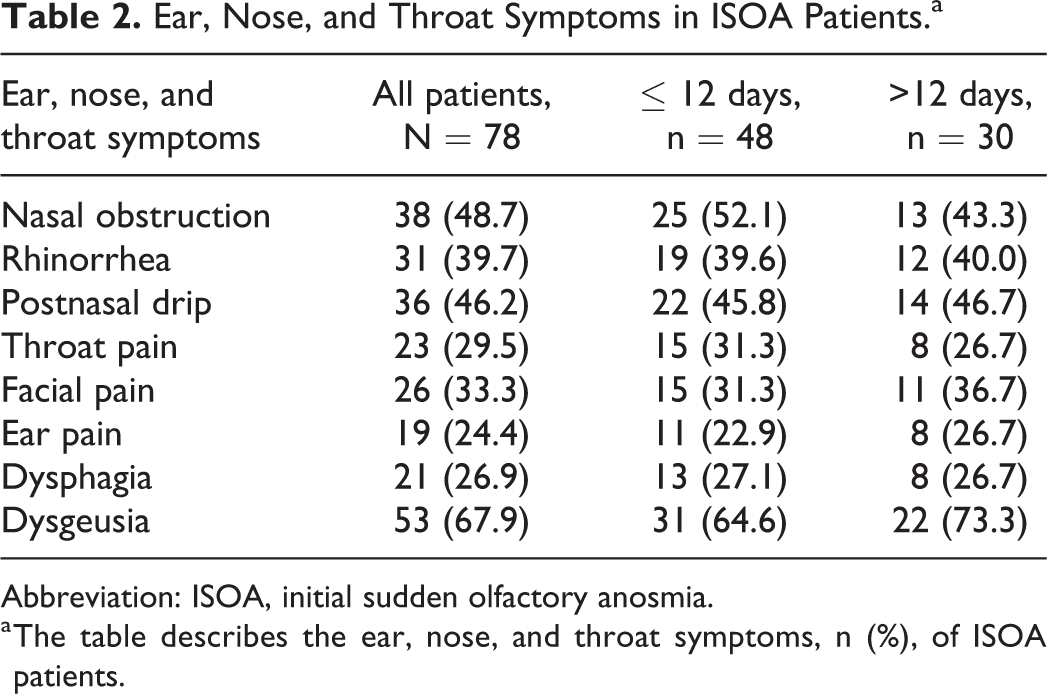
Abbreviation: ISOA, initial sudden olfactory anosmia.
a The table describes the ear, nose, and throat symptoms, n (%), of ISOA patients.
Coronavirus Disease 2019 RT-PCR Positivity and ISOA Patients
Among group 1 (anosmia ≤12 days), 42 patients (87.5%) had a positive viral load determined by RT-PCR while 6 patients (12.5%) were negative. In group 2 (anosmia >12 days), 7 patients (23%) had a positive viral load and 23 patients (77%) were negative.
The viral load level was correlated with the duration of the olfactory dysfunction (rs = 0.441, P = .004; Figure 1). As the Ct is inversely correlated with the viral load, Figure 1 shows that the viral loads are higher during the first days after the onset of anosmia.
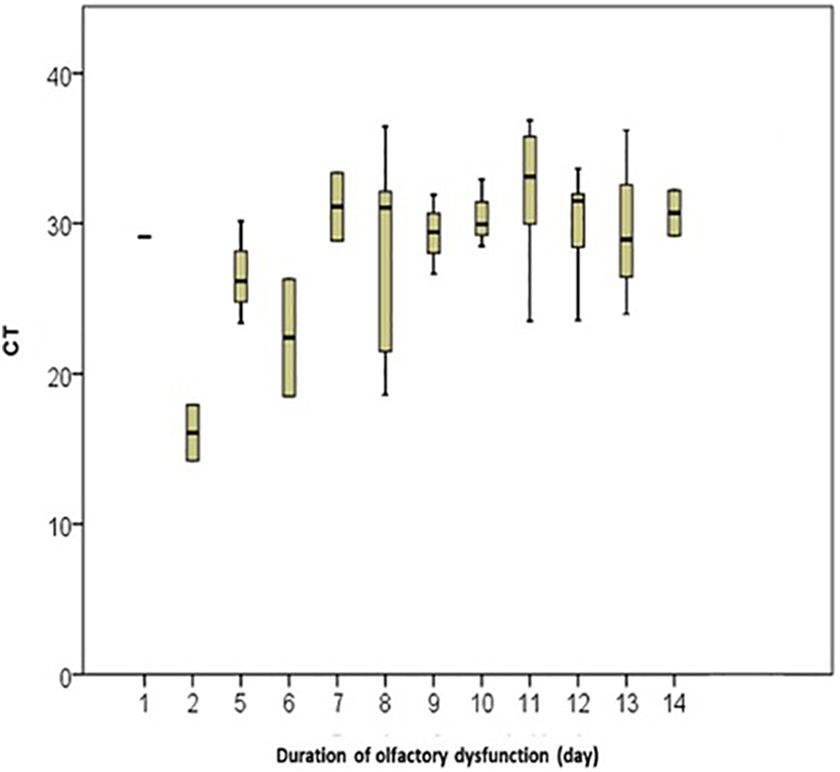
Duration of olfactory dysfunction in relationship with the cycle threshold. Shows the cycle threshold, which reflects inversely the viral load, of our patients according to the onset of the olfactory dysfunction.
Psychophysical Olfactory Evaluation and ISOA Patients
Due to restrictions on movement (lockdown) and the risk of contamination, only 46 patients realized psychophysical assessment. Overall, 24 (52%) and 11 (24%) patients were anosmic and hyposmic, respectively. Eleven (24%) patients were normosmic.
Among the 48 patients of group 1, 21 patients with positive RT-PCR performed the olfactory identification testing: 11 were anosmic (52%), 4 were hyposmic (19%), and 6 were normosmic (29%). Among the 4 patients with a negative RT-PCR, 2 were anosmic, 1 hyposmic, and 1 normosmic. Among the 30 patients of group 2, 7 patients with positive RT-PCR performed an olfactory identification testing: 3 were anosmic (43%), 3 hyposmic (43%), and 1 patients normosmic (6%).
Discussion
According to testimonies from Britain, the United States, France, South Korea, China, Germany, and Iran, the occurrence of olfactory dysfunction in patients with COVID-19 is no doubt. The main finding of this study is the confirmation that COVID-19 infection has to be considered in patients with ISOA. The diagnosis was confirmed in 87.5% of patients with recent onset olfactory dysfunction (≤12 days) and the probability to get a positive result at the RT-PCR significantly decreased throughout the clinical course of the disease.
The results of the present study and those of smaller cohort studies 5,6 support that the ISOA should be considered as an important symptom associated with COVID-19. The key role of olfactory dysfunction in the clinical presentation of patients with mild-to-moderate COVID-19 was recently strengthened through a Bayesian analysis conducted in a cohort of 1420 European patients. 12 In this multicenter study, 70.2% of patients had a total loss of smell without a significant prevalence of nasal obstruction or rhinorrhea in the subgroup of patients with olfactory impairment. Our data suggest that it is beneficial to perform diagnostic swabs in the first 12 days of the ISOA to avoid the risk of a false-negative result as the viral load is reduced. However, this finding has to be confirmed in patients benefiting from repeated swabs over the clinical course of the disease.
Second, we observed that 76% of patients self-reporting total loss of smell had anosmia or hyposmia. The proportion of anosmic patients decreased to 43% in the group with a longer ISOA (>12 days). The majority of patients did not report nasal obstruction or rhinorrhea, which are both factors that may lead to olfactory dysfunction. Indeed, in the study of Akerlund et al, the impairment of psychophysical olfactory evaluations were significantly correlated with nasal obstruction (rhinometry). 13 Interestingly, in this experimental study, authors used a coronavirus to induce the rhinitis and the related nasal obstruction. Based on the results of Akerlund et al, we basically believed that the nasal obstruction related to the viral inflammation led to the anosmia. However, we did not observe a high prevalence of nasal obstruction or rhinorrhea in our cohort. This lack of nasal symptoms strengthens the neural hypothesis of anosmia, consisting of a virus spread through the olfactory neuroepithelium and injuries of glial or neural cells of the olfactory bulb. In 2007, Suzuki et al demonstrated that some coronaviruses may be responsible for neurological anosmia. 14 Recently, Netland et al observed in a transgenic mice model that SARS-CoV may spread to the brain through the olfactory bulb, leading to rapid transneuronal spread. 15 We also observed that our European patients with ISOA often complained from nasal burning at the onset of the disease, before the development of olfactory dysfunction. The nasal burning could be related to the spread of the virus through the trigeminal nerve. From there, the virus could potentially reach the gustatory fibers (cranial nerves VII, IX, and X), which are located in the brain stem. Further research is needed to confirm the neural hypothesis underlying the development of olfactory and gustatory dysfunction.
It is interesting to note that 24% of patients were found to have a normal olfactory function on testing. It is known that patients may have some difficulties to rate their own sense of smell 16 especially if they have other otolaryngologic disorders. This needs further evaluation in future studies.
This study has several limitations. First, the sample size was limited. Second, the patients were included at different time points during the course of the disease, and it is conceivable that some of them progressively recovered olfaction from the onset of the disease to the time of assessment. Future studies would ideally study patients at the onset of the disease and assess evolution olfactory function throughout the clinical course.
Conclusions
The results of this study may suggest that COVID-19 is a potential diagnosis to consider in the patient with sudden onset anosmia, regardless of the other coexisting ear, nose, and throat symptomatology. Considering the fact that the viral load decreases significantly during the first 15 days, it seems beneficial to perform the nasopharyngeal swab as soon as possible. Future clinical and experimental research is needed to better understand the pathophysiological mechanisms underlying the development of olfactory dysfunction in patients with COVID-19.
Footnotes
Authors’ Note
J. R. Lechien and P. Cabaraux have equally contributed to this work and should be regarded as joint first authors. S.S and J.R.L. initiated, designed the project, and developed the methods. S.S, J.R.L, C.H. wrote the manuscript. J.P, S.H, C.C.E, C.C.H, D.M. read, corrected, and commented on the manuscript. S.S., M.K., and P.C. performed the experiments. D.M. performed the RT-PCR analysis. S.S, J.R.L, and C.H. analyzed the results. C.H., J.P., and S.H. supervised the project. All authors read and approved the final manuscript.
Acknowledgments
The University of Mons head and the “call center” staff coordinated by Ahmed Cherifi and the following collaborators and researchers: Philippe Boelpaep, Anne Trelcat, Geradine Descamps, Sonia Furguelese, Laura Soumoy, and Fabrice Journe.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Received financial support from the University of Mons (UMONS) as well as FRMH grant.