
Abstract
There have been few reports of mature cystic teratoma, also known as a dermoid cyst, in the head and neck. Cervical neck teratoma extending into the mediastinum is also relatively rare. Here, we report a mature teratoma found in a cervical tumor in a 21-year-old man. This is the first reported case of a mature cervical teratoma extending into the anterior mediastinum. A combination of frontal X-ray, ultrasonography, computed tomography, and magnetic resonance imaging indicated a large oval heterogeneous mass surrounding the thyroid gland and trachea, underneath the sternocleidomastoid and sternohyoid, which pressed on the left lobar thyroid and trachea and extended into the anterior mediastinum. Based on preoperative observation, a diagnosis of an embryonal benign tumor was made. Although rare, this case demonstrates that these tumors should be completely removed during workup of cervical tumors.
Introduction
Teratomas are multipotential cell tumors that contain a mixture of multiple germinal layers consisting of ectoderm, mesoderm, and endoderm. 1 They can generally be divided into 2 categories, mature and immature teratomas, which occur at various sites and organs. 2 The occurrence of teratomas in the head and neck region is extremely rare in adulthood, accounting for only 3% of all teratomas, 3 and cervical teratomas extending into the mediastinum are rare. The nasopharynx and neck are the most common sites of disease in the head and neck region, although the sacrococcygeal, ovarian, intrathoracic, testicular, 4 and retroperitoneal regions are also relatively commonly afflicted. 5 Here, we report a rare case of a mature cervical teratoma extending to the anterior mediastinum in an adult.
Case Report
A 21-year-old male patient was admitted to our hospital with a 6-month history of a progressively enlarging painless mass in the left neck, with no other associated symptoms, such as fever, pain, and dyspnea, and with no erythema or tenderness of the overlying skin. Physical examination revealed a soft and elastic mass in the anteroinferior neck that measured 40 × 20 mm. Hematological evaluation, blood chemistry, and thyroid function tests were normal. A frontal X-ray of the chest showed that the cervical trachea was compressed to the right (Figure S1).
Ultrasonography (US) revealed a large oval heterogeneous mass located in the superficial subcutaneous tissue, measuring 61 × 25 mm. The lesion was oval in shape and heterogeneously hyperechoic without evident blood flow signals. In addition, it showed clear contours with strong echo separation which seemed like a large lipoma (Figure S2).
The mass was predominantly hyperintense in T1-weighted magnetic resonance imaging (MRI) scans with a focal hypointense area. After contrast administration, heterogeneous, mainly peripheral, nodular contrast enhancement was observed with a central nonenhancing component. The cystic contents were also hyperintense in T2-weighted images. The tumor surrounded the thyroid gland and trachea, underneath the sternocleidomastoid and sternohyoid, which pressed on the left lobar thyroid and trachea and extended into the anterior mediastinum. Consistent with the results of US, it was a well-defined solid-cystic tumor with mostly cystic mass and partially solid portions, measuring 92 × 26 × 42 mm. A diagnosis of an embryonal benign tumor was made based on the MRI findings (Figure 1 and Figure S3).
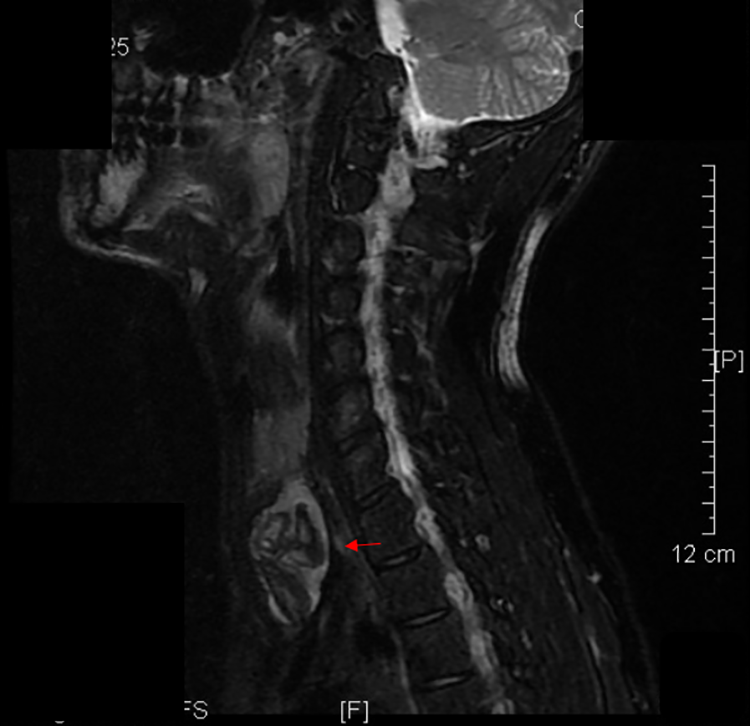
Magnetic resonance imaging showed heterogeneous mainly peripheral nodular contrast enhancement with a central nonenhancing component in sagittal view.
Computed tomography (CT) also revealed a nonhomogeneous mass with fatty tissue, calcified nodes, and variably sized cysts, with well-defined margins measuring 26 × 42 × 96 mm. The lesion compressed the trachea and left lobe of the thyroid to the right anterior side and invaded into the anterior mediastinum, with slight enhancement of its wall (Figure S4). Based on preoperative investigations, we suspected a cervical neck teratoma extending into the anterior mediastinum.
During surgery, we found that the mass compressed and adhered to the internal jugular vein. Using blunt separation and sharp separation, rupture of the jugular vein induced hemorrhage, which was repaired by suturing. After complete removal of the mass, it was found to have extended into the anterior mediastinum. The left recurrent nerve was identified and fully preserved. The whole tumor was removed. The mass had a solid appearance, with grayish-white and yellow areas without immature elements and malignant components. Analyses of tissue sections of the mass revealed that the tumor was a mature teratoma containing hair, yellowish fluid, and a cystic cavity (Figure 2). Histological examination showed that all of the composite elements were mature (Figure 3). The tumor was diagnosed with a mature cystic teratoma (MCT). There were no major complications and the patient was discharged 1 week after the operation. The patient was followed up for about 18 months, with no signs of local recurrence (Figure 4).
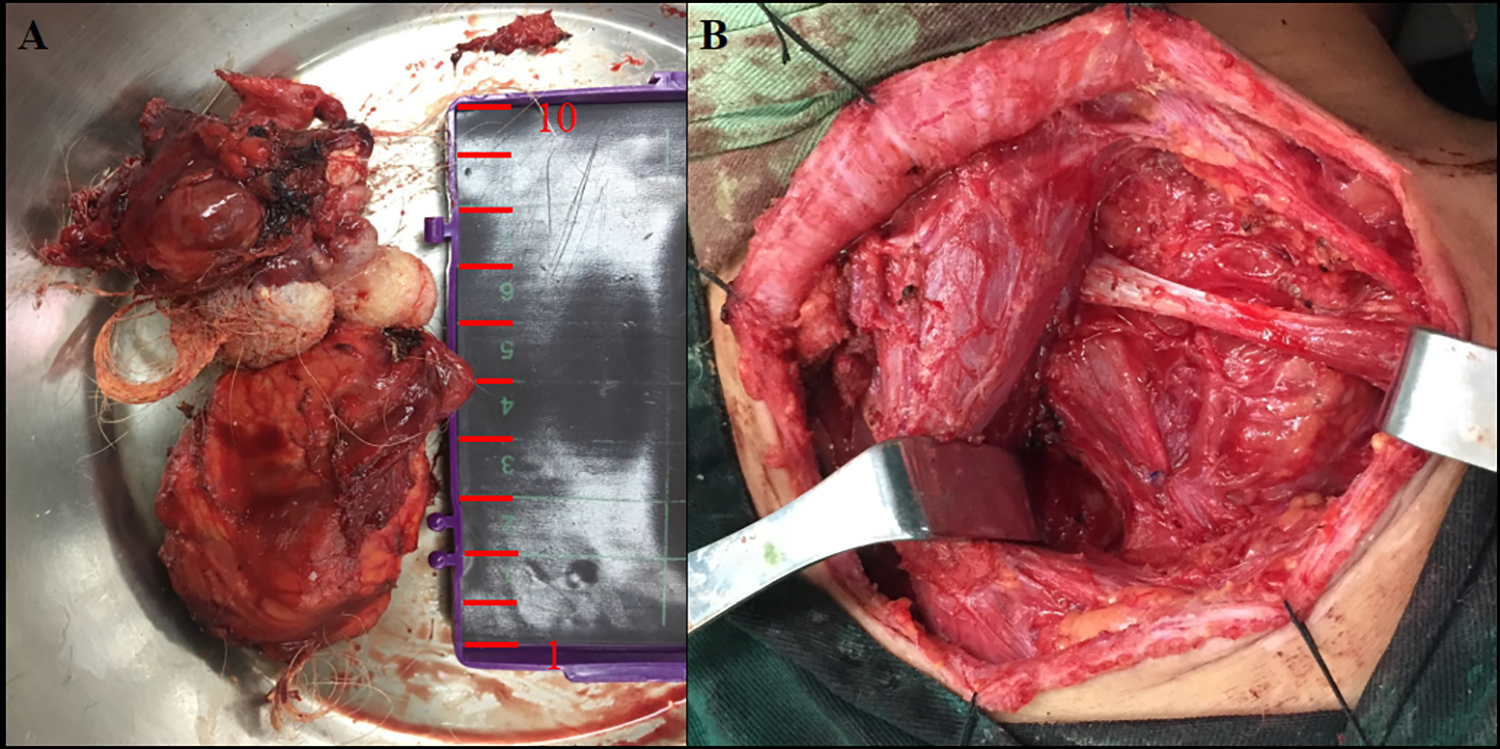
Complete excision of the cervical teratoma extending to the anterior mediastinum showing fatty tissue, hair and osteoid tissue (A). The surgery had good control of shape and depth of incision, thorough hemostasis and coagulation, clean-cut surgery field and slight scars after operation and rinse (B).
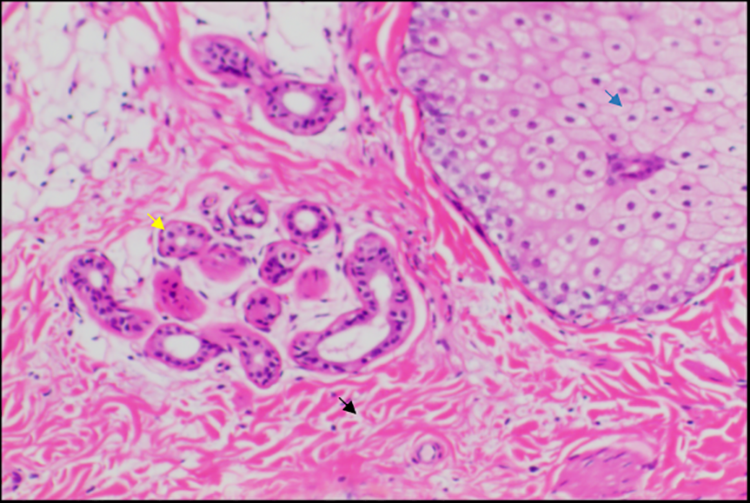
Histological examination revealed collagen fiber (black arrow), perspiratory gland (yellow arrow), pilosebaceous units (blue arrow), stratified squamous epithelium, fatty tissue, or gland and cartilage (Supplemental Figure.5). This tumor was diagnosed as a mature cystic teratoma without malignancy (hematoxylin and eosin stain, ×400).
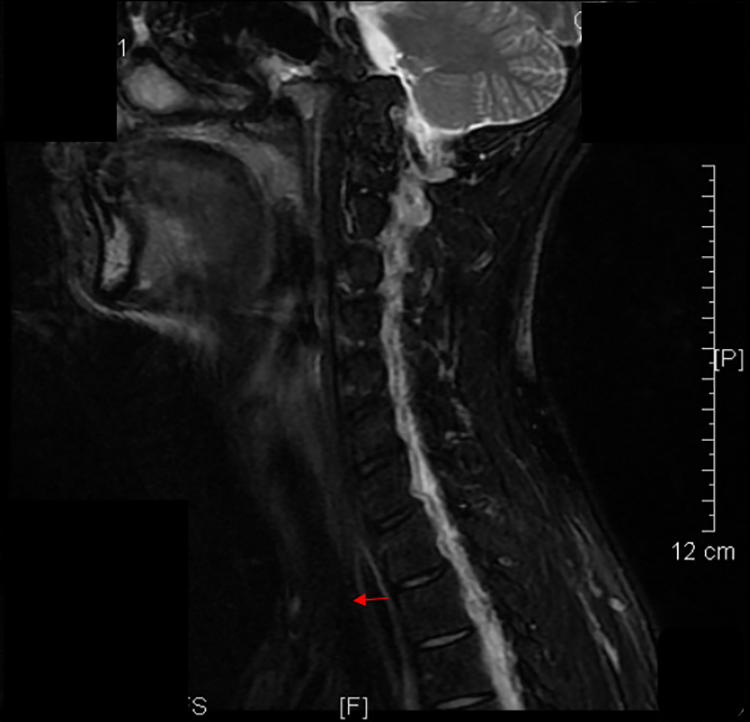
Postoperative MRI showed no occupying lesions, and there was no recurrence in sagittal view. A certain efficacy within 1 year after the observation without recurrence. MRI, indicates magnetic resonance imaging.
Discussion
To the best of our knowledge, this is the first reported case of a cervical teratoma arising in the soft tissue of an adult that extended into the mediastinum. The majority of cervical teratomas arise in neonates or infants, and these lesions are extremely rare in adults, accounting for only 10.6% of all cervical neck teratomas. 6 Moreover, they are highly malignant with very poor prognoses. 3 However, the present case was benign and extended into the anterior mediastinum. This is the first case of a neck teratoma reported to date. However, the lesions also extended into the mediastinum. Therefore, our case expands the possible sites of teratoma expansion, which include the thigh, lumbar region, 1 heart, thyroid, 3 nasal vestibule, 7 and sphenoidal sinus. 8 We suspect that the tumor was a lipoma, dermoid, or epidermoid, as the patient experienced no symptoms other than the mass in the left shoulder region and MRI revealed lipomatous elements in the tumor. We believe that because of the slow growth of the tumor and the gradual compensation, the patient never had any breathing complains. In contrast, there is a case about a massive, right-sided cervical teratoma with occurrence of superior vena cava syndrome and hypoxic ischemic encephalopathy. 9
Magnetic resonance imaging was also very useful for evaluating the relationship between the tumor and the great vessels and vital structures. Therefore, in our case, we mainly obtained an accurate diagnosis preoperatively with CT and MRI. The cystic lesion was likely to be a large expanded teratoma, although we could not determine whether it originated from the anterior, thyroid, or cervical muscles. Only surgery could clarify this situation. Surgical excision is widely accepted as the optimal treatment for cervical teratoma. Proper surgical management, however, relies on establishing the correct clinicoradiological diagnosis. The results of CT and MRI indicated that the teratoma extended into the anterior mediastinum. Therefore, to ensure complete excision, a combination of cervical open surgery was required. However, the tumor was slow growing and encapsulated, so we used blunt separation and sharp separation to carefully remove the tumor from the anterior mediastinum along with completed excision. In our case, it is noteworthy that knowing the anatomical structure, signs, and localization along with careful examination of the CT and MRI results before the operation were important to avoid trauma from combined thoracoscopic surgery.
Unfortunately, we did not test for the markers CA 19-9 and carcinoembryonic antigen, which are elevated in cases of mediastinal mature teratoma. 10
Conclusion
Early surgical excision is the treatment of choice in cases of MCT, and recurrence is rare once complete resection has been achieved. 11 The patient did not show recurrence after almost 18 months of follow-up (Figure 4). Clinicians should be aware of these cystic tumors in the cervical neck region extending into the mediastinum.
Supplemental Material
Supplemental Material, main_document-r1(unmarked) - Mature Cervical Teratoma Extending Into the Anterior Mediastinum of an Adult
Supplemental Material, main_document-r1(unmarked) for Mature Cervical Teratoma Extending Into the Anterior Mediastinum of an Adult by Huiyi Deng, Zhiyuan Wang, Qintai Yang and Jin Ye in Ear, Nose & Throat Journal
Footnotes
Authors’ Note
H.-Y.Deng and Z.-Y.Wang have been contributed equally to this work. As per university standard, the patient’s written consent has been obtained.
Acknowledgments
The authors would like to thank the patient.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Third Affiliated Hospital of Sun Yat-Sen University, Clinical Research Program (No. QHJH201901), the National Natural Science Foundation of China (Grant No. 81670912 and 81870704), and the Industry-Academic Cooperation Foundation of Guangzhou (No. 201704030046) and PROJECT 5010, Sun Yat-sen University (2015005).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.