
Abstract
Objectives:
To review the diagnosis of patulous Eustachian tube (PET) based on the diagnostic criteria for the PET proposed by Japan Otological Society (JOS).
Methods:
We reviewed typical aural symptoms of PET, Eustachian tube (ET) obstruction procedure to confirm diagnosis of PET, objective findings of a patent ET obtainable from observation of the movement of the tympanic membrane, and by ET function tests (tubo-tympano-aerodynamic graphy, sonotubometry). In addition, usefulness of other tests such as patulous Eustachian tube handicap inventory-10 (PHI-10), sonotubometry with postural change (Ohta method), and sitting computed tomography (CT) to diagnose PET is described.
Results and Conclusions:
We have described the diagnosis of PET based on the diagnostic criteria for PET proposed by JOS; PHI-10, Ohta method, and sitting CT are also useful for the diagnosis of PET. Further investigation is needed for an accurate diagnosis and precise evaluation of the pathophysiology of this challenging disease.
Keywords
Introduction
The Eustachian tube (ET) is closed under normal conditions and opens temporarily during swallowing. 1,2 There are 3 primary ET functions: gas transfer and pressure equalization between the nasopharynx and middle ear (ME), prevention of sound and fluid reflux from the nasopharynx, and clearance of secretions from the ME through mucociliary transport. 3 Patients with patulous Eustachian tube (PET) have annoying aural symptoms such as autophony of voice or breathing sounds and aural fullness, among other complaints, due to persistent opening of the normally closed ET. 2 The severity of these symptoms range from being asymptomatic to causing severe disturbances in the quality of life and even inducing suicidal tendencies. Several findings, such as medical history, physical examinations, and ET function tests, are combined to diagnose PET. 4,5 There is no single ET function test available to evaluate ET function accurately in all cases without the aid of other clinical observations and examinations. 4,6
Diagnostic Criteria for the PET Proposed by the Japan Otological Society
Most clinical studies of PET have been reported by different institutions using their own means of diagnosing PET due to the lack of an established set of diagnostic criteria for PET. The Japan Otological Society (JOS) advocated for standardizing the diagnostic criteria for PET (Table 1). 6 If all 3 criteria are met (1 + 2 + 3), the diagnosis of “definite PET” is made, whereas if only 2 criteria are met (1 + 2 or 1 + 3), the diagnosis of “possible PET” is made. These criteria were intended to prevent any ambiguity in the diagnosis of definite PET. Furthermore, it was also intended to minimize the number of cases that could be accidentally excluded even in the presence of some suspected findings. For this purpose, patients fulfilling some but not all criteria are diagnosed with possible PET. As the ET function may vary even over a relatively short period, repeated testing on another occasion is recommended to increase the chance of reaching a diagnosis of definite PET should the first diagnosis be possible PET. All otolaryngologists can use the criteria even without using the ET function test apparatus. However, the use of such an apparatus could increase the chances of detecting definite PET. In this review, we will describe the diagnosis of PET based on these criteria.
The Japan Otological Society Diagnostic Criteria for PET.a
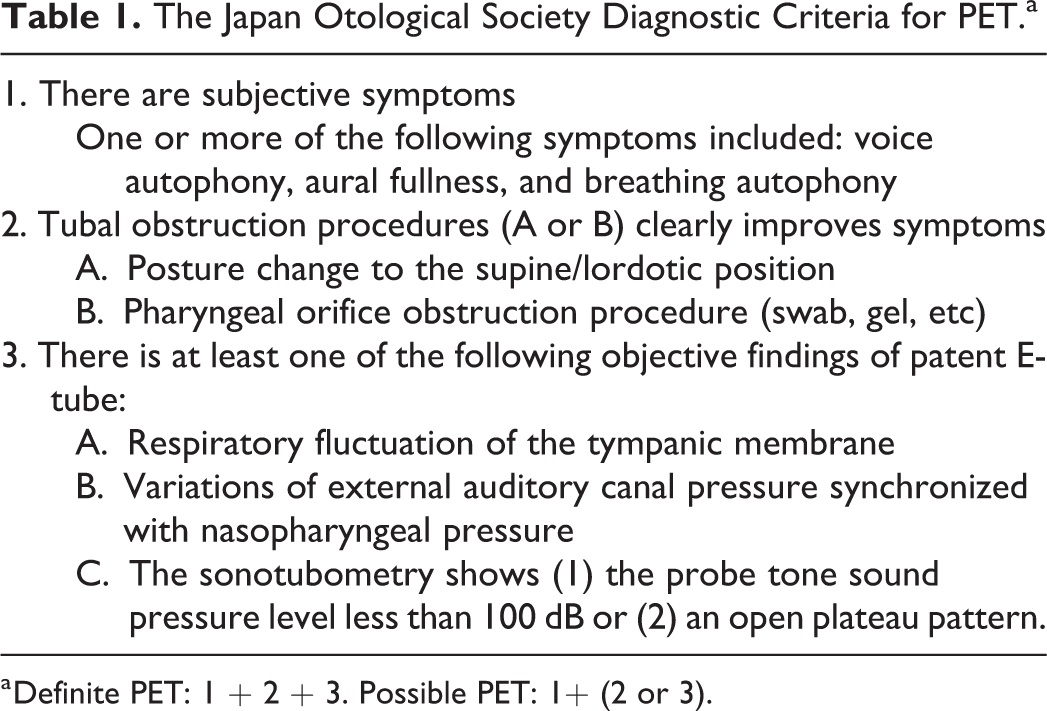
a Definite PET: 1 + 2 + 3. Possible PET: 1+ (2 or 3).
Aural Symptoms
Aural symptoms such as voice and breathing autophony and aural fullness are categorized as item 1 in the JOS criteria (Table 1). These symptoms are caused by an excessive transmission of sound and pressure from the nasopharynx to the ME via an open ET. Voice autophony, a sense of aural fullness, and breathing autophony were observed in 93.6%, 87.2%, and 78.2%, respectively, of definite PET cases. 7 All 3 symptoms were detected in 67.9% of cases. 7 The most annoying aural symptom of PET is usually autophony of voice. 8 This symptom can be especially frustrating for individuals whose work requires frequent communication. It is essential to pay attention to the fact that the specificity of breathing autophony was the highest, and it is one of the most essential keys to differentiate PET from superior canal dehiscence syndrome or sensorineural hearing loss. 9,10 It is also important to note that functional hyporhinolalia was observed in about 17% of patients with PET. 11 These patients seem to modify their vocalization process in order to decrease the vocal sound entering the nasopharynx 11 -14 without being consciously aware that they are doing so.
Tubal Obstruction Procedures
Tubal obstruction procedures are categorized as item 2 in JOS criteria (Table 1). Symptoms of PET should theoretically be eliminated or alleviated by obstructing the open ET at the time of symptom manifestation. There are 2 ways of obstructing the ET. One is a postural change to a lying or lordotic position, causing the closure of the ET in most cases. Second is a direct obstruction of the pharyngeal orifice by swab or jelly like substances. In the majority of PET cases, these symptoms can be temporarily relieved by postural changes into a supine or lordotic position. This is due to congestion in the pterygoid venous plexus and veins in the lateral pterygoid muscle. 15 However, in about 9% of patients with definite PET, 7 the patulous tube does not close, and PET symptoms do not improve by these posture changes. In such cases, diagnosis can be confirmed by a transnasal pharyngeal orifice obstruction procedure using a swab, gel, and so on (Figure 1).

Direct obstruction of the pharyngeal orifice (right) with gel (middle) is performed using a transnasal approach (left).
Objective Findings
Objective findings of a patent ET are categorized as item 3 in JOS criteria. Three findings, such as the movement of the tympanic membrane (TM) upon respiration, tubo-tympano-aerodynamic graphy (TTAG), and sonotubometry, were adopted.
Observation of TM
Tympanic membrane observation should be performed in the sitting position with an endoscope or microscope. Instruct the patient to breathe deeply through the nose, during which the mouth is closed and the nostril on the other side is also occluded with a finger. If the TM is retracted, or if there is ET lock due to nasal sniffing, 16 -21 auto inflation of the ME using Valsalva maneuver or ET catheter inflation at low pressures is performed, since it is easy to obtain TM movement after releasing retraction of the TM.
Eustachian tube function tests
The ET function test apparatus (Figure 2) can be used to carry out 2 objective tests of ET function. Tubo-tympano-aerodynamic graphy 22,23 measures pressure transmission from the nasopharynx to the external auditory canal (EAC) via ET and ME. Sonotubometry 24,25 measures sound transmission from the nasopharynx to the EAC via the ET and ME. According to the diagnostic criteria proposed by the JOS (3), 76.9% ears with definite PET were positive in TTAG, and 55.1% were positive in sonotubometry. 7

Tubal function test apparatus (Rion JK05A).
Pressure changes in the EAC and nasopharynx are simultaneously measured using the manometry mode of the TTAG (Figure 3). Positive findings of TTAG are defined as an EAC pressure change synchronous with that in the ipsilateral nasal cavity or nasopharynx (Figure 3: right). Sonotubometry assesses sound transmission via the ET. The acoustic signal comprises a 7 kHz octave band noise that is presented into the nasopharynx, using a special speakerphone with an olive-shaped tip placed at the nostril. The sound pressure level (SPL) of probe tone is monitored by a microphone inserted into the EAC (Figure 4). The intensity level of the probe tone, presented to the nasopharynx, is automatically adjusted so that the monitored probe tone level measured at the EAC is calibrated at a preset level of 50 dB. The relative probe tone intensity level, compared to 50 dB, measured at the EAC is monitored with time. When it is necessary to lower the nasopharyngeal probe tone SPL to below 100 dB (Figure 4: middle), it is regarded as a positive finding of a patent ET. Similarly, an “open plateau pattern” that is obtained when the ET opens upon swallowing and remains open (Figure 4: right) is regarded as positive finding of a patent ET.
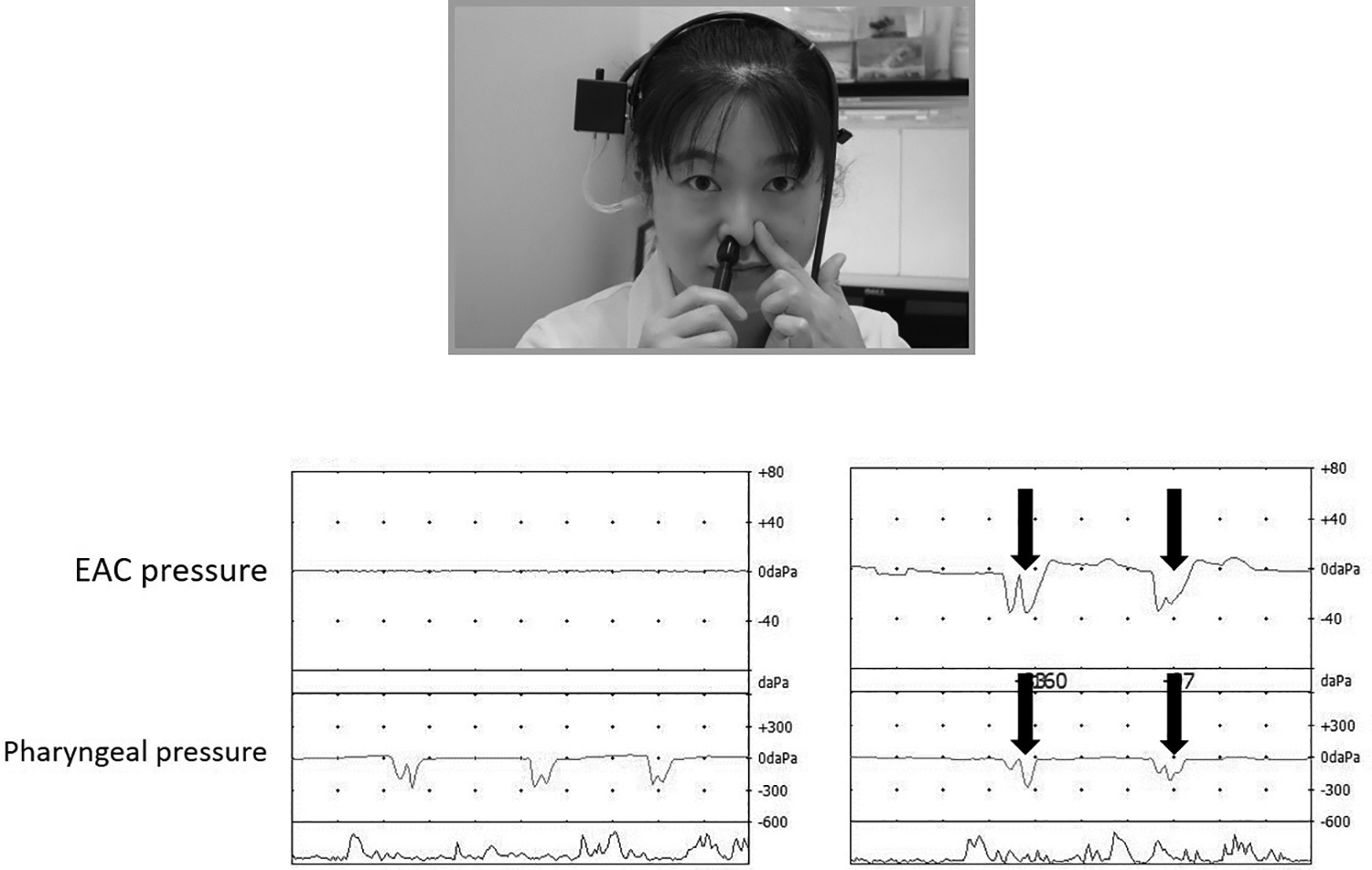
Typical TTAG recordings in normal (left) and PET (right) case. Synchronous changes in the EAC pressure is seen induced by respiration in PET (right: black arrow). EAC indicates external auditory canal; PET, patulous Eustachian tube; TTAG, tubo-tympano-aerodynamic graphy.
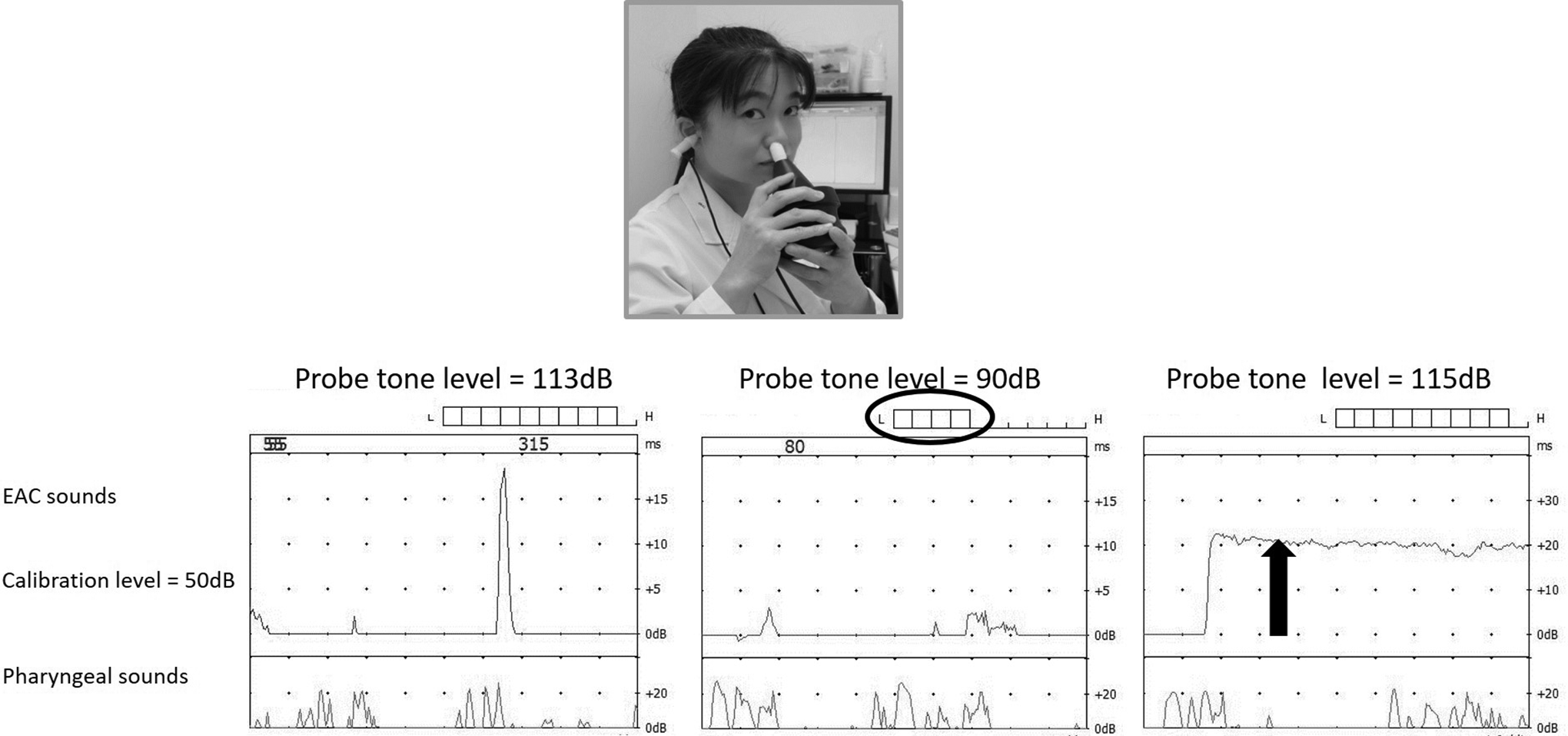
Examples of typical sonotubometric recordings in normal (left) and PET (middle and right) cases. Lowering of the probe tone SPL to less than 100 dB (middle). The ET opens when swallowing and remains continuously open thereafter (right). EAC indicates external auditory canal; ET, Eustachian tube; PET, patulous Eustachian tube; SPL, sound pressure level.
Additional Useful Tests and Examinations
Patulous ET Handicap Inventory-10
Subjective findings are as important as objective findings to evaluate PET severity and outcome. Poe 9 proposed an outcome measurement system to assess the amount of aural symptoms. That is defined as (1) complete relief, (2) significant improvement, (3) slight improvement, (4) unchanged, and (5) worse. Bartlett et al 26 reported a “BBK scale” composed of 7 questions addressing PET symptoms as follows: (1) When I talk I hear my voice echoing in my ear; (2) When I breathe I can hear my breathing in my ear; (3) My ear feels plugged and full; (4) When my voice is echoing in my ear, environmental sounds are too loud or bothersome around me; (5) My symptoms improve when I lie down; (6) When I sniff, my symptoms in my ears get better; and (7) My symptoms resolve when I put pressure behind my ear or on my neck. Each item was evaluated by the Likert scale (1: none of the symptoms to 10: very severe symptoms).
Patulous Eustachian tube handicap inventory, which is a modification from the tinnitus handicap inventory-12, 27,28 is a valuable tool for assessment of PET severity (Table. 2). 29 Grading of PET severity is defined as (1) no handicap (0-8), (2) mild handicap (10-16), (3) moderate handicap (18-24), and (4) severe handicap (26-40). The PHI-10 is also useful for the evaluation of treatment outcomes for PET. 30 However, it must be emphasized that this PHI-10 is valid only if the patients are adequately diagnosed with PET, which is a universal truth for any other diagnostic scoring system.
Patulous Eustachian Tube Handicap Inventory-10.a
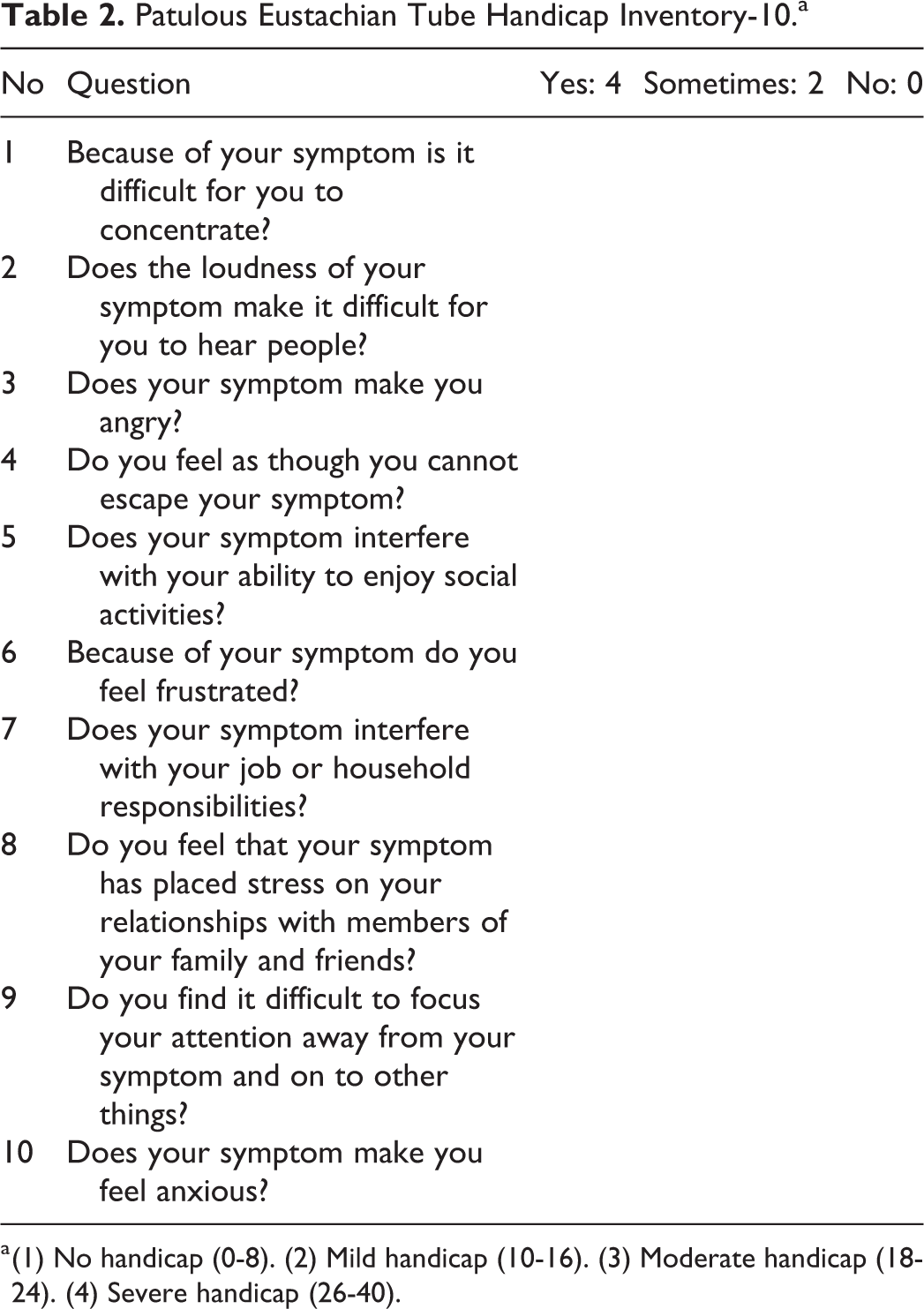
a (1) No handicap (0-8). (2) Mild handicap (10-16). (3) Moderate handicap (18-24). (4) Severe handicap (26-40).
Sonotubometry With Postural Change (Ohta Method)
This is a unique and useful method to diagnose PET. Sonotubometry is performed during postural change from the forward-bending to sitting positions. 31,32 Measurements are started 20 seconds after adopting the forward-bending position. The principle behind this method is that the nasopharyngeal probe SPL necessary to create an EAC SPL of 50 dB is measured in different positions. The necessary nasopharyngeal SPL will be low in the sitting position when the ET is open, but it will increase when the ET is closed in the forward-bending position. This method measures the difference of probe tone SPL in the 2 conditions. The threshold for a patent ET has yet to be officially determined but a change in probe tone SPL exceeding 10 dB is currently regarded as a positive finding (Figure 5: right).
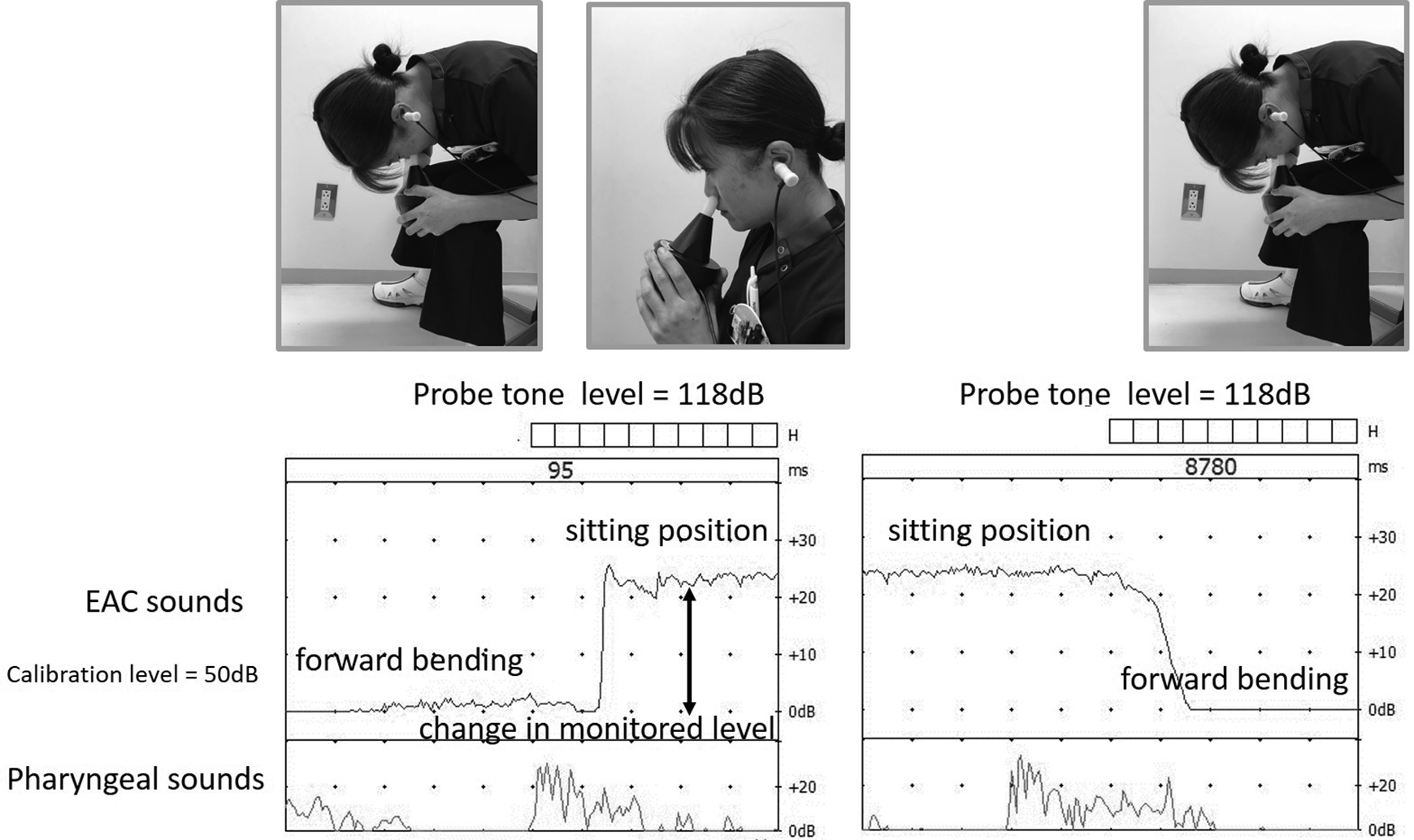
Examples of typical sonotubometric recordings with postural change in normal (left) and PET (right) cases. Sound attenuations from the speaker (probe) to the microphone in the sitting and forward-bending positions. The level difference was observed as a dynamic change of probe tone level in response to the postural change from the forward-bending to sitting positions. PET indicates patulous Eustachian tube.
Imaging
As posture is an essential factor in the pathophysiology of PET because the ET lumen is dilated in the sitting and standing position, the diagnosis of PET by conventional recumbent computed tomography (CT) is unreliable. Therefore, the horizontal CT (sitting CT) is important for the diagnosis of PET. 33 -36 The open tubal distance was significantly longer in the Valsalva condition than in resting conditions. 33 In resting conditions, sound transmission assessed by sonotubometry is significantly correlated with the positive findings of sitting CT revealing an open ET. 23,32,35 A completely open ET (Figure 6: left) is defined as a patent ET and is observed in 68.6% of definite PET cases. 7 A closed-short (less than 3 mm) ET (Figure 6: middle) is defined as a suspected patent ET.
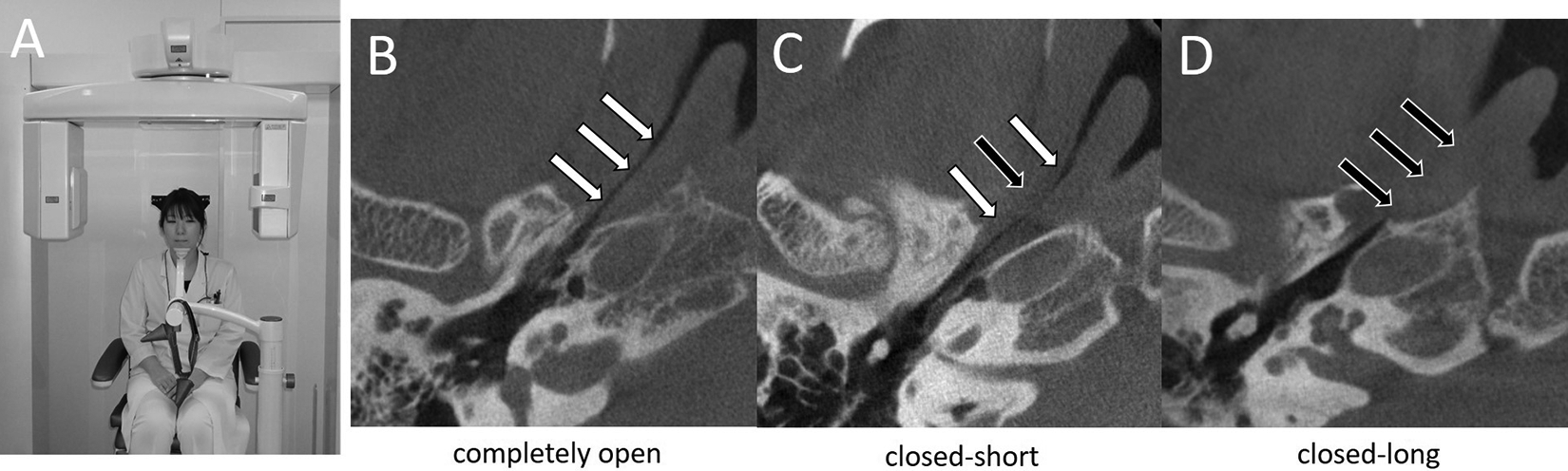
Representative sitting-CT images (axial view) in patients with PET. A, Three-dimensional CT scanner Accuitomo. B, Completely open. C, closed-short (3 mm or less). D, Closed-long (longer than 3 mm). White arrows indicate ET open. Black arrows indicate ET closed. CT indicates computed tomography; ET, Eustachian tube; PET, patulous Eustachian tube.
Magnetic resonance imaging is useful in delineating the ET cartilage and surrounding tissues such as the lateral pterygoid muscle, pterygoid venous plexus, tensor veli palatini muscle, levator veli palatini muscle, and Ostmann fatty tissue. 37,38
Conclusion
We have described the diagnosis of PET based on the diagnostic criteria for PET proposed by the JOS. Patulous ET handicap inventory-10, Ohta method, and sitting CT are also useful for the diagnosis of PET. Further investigation is needed for an accurate diagnosis and precise evaluation of the pathophysiology of this challenging disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by JSPS KAKENHI grant number 15K20175 and 18K16872.