
Abstract
Myxoma is a benign myxoid tumor of connective tissue that develops primarily in the heart. At the level of the external auditory canal, it is extremely rare. It can be isolated or associated with Carney syndrome. Only 5 cases of isolated myxoma of the external auditory canal have been reported in the literature. We present the case of a 53-year-old patient who consulted for a hearing loss that has been evolving for 3 years. Otoscopy revealed a mass filling the external auditory canal. The scan showed a total filling of the external auditory canal with a homogenous sessile neoformation of 20 × 10 mm. This mass was completely resected and the histological examination showed spindle-shaped and star-shaped cells against an abundant myxoid background, which was consistent with myxoma. All the tests, done to eliminate Carney syndrome, did not reveal any abnormalities. The postoperative course was favorable, and no complications were noted. The patient was under follow-up. There was no recurrence 1 year after surgery.
Introduction
Myxoma is a myxoid tumor of the primitive connective tissue, involving, generally, the heart and other soft tissues. First described in 1871 by Virchow and with histopathologic diagnostic criteria established in 1948 by Stout, it is a lesion that is predominantly comprised of a mucinous substance similar to that seen within the umbilical cord. 1
In the head and neck, it is an uncommon entity that presents most commonly in the maxillofacial bones; it is even rarer in the temporal bone. Isolated myxoma rarely involved the external auditory canal and could not be grossly distinguished from other benign neoplasms or cutaneous cysts.
The exact diagnosis is very important because myxoma of the external auditory canal has been reported as a presentation of Carney complex, which is an autosomal dominant syndrome that is associated with spotty skin pigmentation, endocrinopathy, and endocrine and nonendocrine tumors. Only 5 cases of isolated myxoma of the external auditory canal have been reported in English literature.2-5 We present a case of myxoma in the external auditory canal.
Case Report
A 53-year-old woman with no pathological history consulted for right-sided deafness with progressive worsening associated with ipsilateral tinnitus. The beginning of this symptomatology goes back to 3 years before her first consultation. The patient reported the recent onset of an intermittent right otalgia. There was no otorrhea or vertigo. Otoscopy showed a straight, normal-looking ear pinna, and the external auditory canal was filled with a smooth-surfaced and smooth-skinned tumor. Its consistency was soft. This tumor completely obstructed the lumen of the external auditory canal, making the vision of the eardrum impossible. The insertion of this neoformation was difficult to specify by otoscopy alone. There was no otorrhea, and the left ear was healthy. Following this physical examination, a lipoma or epidermoid cyst of the external auditory canal was suspected.
The audiogram showed a right transmission deafness of 40 db. The hearing on the left side was normal. The scan of the temporal bone showed a total filling of the external auditory canal with a homogenous sessile neoformation of 20 × 10 mm, arising from its posterior superior wall. It extends from the external auditory meatus to the tympanum which it represses from within. There was no bone lysis of the walls of the external duct, and the middle and inner ear were normal (Figure 1).
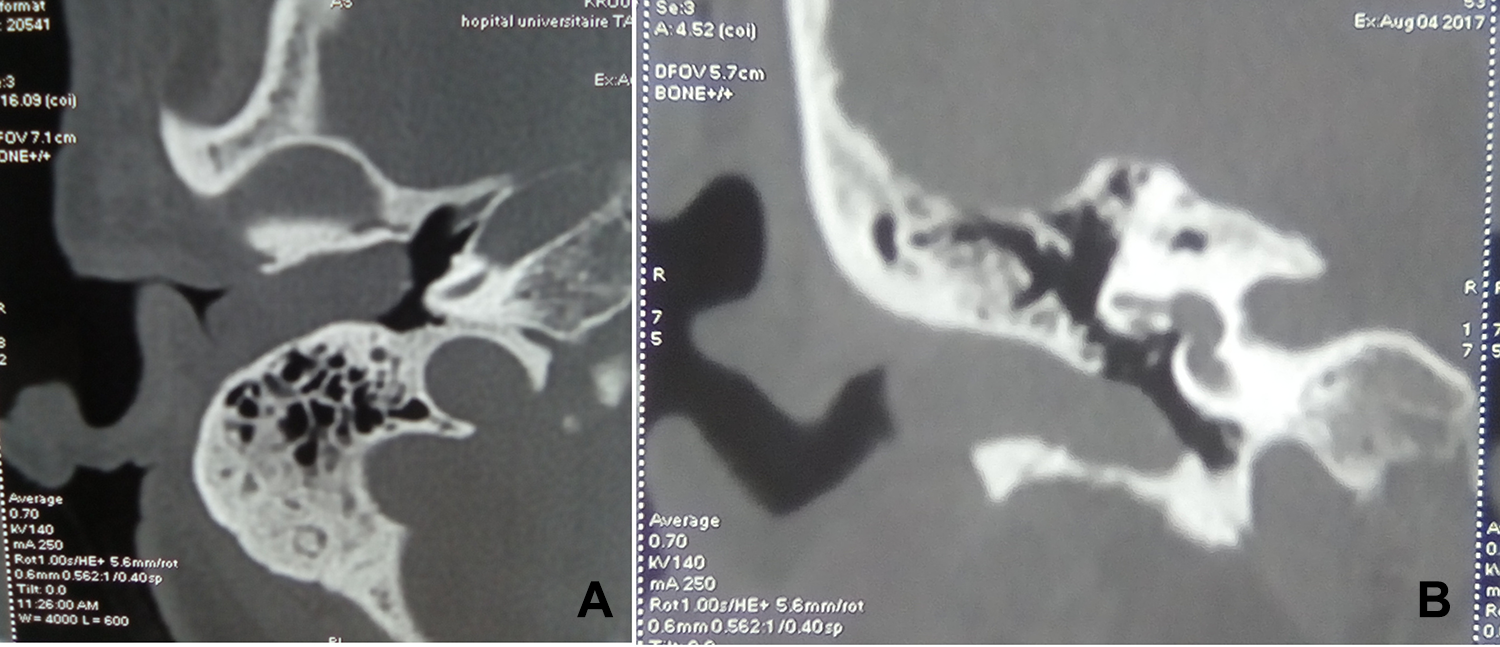
Axial view (A) and coronal view (B) of a computed tomography scan of the right temporal bone showing a homogenous sessile neoformation which extends from the external auditory meatus to the tympanum without bone lysis.
The patient underwent general anesthesia with a retro-auricular approach. The skin of the duct was peeled off, and the tumor was exposed. Therefore, the latter rested on the posterior wall of the external auditory canal.
The tumor was not very hemorrhagic and did not expand to the middle ear. There was no bone lysis. The gradual dissection was made easily until the total excision of the tumor. Then, a small loss of cutaneous substance was covered by Surgicel.
Grossly, the surgical pathology specimen consisted of regularly shaped fragments of soft tissue. Microscopically, the specimen revealed hypocellular benign tumor. It was made by stellate and spindle cells with nonatypical nuclei and no mitosis on an abundant myxoid matrix rich in blood capillaries (Figure 2). The histological findings were compatible with the diagnosis of myxoma.
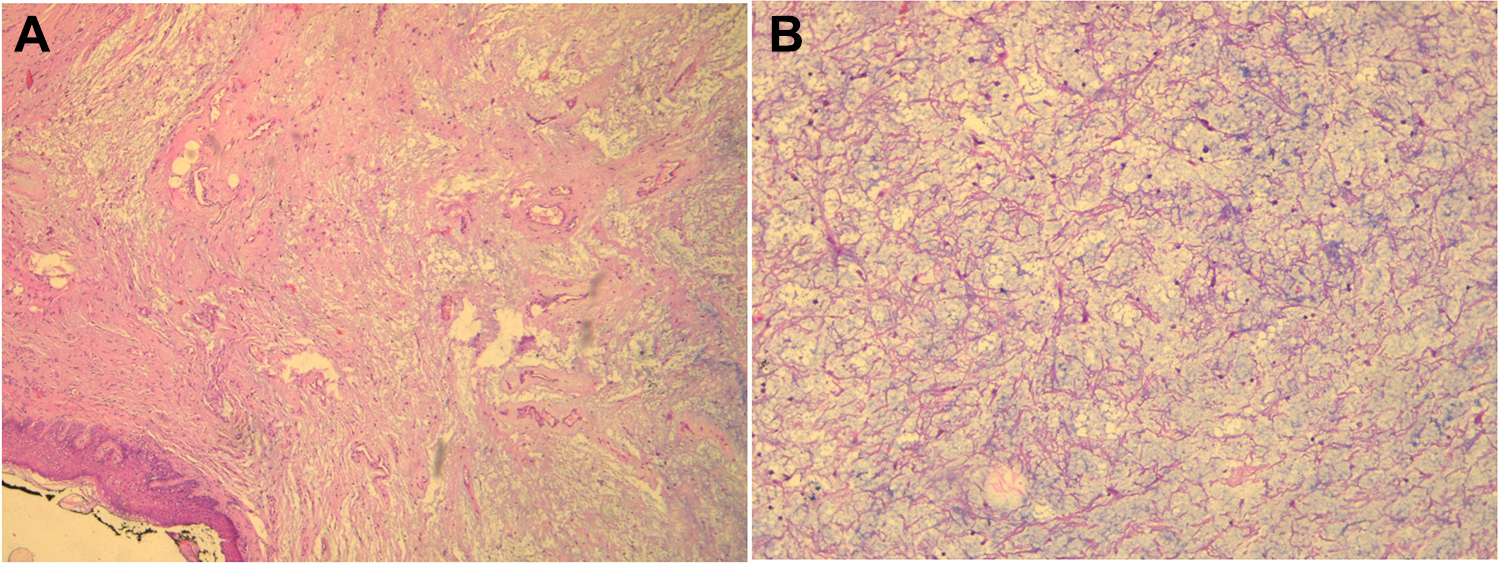
(A) Histological examination revealed a well limited and myxoid tumor (40× HE). (B) High power view showing stellate and spindle cells on an abundant myxoid matrix (100× HE).
Dermatological, cardiological, and endocrinological examinations, done to eliminate Carney syndrome, did not reveal any abnormalities. The postoperative course was favorable. No complications were noted and the patient improved his hearing threshold. There was no recurrence 1 year after surgery.
Discussion
A myxoma is a benign tumor that originates in mesenchymal tissue. Most of these tumors are found in the heart, skin, and subcutaneous and aponeurotic tissues in certain bones.
In 1948, Stout was the first author who defined myxoma as a true benign tumor that is composed of stellate cells that are set in a loose mucoid stroma through which course very delicate reticulin fibers in various directions. 1 In the head and neck, the myxoma lies mainly in the mandible, the maxillary bone, and the oral cavity.3,4,6 Myxomas, as well as those tumors with mixed chondral elements (chondromyxoma, chondromyxoid fibroma), have also been observed within the temporal bone and middle ear.
Review of Previously Reported Cases of Myxoma of the External Auditory Canal.
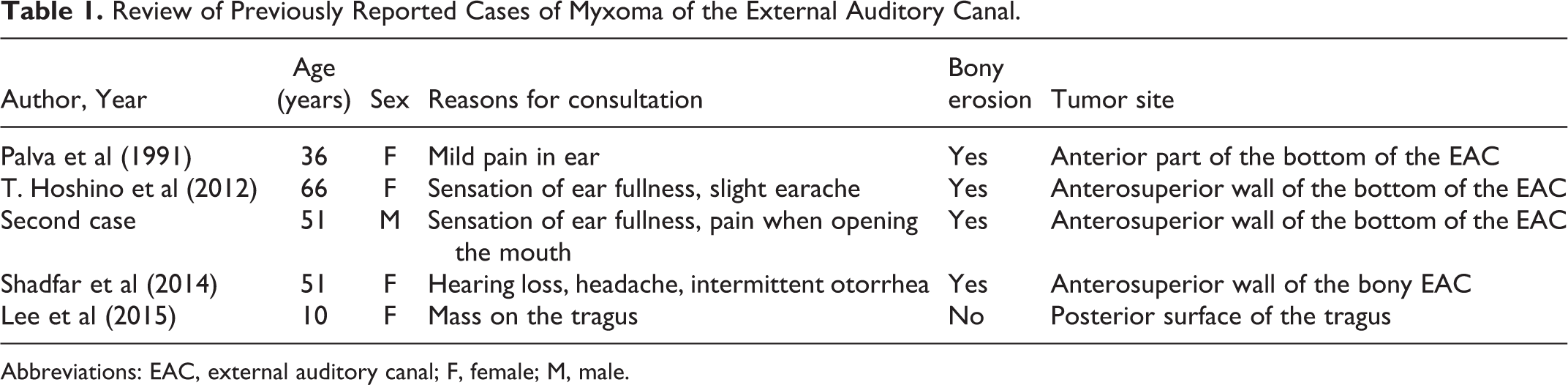
Abbreviations: EAC, external auditory canal; F, female; M, male.
Isolated myxoma of the external auditory canal is extremely rare. After a PubMed search, only 5 cases reported in English literature were found.2-5
Myxomas develop equally in both sexes and most frequently in the 20 to 30 age range. 7 These tumors present as ovoid, soft, and sessile mass with smooth borders.
Despite being benign, myxomas have also local aggressive potential. Myxomas destroy the bone by aseptic pressure necrosis. Many authors have described extensive bony erosion. Shadfar has reported a case of myxoma extending into the glenoid fossa.3,8
Computed tomography and magnetic resonance imaging are useful for clarifying extension to adjacent tissues, searching for underlying bone lysis or very rare intracranial extension, and planning surgical excision. However, the imaging data are not specific.4,9
Our observation has 2 peculiarities compared to those reported in the literature. The first is that the myxoma is inserted on the posterior wall of the cartilaginous and bony external auditory canal, whereas in the other cases, it was located at the level of the anterior bony wall and posterior surface of the tragus. The second is that there was no bone lysis while other authors have described bone lysis next to the basis of myxoma insertion.2-5
In all cases reported in the literature, there was no involvement of the tympanic membrane or middle ear space. Fine needle aspiration and cytology were performed by Lee. Thick, yellow, mucoid fluid was aspirated, and cytology was nondiagnostic.
Myxoma can be confused with other tumors and pseudotumors that have a myxoid component. The myxoid skin cyst is usually located in the fingers. Focal oral mucinosis is another myxoid lesion in the gingiva and hard palate. In front of a mass of the external auditory canal, other diagnoses can be evoked such as schwannoma, skin cancer, and fibrous dysplasia.2,9
Usually myxomas are part of Carney syndrome. It constitutes an autosomal dominant syndrome comprising myxomas of the heart and skin, hyperpigmentation of the skin (lentiginosis), and endocrine overactivity.
The histological appearance of sporadic myxoma is identical to that of Carney syndrome. Only a good physical examination, a cardiac ultrasound, and biological tests can eliminate this syndrome.
The genetic study also makes it possible to look for a mutation of the PRKAR1A gene which is the most frequent mutation in this syndrome.10,11 This gene provides instructions for making one part of an enzyme called protein kinase A. This enzyme promotes cell growth and division (proliferation). The genetic study was not carried out in our patient because of the unavailability of this examination.
The treatment of myxoma is based on surgery. Radiation therapy and chemotherapy have been tried in cases of facial myxoma with poor results but have not been tested in the external auditory canal.3,9 In all cases that has been reported in the literature, the surgery was carried out via a postauricular incision except for 1 case of myxoma of the tragus posterior surface.
Given the locally destructive nature of these tumors, accurate identification of tumor margins remains difficult, and recurrences have been reported as high as 25% in patients undergoing effective enucleation. Recurrence has been noted as early as 3 months and as late as 10 years after initial surgical resection.3,7
Therefore, long-term follow-up is recommended due to the high risk of recurrence in the setting of failed complete extirpation.
Conclusion
Isolated myxomas of the external auditory canal are extremely rare. Only, few cases were reported in the literature. We report here the sixth case.
The otolaryngologist must evoke the diagnosis of myxoma in front of a mass of the external auditory canal and when this diagnosis is confirmed, he must not forget to look for a Carney syndrome that can be serious and even fatal. Although myxomas are benign, they also have local aggressive potential and a careful assessment should be made in this regard.
Footnotes
Authors’ Note
The patient provided written informed consent.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.