
Abstract
Background:
Despite different etiologies, chronic otitis media involves the damaging and restructuring of bone tissue. The inflammatory process destroys elements of the ossicular chain, and bone lesions may appear that allow the development of otogenous complications.
Aims/Objectives:
A correlation between the degree of damage to the ossicular chain as well as the bony walls of the middle ear and the type of chronic inflammatory lesions was sought. Destructive changes to bones were observed using scanning microscopy.
Material and Methods:
The removed damaged fragments of the ossicles were prepared for evaluation with a scanning microscope. Preparations were sputter-coated with a thin layer of gold and subsequently evaluated.
Results:
Of 220 surgeries carried out in the discussed period, destruction of the middle ear bone walls, opening the way for the development of intracranial complications, was found in 27 patients. Most of them had ongoing chronic otitis media with granulation.
Conclusions:
(1) Bone loss of the skull base was observed more frequently in patients with chronic otitis media with granulation than with cholesteatoma. (2) In chronic otitis media with cholesteatoma, damage to the ossicular chain was observed significantly more frequently than in the case of otitis media with granulation.
Introduction
The term middle ear describes the air spaces of the temporal bone, including the tympanic cavity, air cells of the mastoid process, and the part of the Eustachian tube located closer to the tympanic cavity, with bony walls. In the above-mentioned spaces, disease processes are observed, most often inflammatory states (acute and chronic). The treatment of acute otitis media is conservative. It is only in cases with complications that surgical treatment is administered.
Chronic otitis media is characterized by tympanic membrane perforation, occasional leakage from the ear and various hearing impairments of a conductive nature. Depending on the observed lesions of the middle ear lining, several types of chronic otitis media may be distinguished: simple chronic otitis media, chronic otitis media with granulation, chronic otitis media with cholesteatoma, and chronic otitis media in the course of specific diseases.
In the course of chronic infection in the middle ear spaces, pathologically changed connective tissue with an expanded set of vessels and the appearance of granulation tissue can be observed. This granulation tissue is modified by inflammatory factors, which are the most typical indicator of chronic middle ear infection. Granulation tissue can be the only feature of infection (chronic otitis media with granulation) or it can coexist with cholesteatoma (chronic otitis media with cholesteatoma and granulation). In rarer cases, only cholesteatoma is observed in the results of histopathological examination (chronic cholesteatoma otitis media).1,2
The treatment of choice in cases of chronic otitis media is surgery.3,4
Chronic suppurative otitis media with cholesteatoma (otitis media purulenta chronica cholesteatomatosa) and to a lesser extent chronic otitis media with granulation (otitis media granulomatosa) lead to the destruction of bone structures within the middle ear area.
Despite their different etiologies, diseases whose course involves damaging and restructuring the bone tissue have a common mechanism at the molecular level that is associated with the RANKL (receptor activator of nuclear factor kappa B ligand)-OPG (osteoprotegerin)-RANK (receptor activator of nuclear factor kappa B) triad. The RANKL-OPG-RANK system is the most important cascade regulating the process of bone destruction.5-7
The ratio of RANKL to OPG has been shown to be higher in cholesteatoma than in a healthy ear. In 2000, Cinamon et al presented a picture of a bone adhering to the mass of cholesteatoma in the form of empty lagoons, ossification bands, eosinophilic vesicles, and a disruption in the continuity of the periosteum. 8
In chronic otitis media with granulation, the pathological granulation tissue contains inflammatory cells, such as T and B lymphocytes, plasma cells, and other cells from the monocyte–macrophage lineage, producing large amounts of pro-inflammatory cytokines (including interleukin [IL]-1α, IL-1β, IL-6, Prostaglandin E2 [PGE2], and tumor necrosis factor [TNF]-α). Studies have shown a significantly elevated RANKL concentration, the main source of which is activated T cells, and a simultaneous reduction in OPG in the granulation tissue adjacent to the bone. The inflammatory process destroys the bony structures of the middle ear and elements of the ossicular chain. The long process of the incus is the quickest to erode.9,10 Bone lesions may appear that allow for the development of intra-temporal (loss in the horizontal semicircular canal and loss in the facial nerve canal) and intracranial (loss in the skull base) complications. The inflammatory process may spread to the labyrinth, onto the sigmoid sinus and cranial cavities. Other ways of developing complications stemming from the ears include through thromboembolic vasculitis and bone tissue inflammation.
Aims/Objectives
A correlation between the degree of damage to the ossicular chain as well as the bony walls of the middle ear and the type of chronic inflammatory lesions was sought.
Destructive changes to bones were observed using scanning microscopy.
Material and Methods
A prospective analysis of 220 patients operated upon for the first time due to chronic otitis media at the Department of Otolaryngology of the Jagiellonian University Medical College during the years 2015 to 2017 was performed. The research group included 120 women and 100 men. The youngest patient was 27 years old, and the oldest was 70.
All the patients underwent a histopathological examination at the Department of Pathomorphological Diagnostics of the University Hospital in Krakow, the result of which determined the final diagnosis. Further analysis was performed for individuals with chronic otitis media with granulation and chronic cholesteatoma otitis media as types of chronic infection with a tendency to lead to bone destruction.
On the basis of defects in the middle ear lining found during surgery and the obtained histopathological results, the patients were divided into 2 groups: Group I—chronic otitis media with granulation, n = 85 Group II—chronic otitis media with cholesteatoma, n = 65
Patients in whom lesions resulting from both granulation and cholesteatoma had been found within the area of the middle ear during the surgery were not analyzed. In all of the examined patients, presurgical examination and diagnostics were carried out, including subject-matter and object-matter otolaryngological examination and a complete set of audiological examinations, including acumetric tests, tuning fork tests, pure-tone threshold audiometry, and speech audiometry.
During the surgical procedure, the degree of damage to bony structures in the middle ear areas was analyzed: damage to the ossicular chain and bone loss in the tympanic cavity walls and the mastoid process. For the purpose of performing a comparative analysis of the degree of damage to the ossicular chain, the changes observed within the auditory ossicles were divided into 3 groups: A: only 1 auditory ossicle damaged B: 2 auditory ossicles damaged C: 3 auditory ossicles damaged
The analyzed damage related to the middle ear wall was divided into: loss in the middle cranial fossa loss in the middle and posterior cranial fossae loss in the posterior cranial fossa loss in the bony canal of the facial nerve canal loss in the lateral semicircular canal
To assess the advancement of the inflammatory process in the middle ear areas, the removed damaged fragments of the ossicles were prepared for evaluation with a scanning microscope using magnifications of 20×, 60×, 300×, and 600×. During the study, a correlation between the degree of damage to the ossicular chain as well as the bony walls of the middle ear border and the type of chronic inflammatory lesions was sought.
Statistical analysis was performed with a significance level of 5%. Statistica software (ANOVA; Statistica, StatSoft) was used for statistical analysis. The multifield contingency tables for patients were taken into consideration, and the χ2 value was determined. The magnitude of the relationship was measured using the Cramer ratio. This result of this test was confirmed using the chi-square test and maximum likelihood estimation. Statistically significant results were reported for P < .05.
Results
The research group included 220 individuals. The youngest patient was 27 years old, and the oldest was 70.
Based on the data collected from the patients’ history, the average duration of disease in individuals admitted to the surgical treatment was estimated to be approximately 4 years. The shortest history of chronic middle ear infection lasted 2 years, and the longest, 15 years. Exacerbation of symptoms and signs may have affected the time taken to visit the otologist and start of treatment.
The degree of damage to the ossicular chain and bony walls of the middle ear in chronic otitis media with granulation and cholesteatoma is presented in Table 1.
The Degree of Damage to the Ossicular Chain and Bony Walls of the Middle Ear in Chronic Otitis Media With Granulation and Cholesteatoma.a
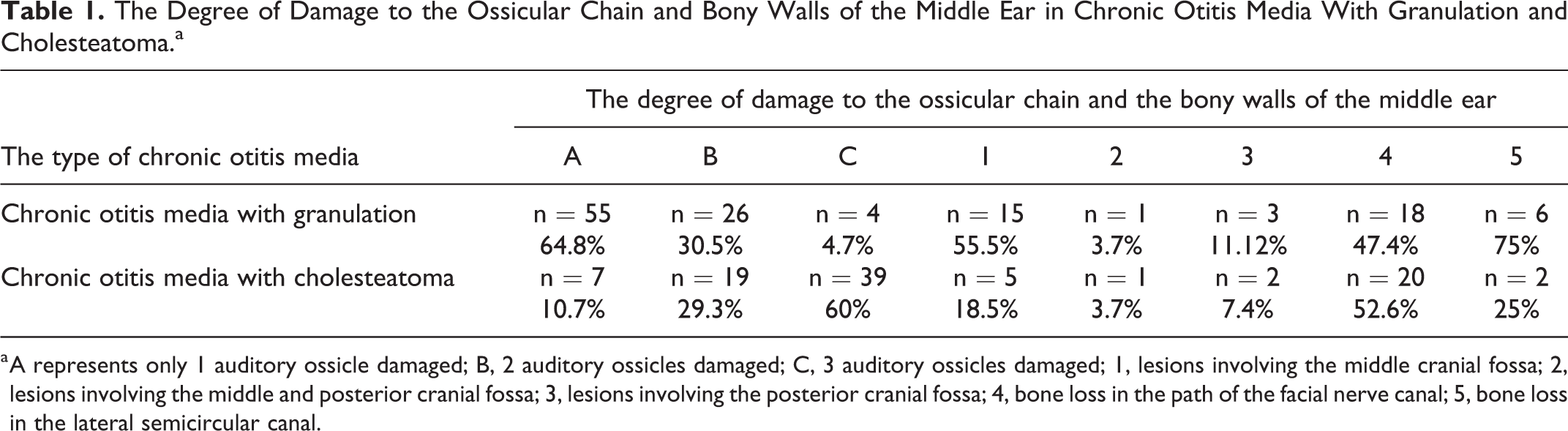
a A represents only 1 auditory ossicle damaged; B, 2 auditory ossicles damaged; C, 3 auditory ossicles damaged; 1, lesions involving the middle cranial fossa; 2, lesions involving the middle and posterior cranial fossa; 3, lesions involving the posterior cranial fossa; 4, bone loss in the path of the facial nerve canal; 5, bone loss in the lateral semicircular canal.
In the assessment via scanning microscopy of group I of patients with chronic otitis media with granulation, destructive changes to bones in the form of singular deep bone losses and an extensive resorption process were observed (20× magnification). A magnification of 60× allowed us to observe an irregular surface with shallow linear bone losses, most likely with small Howship’s lacunae present (Figure 1).
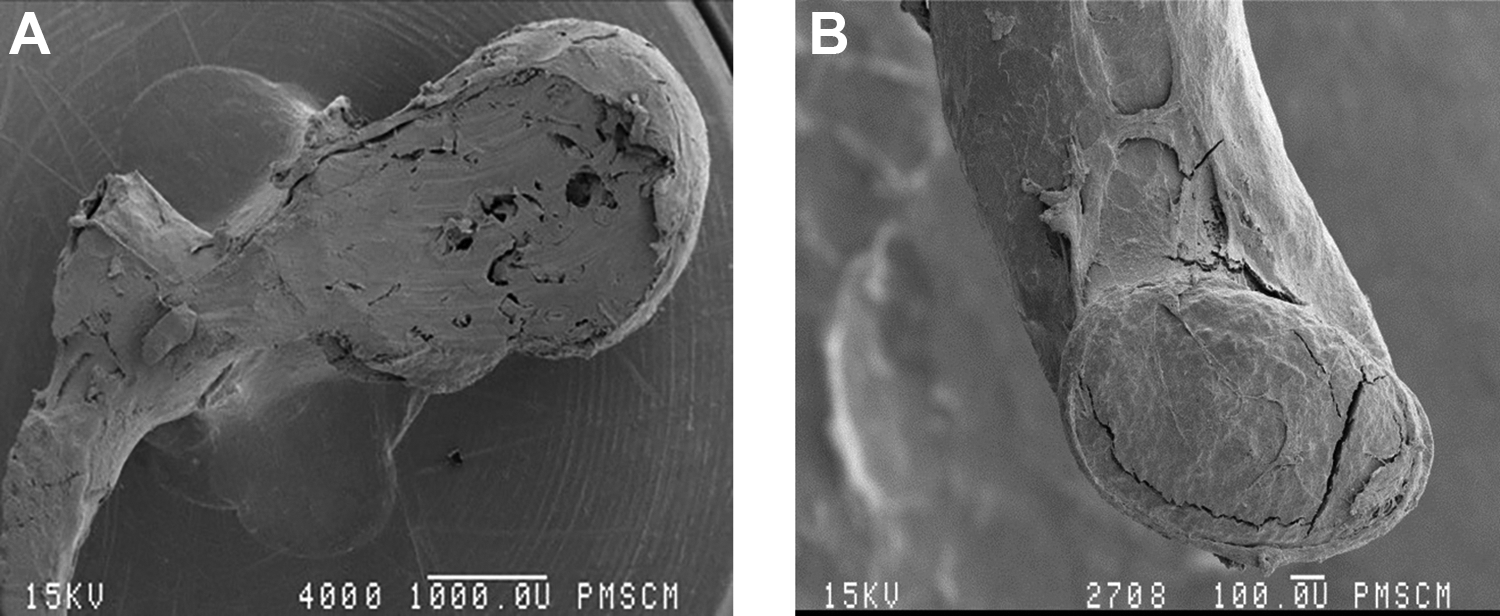
Fragment of a damaged malleus, 20× (A) and 60× (B), chronic otitis media with granulation (workshop of scanning microscopy, Jagiellonian University Medical College, K. Świeży).
The changes observed at a magnification of 600× included lesions in the form of an irregular surface (Figure 2).
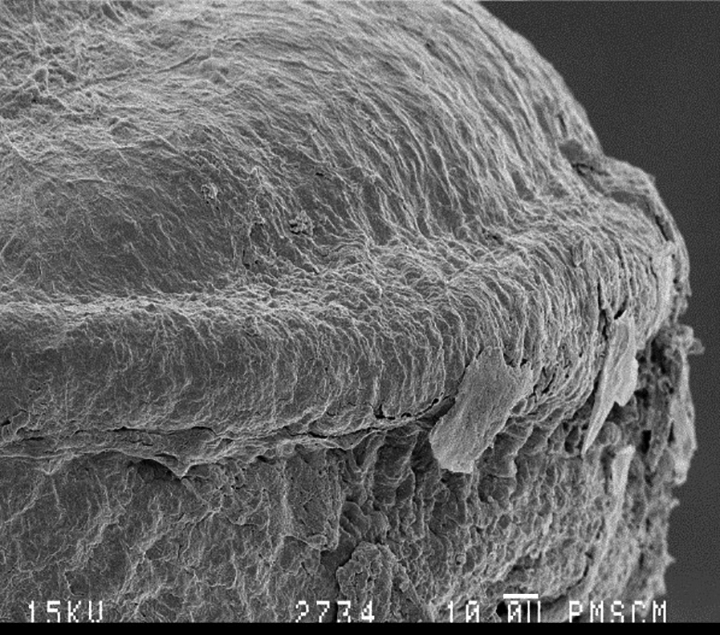
Fragment of a damaged malleus, 600×, chronic otitis media with granulation (workshop of scanning microscopy, Jagiellonian University Medical College, K. Świeży).
The scanning microscope image of fragments of the auditory ossicles showed extensive changes in the form of irregular surface changes with deep linear bone losses and an extensive bone resorption process (Figures 3 and 4).
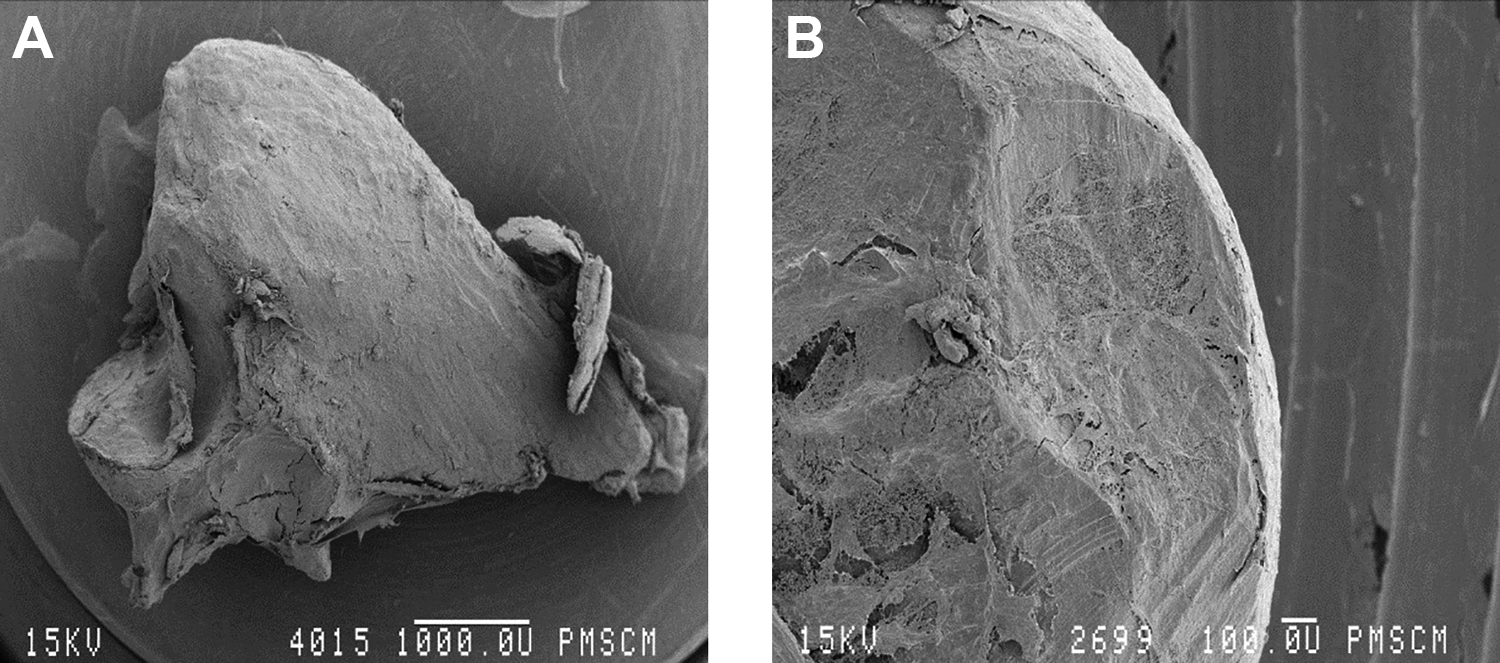
Fragment of a damaged malleus, 20× (A) and 60× (B), chronic cholesteatoma otitis media (workshop of scanning microscopy, Jagiellonian University Medical College, K. Świeży).
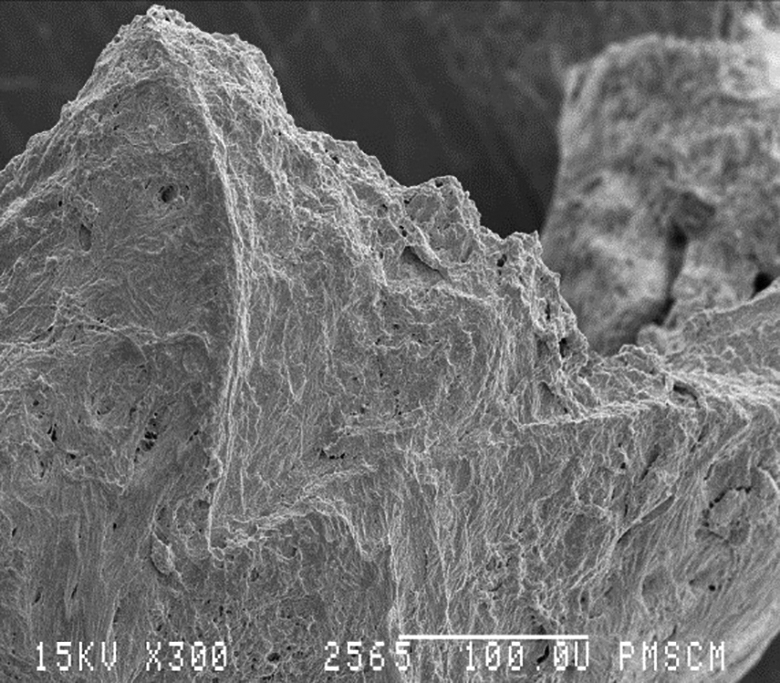
Fragment of a damaged malleus, 300×, chronic cholesteatoma otitis media (workshop of scanning microscopy, Jagiellonian University Medical College, K. Świeży).
Of 220 surgeries carried out in the discussed period, destruction of the middle ear bone walls was found in 27 patients. This accounts for over 12% of the patients operated on due to chronic otitis media. Most of them had ongoing otitis media with granulation (20 cases), and 7 patients had chronic otitis media with cholesteatoma. Most often, there were losses in the bone mass forming the walls of the middle cranial fossa. Losses involving both the middle and the posterior cranial fossa were described in 2 cases, and there were 5 cases of losses that involved only the posterior cranial fossa. The above indicates that chronic otitis media with granulation is an unfavorable prognostic factor at a statistically significant level with regard to the appearance of losses in the base of the skull as a way for intracranial complications stemming from the ears to develop (P < .05).
The most common intracranial complication stemming from the ears was meningitis, found in 4 patients with chronic otitis media with cholesteatoma. Meningitis was observed in 3 patients with bone defects in the base of the middle cranial fossa and 1 patient with defects concurrently in the middle and posterior cranial fossae. Damage to the facial nerve canal was observed in 38 cases. Of these, 47.4% of the losses (n = 18 people) were found in chronic otitis media with granulation, and 52.6% were found in patients with cholesteatoma (20 cases).
The temporal fascia was the material used most often to fill the loss of bone mass in the wall of the base of the skull. In the case of the smallest losses, the treatment consisted of covering the dura with a fragment of the fascia. The fascia was often additionally strengthened with oxycel and Surgicel (Johnson & Johnson) and TachoComb (Takeda). Larger losses were filled by supporting the layer described above with a fragment of cartilage. In the case of more extensive cavities, a pedicled muscle flap was additionally used, which supported the aforementioned structure and at the same time served to obliterate the surgical cavity in the temporal bone. The largest losses, with a diameter of over 1 cm, were filled using 3 layers. The osseous spiral lamina was additionally inserted between the fascia and the pedicled flap described above. This reconstruction was effective and could be carried out simultaneously with the reconstruction of the ossicular chain.
Discussion
Our study showed that inflammatory granulation favors bone defects to the middle ear walls, including losses to the skull base. Analysis of auditory ossicles performed in scanning electron microscope revealed defects to their surface with varying degrees, even if macroscopic appearance of them was within the normal limits. Our analysis indicated it could be the result of direct contact between ossicles and inflammatory lesions. Above observation is compatible with studies of other authors.11,12
Destruction of the bony elements of the middle ear in cholesteatoma is activated and regulated by inflammation. Our observations suggest that inflammation is perhaps the most important factor associated with bone destruction, but it is possible that compression caused by the mass of the cholesteatoma can also play a minor role.13-15 Osteoclasts produced from the monocyte-macrophage lineage are actively involved in resorption of the mineralized bone matrix. The influx of cells is controlled by cytokines, growth factors, adhesion molecules, and osteotropic hormones. The combination of osteoclast and bone matrix occurs with the participation of integrins, which participate in the transfer of signals. A particularly high concentration of αvβ3 integrins has been demonstrated on the surface of osteoclasts.16,17 After joining the surface of a bone, osteoclasts polarize their structure to create 3 morphologically and functionally different areas of the cell membrane: the basolateral membrane, which is rich in integrins and is not in contact with the bone, and a bright adhesion zone and ruffled border, very characteristic of osteoclasts. The adhesion zone is essential for closing the resorptive bay, that is, the space between the ruffled border and the bone, where very low pH values predominate. The fate of the ingredients of bone tissue degraded by osteoclasts, which had previously been unclear, has been explained by the research conducted by Stenbeck and Horton.14,18,19 They described vesicular transcytosis using microtubules from the lysis site, that is, the ruffled border, to the opposite pole of the osteoclast, from which their process takes place. Precursor osteoblast cells have a mesenchymal origin. Osteoblasts synthesize the structural components of the intercellular substance of the bone and regulate the pool of active osteoclasts through the RANKL/OSTEOPROTEGERIN/RANK system. Proresorptive molecules (hormones and cytokines) initiate bone resorption through the induction of RANKL expression on osteoblasts. In inflammation, T lymphocytes become an additional source of RANKL. By joining with the RANK molecule on mature osteoclasts and their precursors, RANKL triggers a cascade of signals leading to the formation of osteoclasts capable of resorbing bone tissue. Osteoprotegerin protects the bone, as it binds to RANKL and thus inhibits the formation and activation of osteoclasts.20,21
Bone destruction combined with the formation of pathological granulation tissue is associated with an increase in T and B lymphocytes, plasma cells, and other cells from the monocytic–macrophage lineage, which produce large amounts of pro-inflammatory cytokines: IL-1α, IL-1β, IL-6, PGE2, and TNF-α. A significant increase in RANKL concentration and decrease in OPG in the granulation tissue adjacent to the bone were demonstrated by Crotti et al.9,22,23
According to the data from the literature, the destruction of the bony wall of the middle ear is observed in approximately 10% of all middle ear operations, and intracranial complications are found in 1% of the total number of patients operated on due to diseases of the middle ear. The patients diagnosed with otitis media chronica cholesteatomatosa (chronic otitis media with cholesteatoma) and otitis media chronica granulomatosa (chronic otitis media with granulation) that undergo operations tend to show the destruction of bone tissue. Destruction of bone elements leads to damage to the ossicular chain and often worse results of surgical treatment in terms of hearing improvement and, as a result of the destruction of the temporal bone walls, constitutes the preliminary stage in the development of intratemporal and intracranial complications.3,4 The observed bone loss within the middle cranial fossa was found almost 3 times more often than in the case of the posterior cranial fossa and the simultaneous bone loss in the middle and posterior cranial fossae. We found that otitis media with cholesteatoma was associated to a lesser extent with exposure of the dura mater of the skull base than with the presence of inflammatory granulation. The destruction of bone structures of the temporal bone in the areas of the middle and/or posterior cranial fossae was usually asymptomatic. Most lesions (80% to 90%) were found accidentally during surgery on the middle ear. This observation emphasizes the importance of imaging tests, especially computed tomography of the temporal bone, in presurgical diagnostics. In the analyzed material, intracranial complications stemming from the ears in the form of meningitis were found in 1.8% of all procedures on the middle ear. These complications were present in the course of chronic cholesteatoma of the middle ear. The degree of damage to the osseous chain in our research depended on the type of inflammation. Extensive, large destructive lesions involving all auditory ossicles were observed in 60% of cases of media otitis with cholesteatoma. The same analysis among patients with chronic otitis media with granulation showed total destruction of the chain in 4.7% of cases. This result was consistent with the results obtained from analyses via scanning microscopy.
This study contained subsequent patients with chronic otitis media admitted to the hospital in order to undergo middle ear surgery. Limitations of the performed study relate to a lack of observation time before surgical therapy. The postponement of otosurgery increases the risk of bone losses and significantly enhances the risk of development of otogenic complications.
Conclusions
Bone loss of the skull base was observed more frequently in patients with chronic otitis media with granulation than among those with cholesteatoma. (2) In chronic otitis media with cholesteatoma, damage to the ossicular chain was observed significantly more frequently than in the case of otitis media with granulation. In otitis media with cholesteatoma, damage to all auditory ossicles was observed the most frequently, and simultaneous destruction of the malleus and incus was observed slightly less frequently.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by statutory funds of the Department of Otolaryngology of the Jagiellonian University, Krakow, Poland.