
Abstract
Objectives:
The aim of this study was to analyze the risk of malignancy in salivary gland tumors on the basis of the Milan System for Reporting Salivary Gland Cytopathology.
Methods:
A retrospective review was performed of the charts of patients with salivary gland tumors in whom the final diagnosis was confirmed by surgical excision. Preoperative fine needle aspiration results were categorized according to the Milan System for Reporting Salivary Gland Cytopathology: non-diagnostic (category I), nonneoplastic (category II), atypia of undetermined significance (category III), neoplasm (category IV), suspicious for malignancy (category V), and malignant (category VI). Fine needle aspiration and final diagnosis were compared, and the risk of malignancy and operative/oncological outcomes were analyzed.
Results:
A total of 288 patients were enrolled in this study. Postoperative histopathologic salivary gland malignancies were found in 30 (10.4%) patients. Risk of malignancy was 7.1%, 0%, 48.0%, 4.8%, 88.7%, and 100% in categories I, II, III, IV, V, and VI, respectively. The most common malignant tumor in category III was salivary duct carcinoma (37.5%), followed by acinic cell carcinoma (25.0%), mucoepidermoid carcinoma (25.0%), and squamous cell carcinoma (12.5%). The 5-year survival rate of patients with malignant tumors showed no statistical difference between category III and category V/VI (P = .140). Risk of malignancy was 88.9% and 100% in category V and VI, respectively.
Conclusions:
A half of atypia of undetermined significance (category III) cases were malignant. Once diagnosed, the prognosis of malignant tumor in category III was similar with that in category V/VI.
Introduction
Salivary gland cancers are morphologically distinct and rare malignancies constituting approximately 5% of head and neck cancers. 1 Fine needle aspiration (FNA) is a well-accepted diagnostic tool used in the preoperative evaluation of salivary gland mass lesions to distinguish nonneoplastic lesions from neoplastic tumors and benign tumors from malignant ones. 2 Fine needle aspiration is a minimally invasive, cost-effective, and relatively well-tolerated procedure performed in an outpatient clinical setting or under ultrasound guidance.3,4 The cytomorphologic findings of material aspirated from salivary glands play an important role in the risk stratification and management of patients presenting with a salivary gland mass. It has been shown that unnecessary surgery can be avoided in approximately one-third of cases based on the preoperative FNA diagnosis. 5 Patients with nonneoplastic lesions are followed up by vigilance for potential symptoms, whereas patients with a neoplastic diagnosis are candidates for surgical intervention.
Salivary gland FNA has been reported to have a high specificity for the detection of neoplasia (98%) and malignant processes (96%). However, the sensitivity has been reported to be lower and more variable: 96% and 79% for detection of neoplasia and malignancy, respectively. 6 The lower sensitivity has been attributed to morphologic heterogeneity, a variety of epithelial metaplastic changes, and even occasionally cystic changes.7-11 Moreover, morphologic overlap between primary neoplasms of salivary glands and metastatic neoplasms contributes to the complexity of the diagnosis. Limited diagnostic material is another reason for the lower sensitivity, which precludes ancillary testing to reach a definitive diagnosis. However, an indeterminate diagnosis despite cellular adequacy, even in the hands of an experienced cytopathologist, is not an uncommon finding. An indeterminate interpretation may be associated with a nearly 2-fold increased likelihood of malignancy on final diagnosis compared to in the overall group. 12 In a previous study, more than half of the subset of “atypical” salivary gland FNAs with histological resection turned out to be malignant tumors. 13
To address the lack of guidelines, risk-stratification classification schemes for reporting findings of salivary gland FNA have recently been suggested.14,15 At the European Congress of Cytology meeting held in Milan, Italy, in 2015, a group of pathologists initiated the development of an international classification scheme for salivary gland FNA, known as the Milan System for Reporting Salivary Gland Cytopathology (MSRSGC). 16 Although there is much information on the general performance of salivary gland FNA, much less is known specifically about “atypical” and “suspicious for malignancy” salivary gland lesions and the impact that this category would have on a tiered classification scheme. In this study, we aimed to analyze the risk of malignancy of salivary gland tumors by FNA results, and characteristics of cancer patients according to FNA results classified according to the MSRSGC.
Materials and Methods
Patients
This study was approved by the institutional review board (IRB No. L-2019-169). We retrospectively reviewed the clinical and pathological data of 432 patients who had undergone parotidectomy or submandibular resection at the Department of Otorhinolaryngology-Head and Neck Surgery from January 2008 to December 2017. Exclusion criteria were (1) no preoperative FNA result (n = 43); (2) surgery undertaken by another department (n = 94); (3) FNA undertaken by another institution which cannot be reviewed (n = 27); and (4) revision cases (n = 16). After excluding 144 patients who met the abovementioned exclusion criteria, a total of 288 patients were included in this study. All patient evaluations included a clinical history, ultrasonography with FNA of the parotid or submandibular gland, and computed tomography (CT) and/or magnetic resonance imaging (MRI). The following data were also collected: patient’s age, gender, tumor size, and final histologic findings.
Fine Needle Aspiration, Pathological Diagnosis, and Treatment Policy
In our institute, all FNA was carried out using a 25-gauge needle and standard aspiration technique by a surgeon, a pathologist, or a radiologist. Fine needle aspiration was performed by a surgeon or pathologist when the tumor was superficial and easily palpable, while it was performed by the radiologist with ultrasonography when the tumor was not easily detected on physical examination. Histology was evaluated and reviewed with knowledge of the FNA by 1 pathologist. Computed tomography with or without MRI scan was performed preoperatively, and intraoperative frozen section was performed in case the tumor was on the suspicion of malignant tumor. In general, partial or superficial parotidectomy was performed when FNA findings indicated benign tumor, and total parotidectomy with or without neck dissection was performed in case of atypia of undetermined significance with highly suspicious of malignant tumor, suspicious for malignancy, or malignant in FNA report.
Patient Grouping and Statistical Analysis
The preoperative results of FNA cytology were categorized according to the MSRSGC classification as follows: (1) nondiagnostic (category I), (2) nonneoplastic (category II), (3) atypia of undetermined significance (category III), (4) neoplasm (category IV), (5) suspicious for malignancy (category V), and (6) malignant (category VI).
Results of imaging studies using ultrasonography, CT, or MRI were reviewed, including size of tumor, location, deep lobe involvement, margin irregularity, necrosis, and adjacent lymph node enlargement. Risk of malignancy and type of malignancy were evaluated according to MSRSGC. In each category of this classification, the associations between clinicoradiologic characteristics and malignancy risk were evaluated. Continuous outcomes were analyzed using the independent t test between groups of 2, and dichotomous outcomes were analyzed using the χ2 test for trend and logistic regression analysis. Cumulative survival rates were calculated using life table analysis to analyze changes in outcome. Cox regression analysis was performed to assess the difference in disease-specific survival according to the category identified by life table analysis. Statistical analysis was performed using SPSS V21.0 (IBM SPSS). Statistical significance was considered to be P < .05.
Results
The male to female ratio was 1.25:1 (male 160, female 128) and the mean age was 53.2 ± 15.9. The incidence of malignant tumor among all of the surgical cases was 10.4% (30/288). Numbers of patients in each pathological category were as follows: category I, n = 16 (5.6%), category II, n = 15 (5.2%), category III, n = 17 (5.9%), category IV, n = 229 (79.5%), category V, n = 9 (3.1%), and category VI, n = 2 (0.1%). Median follow-up duration of malignant tumor was 26.4 months (1-213 months).
Risk of Malignancy
According to the final pathology, risk of malignancy for each category was as follows: category I—7.1% (1/16), category II—0%, category III—48.0% (8/17), category IV—4.8% (11/229), category V—88.7% (8/9), and category VI—100% (2/2; Figure 1). Among the malignant tumors in each category, the proportions of those with high-grade malignancy were 0%, 62.5%, 9.1%, 75.0%, and 100% in categories 1, 3, 4, 5, and 6, respectively (Table 1). Among the low-grade malignant tumors, acinic cell carcinoma was most frequent (23.3%), while salivary ductal carcinoma was most frequent in the high-grade malignant tumors (26.7%).
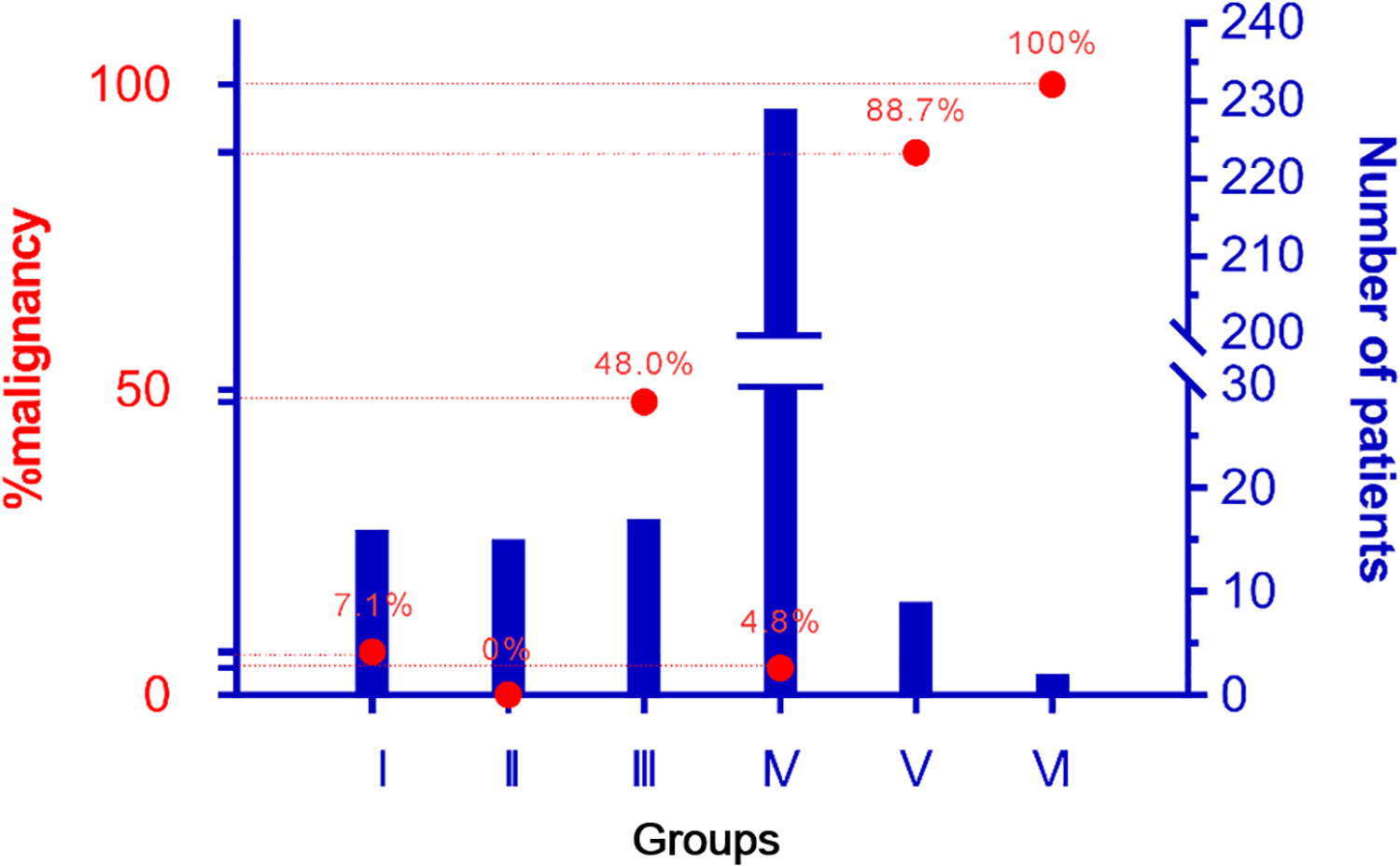
Risk of malignancy (%) and number of patients of each groups.
Types of Malignancy in Each Groups.
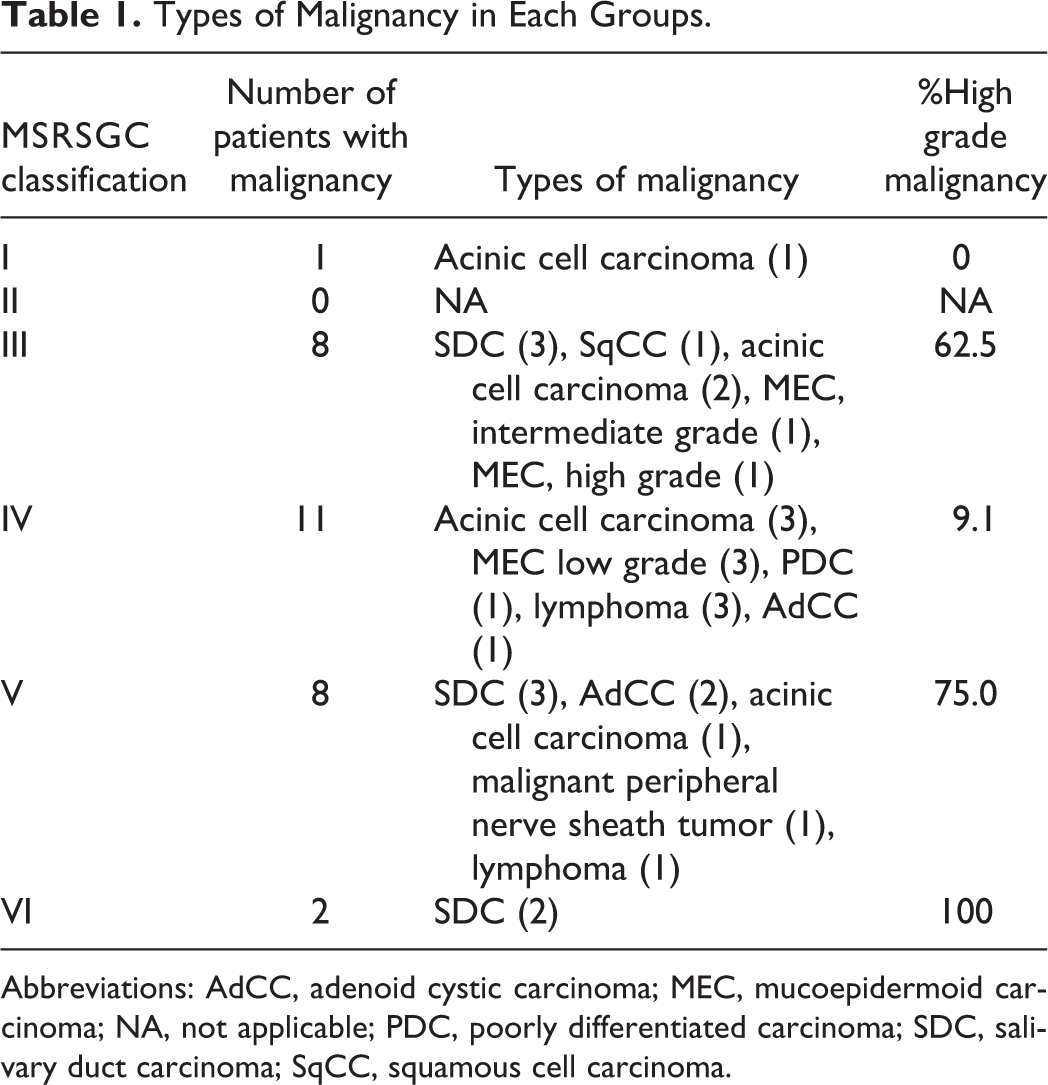
Abbreviations: AdCC, adenoid cystic carcinoma; MEC, mucoepidermoid carcinoma; NA, not applicable; PDC, poorly differentiated carcinoma; SDC, salivary duct carcinoma; SqCC, squamous cell carcinoma.
Atypia of Undetermined Significance in FNA (Category III)
Over a half of patients with category III (atypia of undetermined significance (AUS)) were diagnosed as malignant tumors postoperatively (Table 2). Among the benign tumors, Warthin’s tumor was the most frequent (33.3%), followed by pleomorphic adenoma (22.2%), basal cell adenoma (22.2%), myoepithelioma (11.1%), and intraparotid lymph node carcinoma (11.1%). Of the malignant tumors, salivary duct carcinoma was the most frequent (37.5%), followed by acinic cell carcinoma (25.0%), mucoepidermoid carcinoma (25.0%), and squamous cell carcinoma (12.5%). The 5-year disease-specific survival rate of patients with malignant tumors in category III was 66.7%, while no patients in category V and VI (except lymphoma of final pathology) with malignant tumors survived. However, the survival curve showed no statistical difference between category III and category V/VI (P = .140; Figure 2). Because category III showed about 50% of malignant potential, further analysis was performed to increase the predictive power with clinical and radiological features. Patients’ age and gender were about the same when comparing final pathology of benign and malignant tumors (P = .453 and P = .627, respectively). Regarding the results of imaging studies, size of tumor, anterior location, deep lobe involvement, irregular margin, necrosis of tumor, and adjacent lymph node enlargement were not different between benign and malignant tumors in the case with AUS (category III; P = .987, 0.735, 0.627, 0.183, 0.627, and 0.183, respectively; Table 3).
Final Pathology of Benign and Malignant Tumor in Patients With AUS.
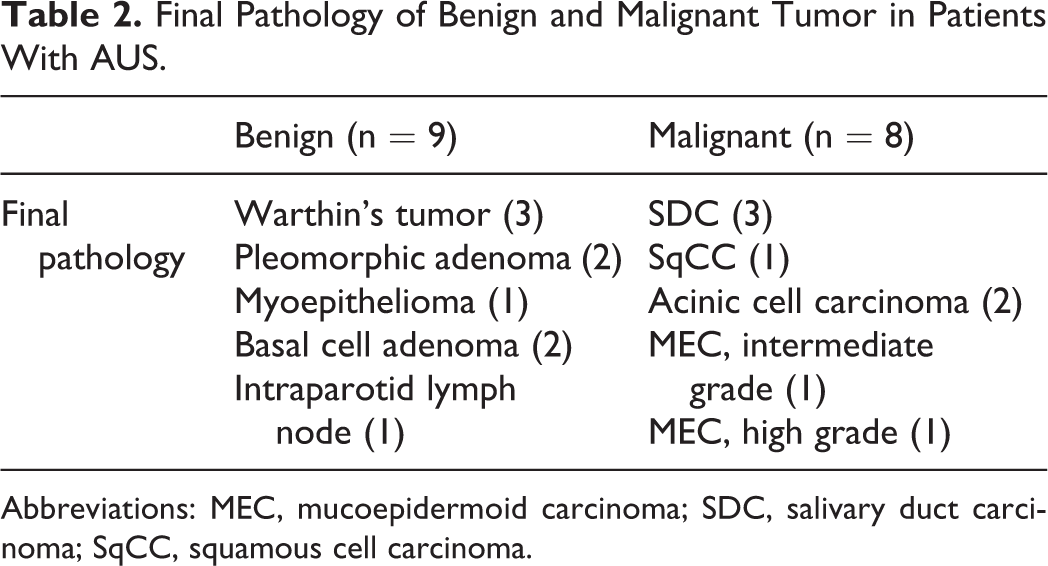
Abbreviations: MEC, mucoepidermoid carcinoma; SDC, salivary duct carcinoma; SqCC, squamous cell carcinoma.
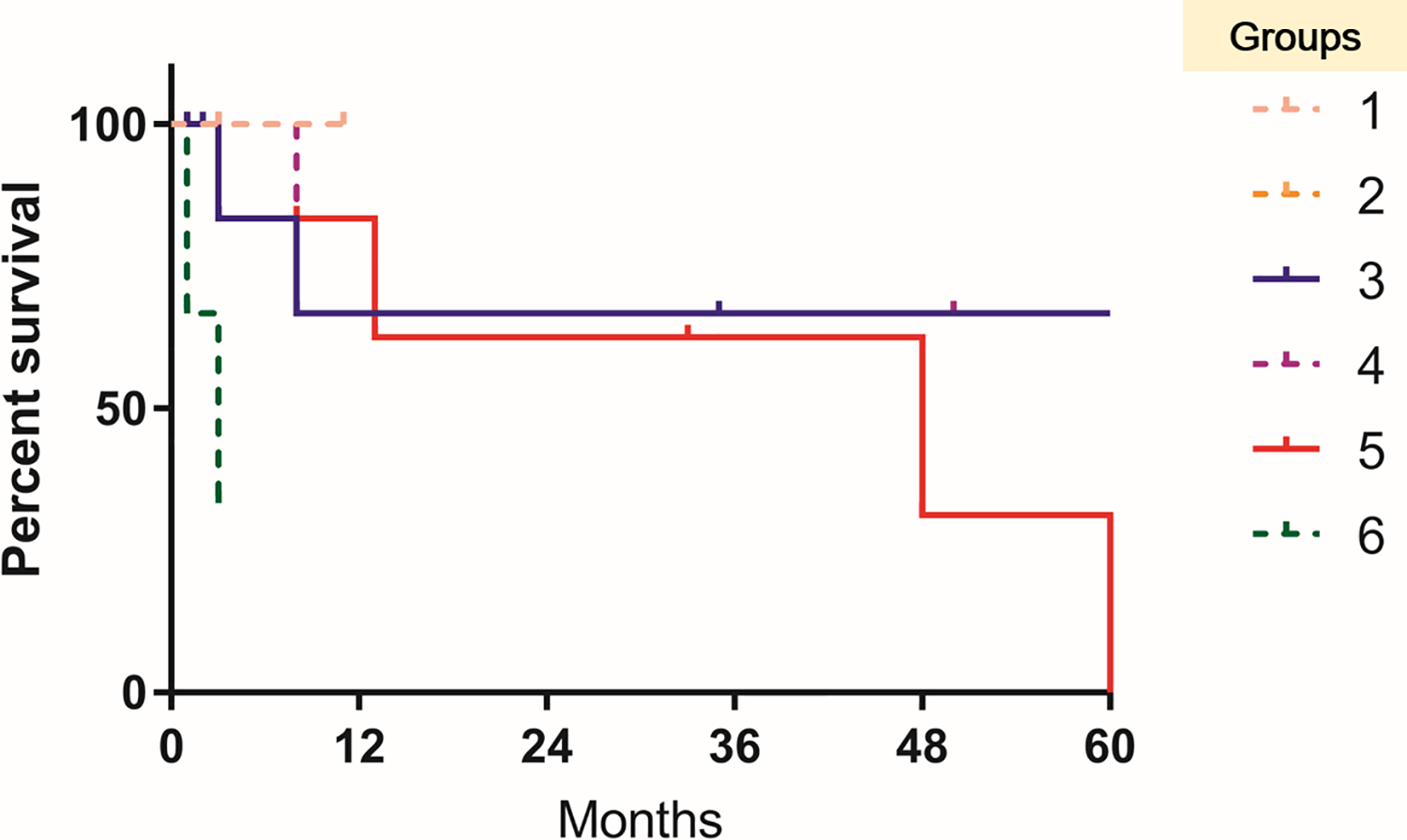
Disease-specific survival of malignant tumor of each groups. The survival curve showed no statistical difference among groups.
Comparison of Clinicoradiologic Characteristics in Benign and Malignant Tumor of AUS in Fine Needle Aspiration.
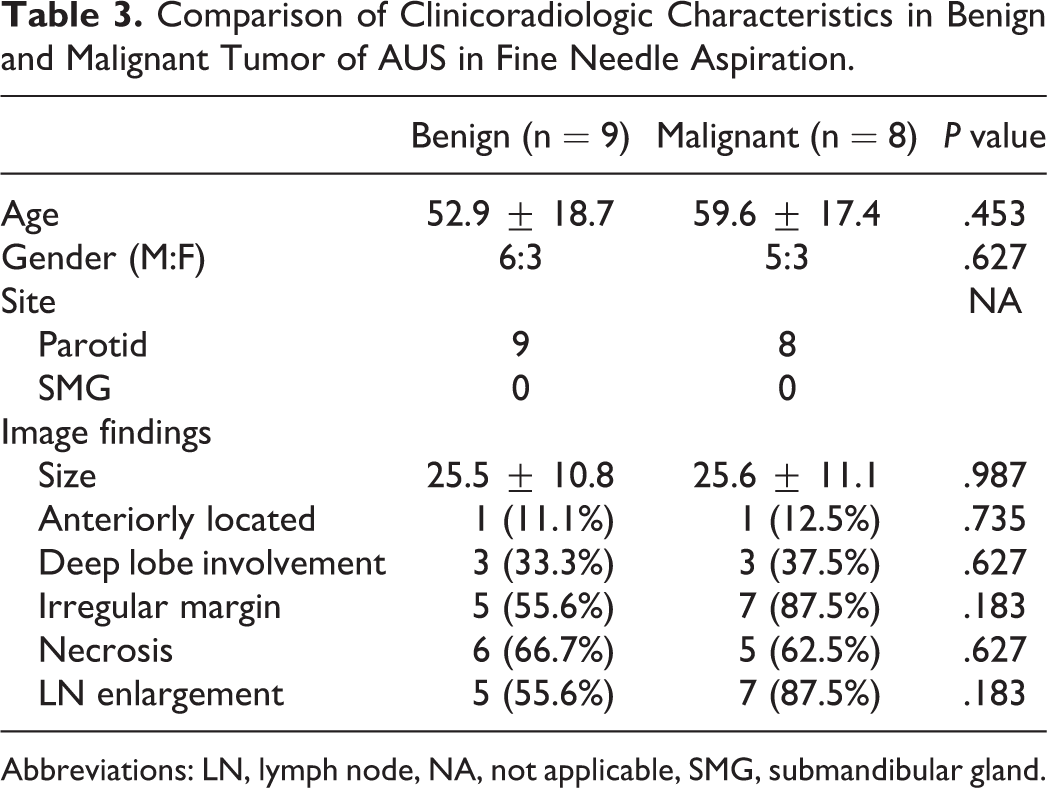
Abbreviations: LN, lymph node, NA, not applicable, SMG, submandibular gland.
Discussion
This study demonstrated that the incidence of malignant tumors among all surgical cases of salivary gland tumors was 10.4% (30/288), and risk of malignancy for each group according to the Milan classification and proportion of high-grade malignancy was highest in group 6, followed by group 5 and group 3. About half of the AUS samples turned out to be malignant tumors, which included salivary duct carcinoma, acinic cell carcinoma, mucoepidermoid carcinoma, and squamous cell carcinoma. Of the benign tumors in group 3, Warthin’s tumor was most frequent. The survival rate was not significantly different between group 3 and group 5/6.
Recent prospective study showed the malignant potential of 6 groups of Milan system by analyzing 119 patients. 17 Although the number and proportion of patients in each group were different from our study, malignant potential of each group showed similar range with our results. In the study, malignant potential of AUS was not shown, as patient with AUS was not included. In our study, group 4 which mostly included cases of benign salivary gland tumor showed about 5% malignancy risk. Pleomorphic adenoma is the most common cytological diagnosis in FNA specimens from salivary glands. 18 Scarcity of matrix material with a dominant epithelioid or myoepithelial cell component can lead to misdiagnoses, with the most commonly misdiagnosed malignant tumor being acinic cell carcinoma. 9 Conversely, acinic cell carcinoma can be confused with pleomorphic adenoma. In our study, the most common malignant tumor in group 4 was also acinic cell carcinoma (27.3%). The second most common benign tumor of the salivary gland is Warthin’s tumor, which is characterized by 3 components, including sheets of oncocytes, a polymorphous population of lymphocytes, and a dirty granular background. 19 The differential diagnosis of salivary gland lesions with oncocytic features includes oncocytosis, oncocytoma, Warthin’s tumor, oncocytic carcinoma, pleomorphic adenoma, the oncocytic variant of mucoepidermoid carcinoma, and acinic cell carcinoma. In our study, 1 case of benign tumor was found on final pathology in group 5, and this was an oncocytoma.
A previous study reported that in 6249 cases of salivary gland tumors, the sensitivity and specificity were 73% and 91%, respectively. 9 In other studies, the range of FNA accuracy was found to be from 88% to 98%, with an average of 92%.20-23 Recently, Tommola et al reported the salivary gland FNA diagnostics using the Milan system. 24 The study reported that the MSRSGC performance in patient-based analysis was as follows: accuracy was 90.9%, sensitivity was 61.5%, specificity was 100%, positive predictive value was 100%, and negative predictive value was 89.4%, respectively. In this study, sensitivity and specificity were 73.2% and 95.6%, respectively, and positive and negative predictive values for malignant tumor were 75.0% and 95.2%, respectively, which is in accordance with previous studies.
In our study, age and gender were about the same when comparing the final pathology of cases of benign and malignant tumors with AUS. Although our study also failed to show a statistically significant difference in radiologic characteristics of benign and malignant tumors with AUS on the FNA result, irregular margin and adjacent lymph node enlargement were much higher in malignant tumors (55.6% vs 87.5%, and 55.6% vs 87.5%, respectively). An aggressive salivary gland tumor typically shows an ill-defined, infiltrative border, heterogeneous internal signal with cystic change and necrosis when assessed by both MRI and CT.25,26 The internal signal is characteristically low to intermediate on both T1W and T2W images. The surrounding soft tissue, subcutaneous tissue, and skin may be infiltrated. On dynamic MRI, malignant tumors are shown to exhibit early enhancement and slow washout. 27 However, a low-grade malignant lesion generally has imaging features overlapping those of a benign salivary gland tumor. 26 We think that inclusion of many low-grade carcinomas in our cohort and the small number of patients were the reasons why radiologic features failed to attain statistical significance.
Some studies report that FNA has evident limitations for diagnosis of malignancy in major salivary gland neoplasms. False prediction is up to 40%, when not diagnosed by FNA. With a specificity value of 97.5%, FNA could be considered as a good test for confirmation, but not as a suitable screening test for malignancy. 28 In order to reduce false prediction, firstly, as mentioned above, clinical characteristics on modalities such as ultrasonography should be taken into consideration, 29 and there should also be discussion and consultation with another experienced pathologist before a final decision is taken on the results. 12
Malignant tumor presenting with preoperative AUS seems not to affect the disease-specific survival. So far, there has been no study regarding the role of preoperative FNA result in survival in salivary gland cancer. Our study demonstrated that the survival of group 3 was about the same with group 5/6 (Figure 2). In general, there can be several reasons for no effect of preoperative pathologic confirmation of salivary cancer on survival in group 3, group 4, and group 5. First, surgeons prepare for the extent of resection required by using imaging studies as well as FNA results. In high-grade carcinoma, wider surgical resection can be performed when there is suspicion of malignancy on imaging studies. In low-grade carcinoma, although surgical resection may not be as extensive as in high-grade cancer, this does not influence the prognosis unless the surgical margin is violated. Second, many surgeons utilize frozen sections. Although not perfect, frozen-section pathology for parotid lesions has high accuracy and utility in intraoperative decision-making, facilitating timely, complete procedures. 30
In summary, in our study about 5% of cases showed AUS on FNA of salivary gland tumor. Malignant risk in cases with AUS was about 50%. Most of the malignant tumors from the MSRSGC classification III category were high grade, while those in the classification IV category were mostly low grade. No clinicoradiologic parameters were found to be associated with risk of malignancy in cases with AUS. Considering the risk of malignancy and the proportion of high-grade cancer in cases with AUS on FNA of the salivary gland tumor, proper preoperative evaluation, and intraoperative management is needed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.