
Abstract
Objective:
Chronic otitis media is a heterogeneous disorder. Chronic suppurative otitis media with cholesteatoma and, to a lesser extent, chronic otitis media with granulation lead to the destruction of bone structures within the middle ear. Bone loss may appear in the prominence of the horizontal semicircular canals and the bony canal of the facial nerve. The inflammatory process may spread to the bony labyrinth of the sigmoidal sinuses and the cranial cavities.
Materials and Methods:
The analysis comprised the examination of fragments of auditory ossicles removed during surgery in 21 patients with various types of chronic inflammation of the middle ear. The purpose of this study was to evaluate the usefulness of scanning electron microscopy in evaluating the erosion of middle ear ossicles in different types of chronic otitis media. Images captured at various magnifications were used for the best possible illustration of the observed lesions in bone tissue.
Results:
The observed lesions and the degree of bone surface damage were dependent on the type of chronic inflammation of the middle ear. The largest destructive changes in the ossicular chain were observed in chronic otitis media with cholesteatoma; smaller changes were observed in chronic otitis media with granulation.
Conclusion:
In the case of damage to the ossicles inflicted by inflammation, the use of a modeled bone block made of a temporal bone taken from outside the tympanic cavity or a biomaterial prosthesis is a good choice in ossiculoplasty.
Introduction
Chronic otitis media is characterized by loss of the tympanic membrane, occasional otorrhea, and various conductive hearing impairments. The pathogenesis of this disease is complex. At its base is biological worsening of the immunological resistance of the middle ear lining, past bouts of inflammation, the type and resistance of the strain of bacteria causing infection, anatomical conditions of the middle ear pneumatic spaces, and general diseases, such as allergies, immunodeficiency syndromes, and diabetes.
Chronic otitis media is a heterogeneous disorder. In the active form, depending on the observed lesions of the middle ear lining, the following varieties may be distinguished: simple chronic otitis media, chronic otitis media with granulation, chronic otitis media with cholesteatoma, and chronic otitis media in the course of specific diseases.
Chronic suppurative otitis media with cholesteatoma (otitis media purulenta chronica cholesteatomatous) and, to a lesser extent, chronic otitis media with granulation (otitis media granulomatosa) lead to the destruction of bone structures within the middle ear.
The destructive effect of chronic suppurative otitis media with cholesteatoma in the middle ear initially consists of destruction of the ossicular chain through bone resorption. The process of bone resorption in cholesteatoma is initiated by the molecular cascade of osteoclast differentiation factors, which include osteoprotegerin (OPG), receptor activator of nuclear factor κB (RANK), located on osteoclasts, and receptor activator for nuclear factor κB ligand (RANKL), located on the surface of osteoblasts. This system is the most important cascade regulating the process of bone destruction. The long process of the incus is the quickest to erode. Bone loss may appear in the prominence of the horizontal semicircular canals and the bony canal of the facial nerve. The inflammatory process may spread to the bony labyrinth of the sigmoidal sinuses and the cranial cavities.
In chronic otitis media with granulation, the pathological granulation tissue contains inflammatory cells, such as T and B lymphocytes, plasma cells, and other cells from the monocyte–macrophage line, producing large quantities of pro-inflammatory cytokines (including interleukin 1α [IL-1α], IL-1β, IL-6, prostaglandin E2, and tumor necrosis factor α [TNF-α]). Studies have shown significantly increased levels of RANKL, the main source of which is activated T cells, and reduced levels of OPG in the granulation tissue adhering to the bone. The RANKL-OPG-RANK system is crucial in the process of bone resorption in all chronic inflammatory conditions, and the cascade of other inflammatory signals activates, regulates, and supplements the mechanism of the inflammatory process. 1 -5
Materials and Methods
The analysis comprised the examination of fragments of auditory ossicles removed during surgery in 21 patients with various types of chronic inflammation of the middle ear. The fragments of ossicles were not suitable for use as a reconstructive material for the middle ear conduction system or were damaged due to the very advanced inflammatory process.
At the same time, histopathological examination was performed. Based on the clinical state of the middle ear verified during surgery and the obtained histopathological results, all 21 patients participating in the study were divided into 3 groups (Table 1).
Division of Patients Into Groups Depending on the Type of Chronic Inflammation of the Middle Ear.
For the purpose of assessing the structural properties of the middle ear ossicles and the advancement of the inflammatory process, the surgically removed material was fixed in 4% formalin and dehydrated in an ethanol series of 35%, 50%, 75%, 96%, and 99.9% (pure alcohol). Once prepared, the samples were air-dried and mounted on slides using glue (Electrodag 915 Silver Paint; Ted Pella, Redding, California). The prepared samples were sputter-coated with a thin layer of gold using a JEOL JEE-4x device (JEOL JEE-4x; JEOL Vacuum Evaporator, Freising, Germany; Figure 1).

A prepared bone sample sputter-coated with a gold layer for examination by scanning electron microscopy.
Subsequently, analysis of the prepared samples was performed using a JEOL JSM-35CF scanning microscope (JSM-35CF; JEOL Vacuum Evaporator). The degree of damage to the ossicle surface at different magnifications was assessed depending on the type of chronic inflammation. To conduct a comparative analysis of the surface of the examined samples, magnifications of ×36, ×100, ×200, and ×2000 were selected, and the samples in individual groups (I, II, III) were compared.
Informed consent was obtained from each patient included in the study. The local ethics committee approved the study.
Statistical Analysis
In the statistical analysis process, Statistica software was used (StatSoft Polska, Krakow, Poland).
Results
Images captured at various magnifications were obtained for the best possible illustration of the observed lesions in bone tissue. To consolidate the results, scanning electron microscopy (SEM) images obtained at magnifications of ×36, ×100, ×200, and ×2000 were analyzed.
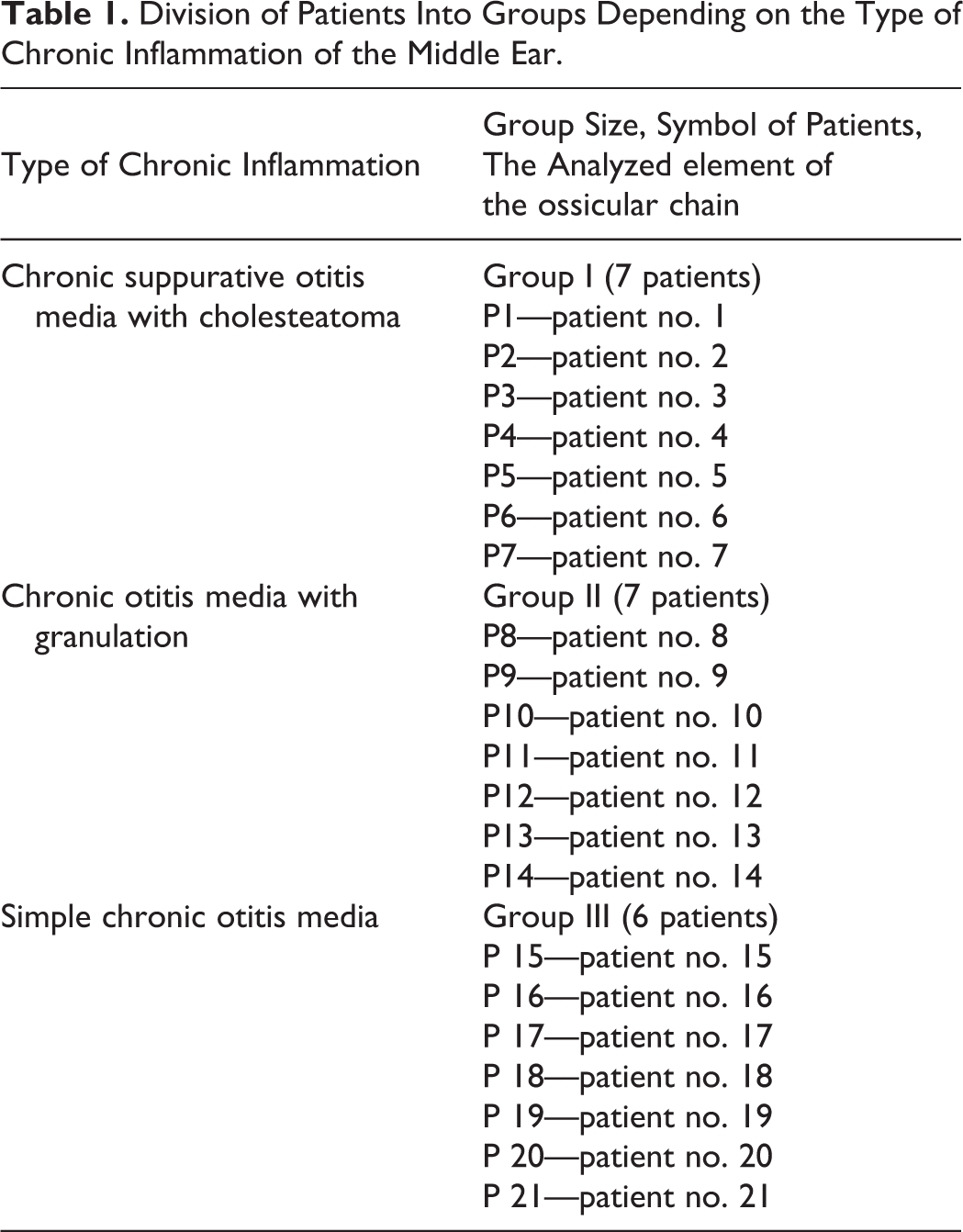
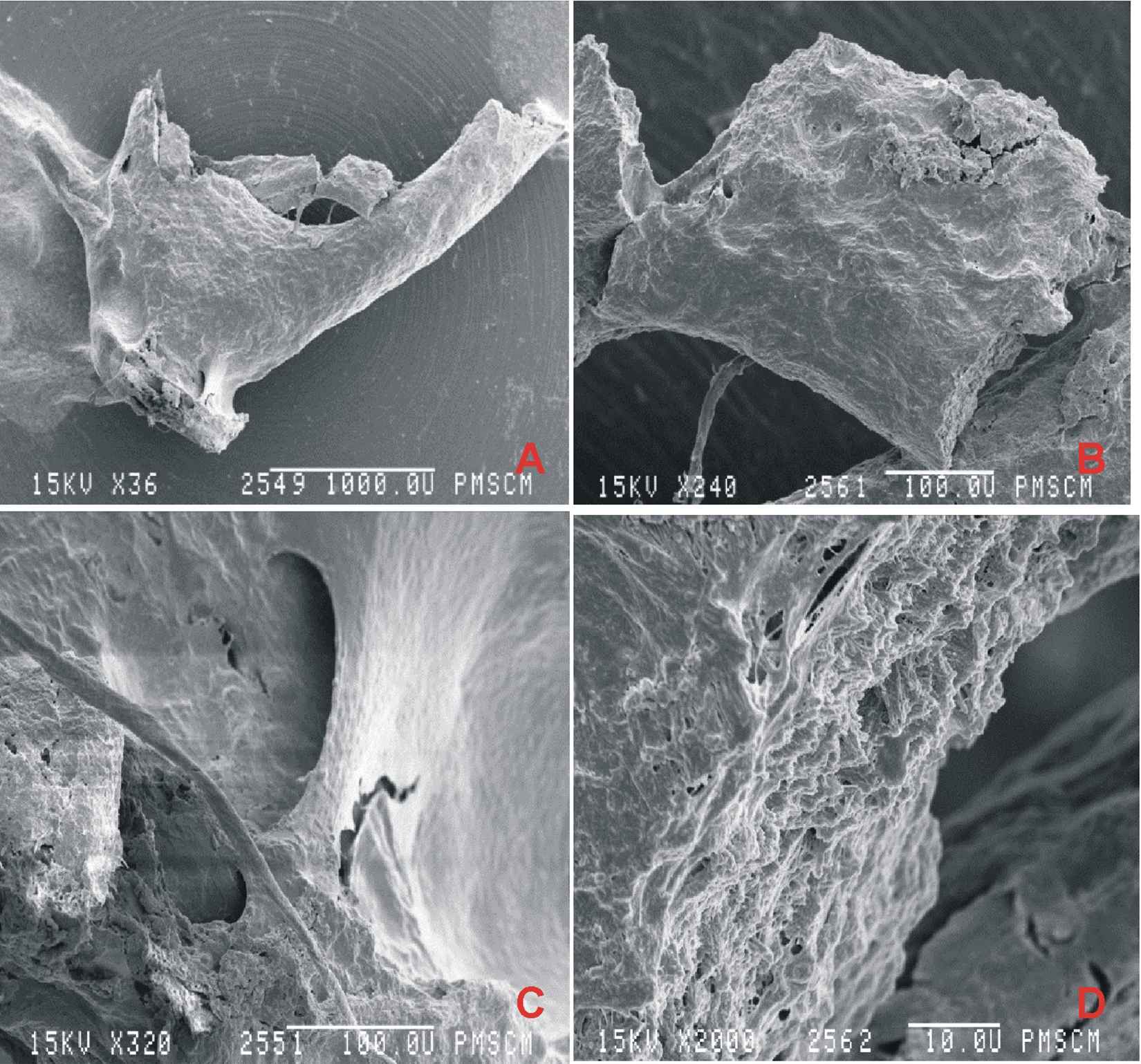
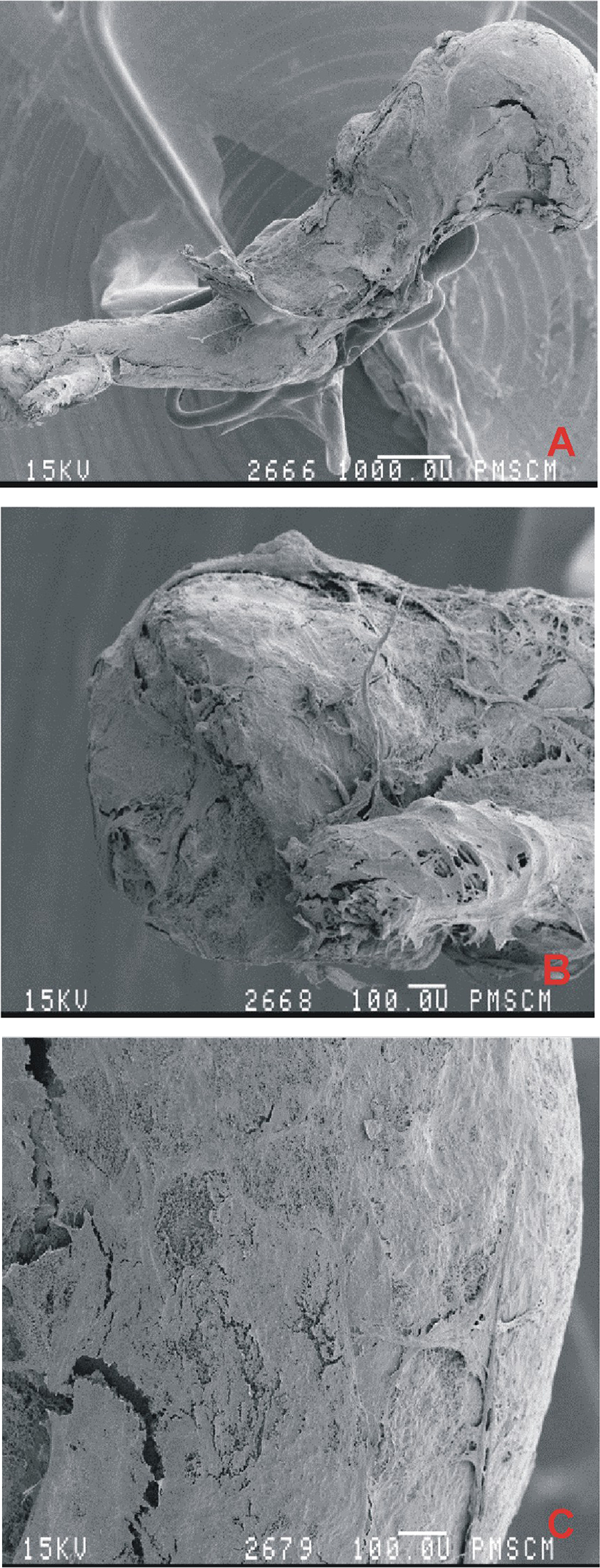
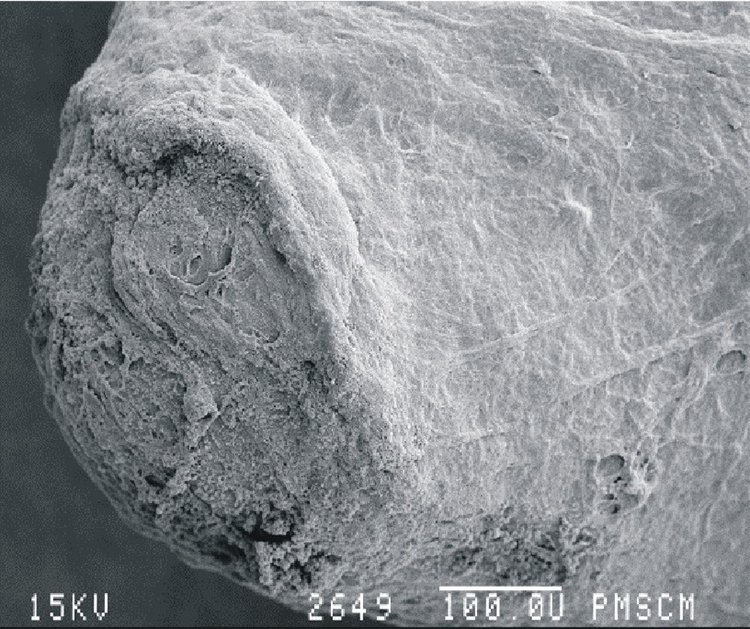
Group I: Chronic suppurative otitis media with cholesteatoma (Figures 2 –4)
Chronic cholesteatoma otitis media. Removed stapes (group I, P1). Scanning electron microscopy showed a fragment of a damaged stirrup (A) ×36, broken anterior crus (B) ×240, vicinity of the stapes’ head (C) ×320, and end of the anterior crus (D) ×2000.
Chronic cholesteatoma otitis media. Removed malleus (group I, P2). Scanning electron microscopy showed a fragment of a damaged malleus (A) ×15, distal part of the malleus handle (B) ×78, head of the malleus (C) ×100.
Chronic cholesteatoma otitis media. Removed incus (group I, P2). Scanning electron microscopy showed a long process ×60 (A), a long process—articular surface ×200 (B). Removed incus (group I, P5). Scanning electron microscopy showed eroded corpus of the incus ×300 (C).
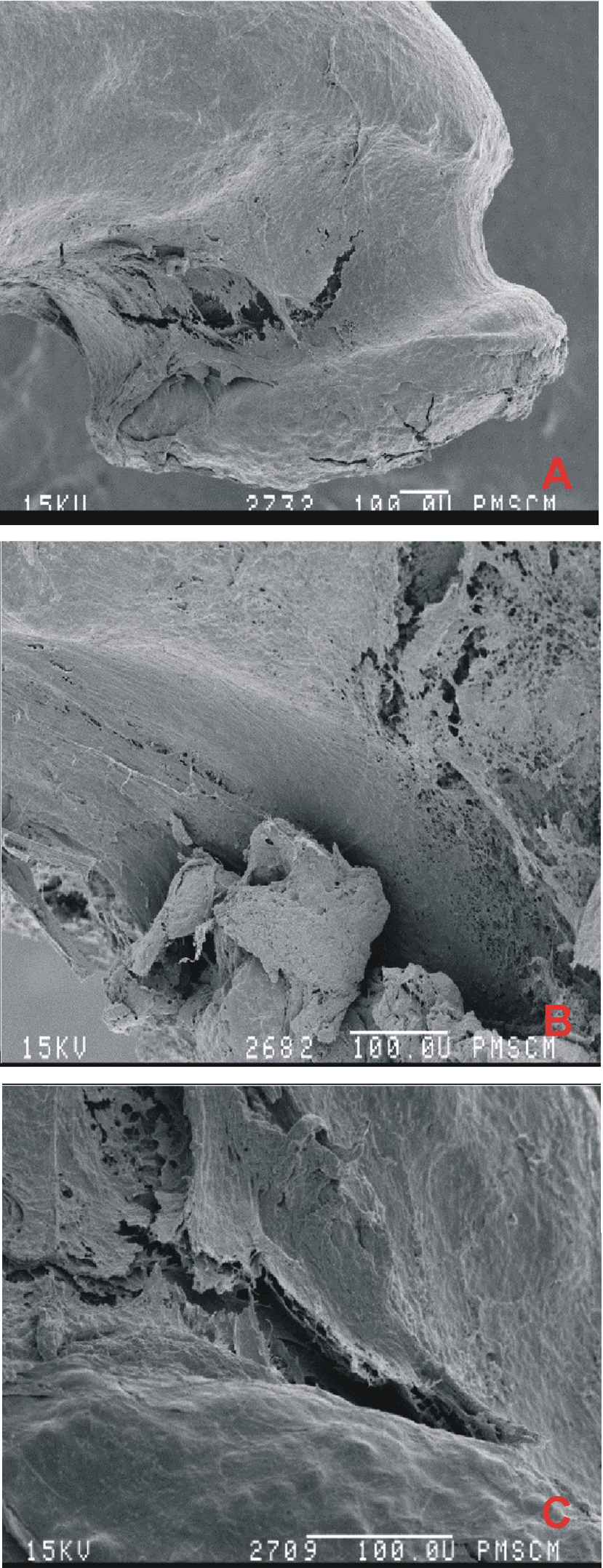
Group II: Chronic otitis media with granulation (Figures 5 -7)
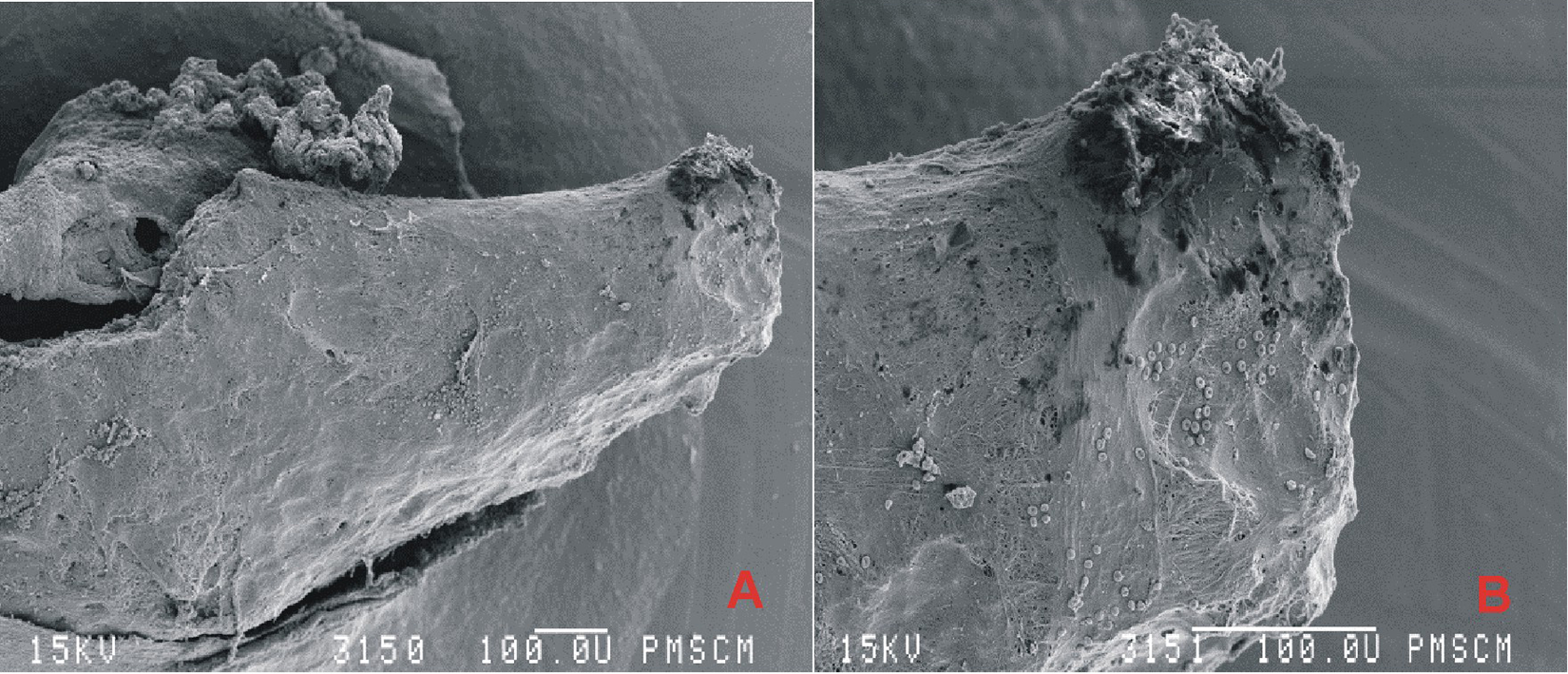
Chronic otitis media with granulation. A fragment of a damaged malleus (group II, P9). Scanning electron microscopy showed eroded handle of the malleus ×110 (A), ×300 (B).
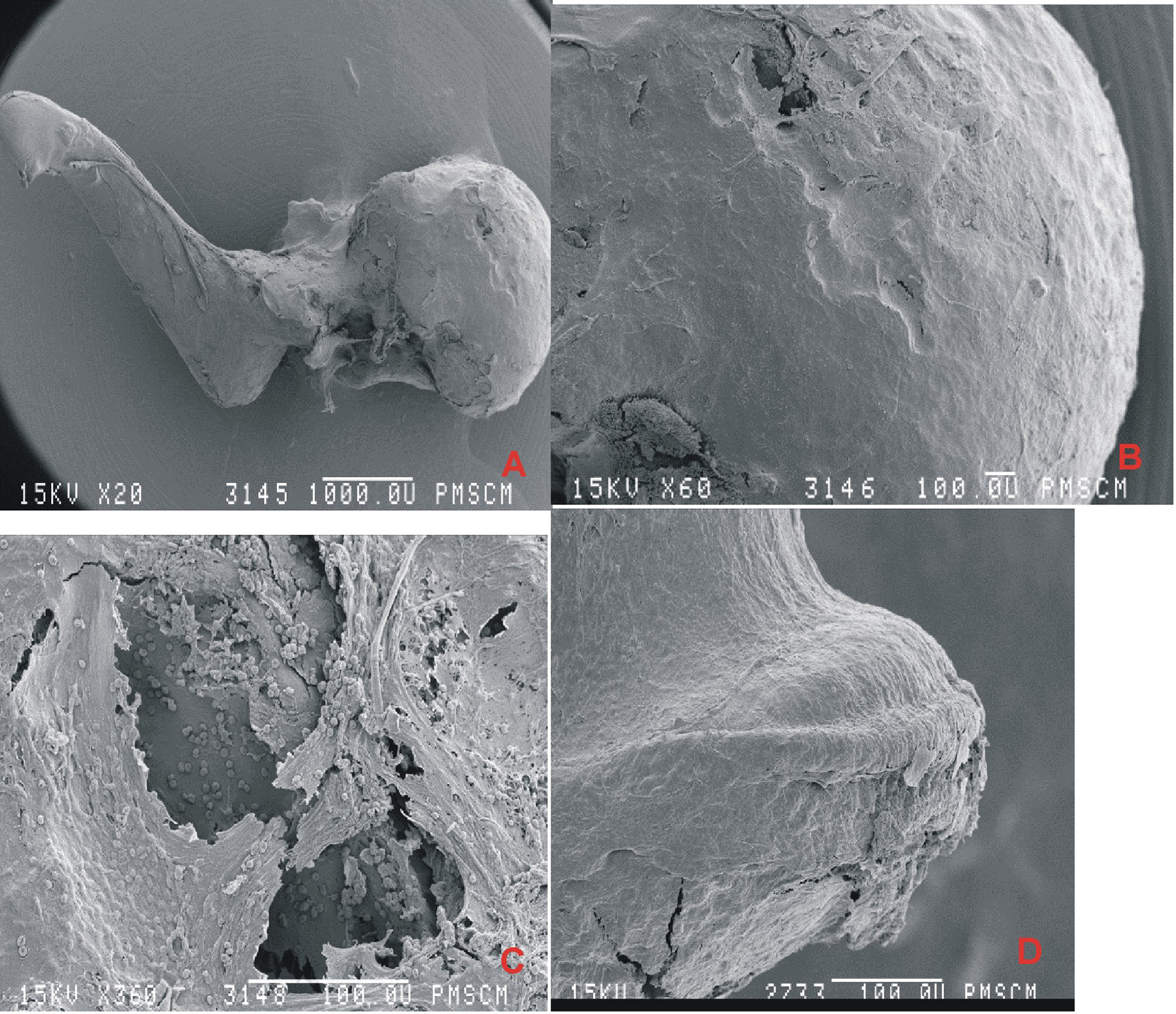
Chronic otitis media with granulation. Removed incus (group II, P11). Scanning electron microscopy showed damaged incus ×20 (A), head of the incus ×60 (B), eroded head of the incus ×360 (C). Removed incus (group II, P14). Scanning electron microscopy showed eroded end of the long process ×160 (D).
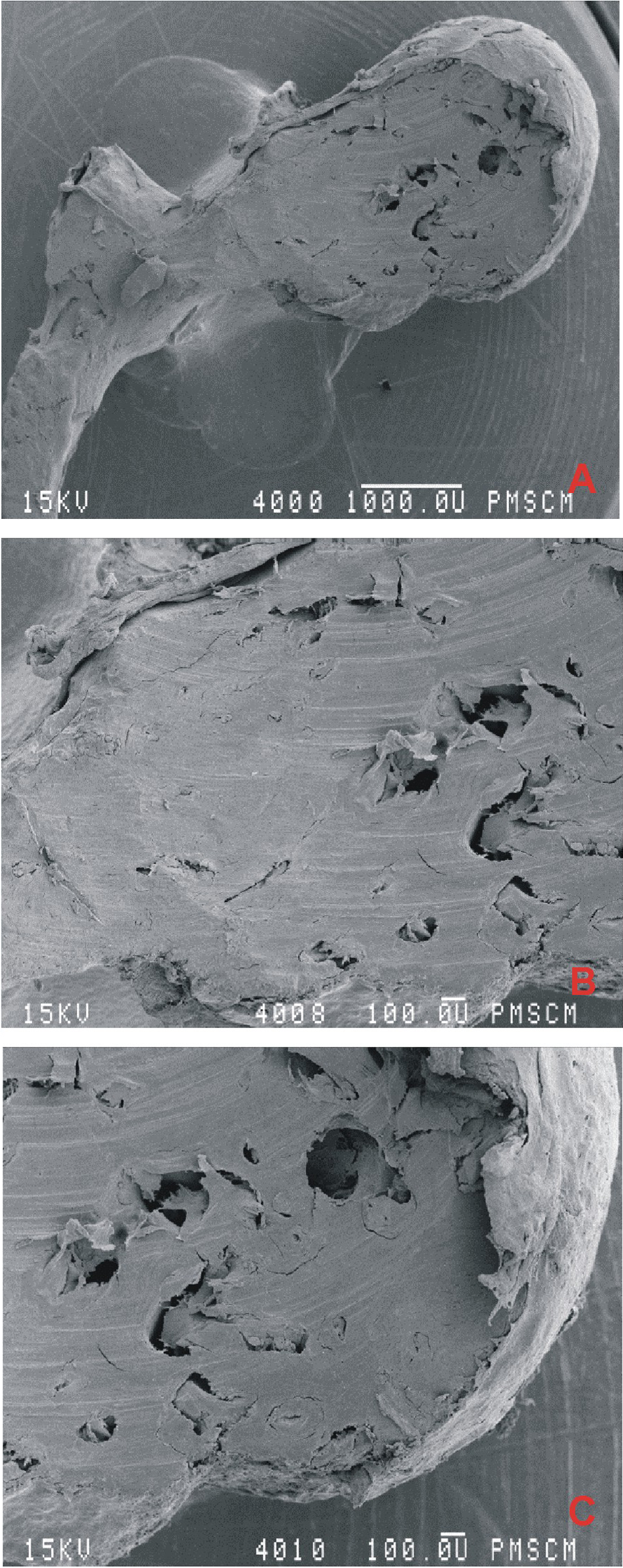
Chronic otitis media with granulation. Removed malleus (group II, P12). Scanning electron microscopy showed eroded malleus head ×20 (A), ×48 (B), ×48 (C).
Group III: Simple chronic otitis media (Figures 8 –10)
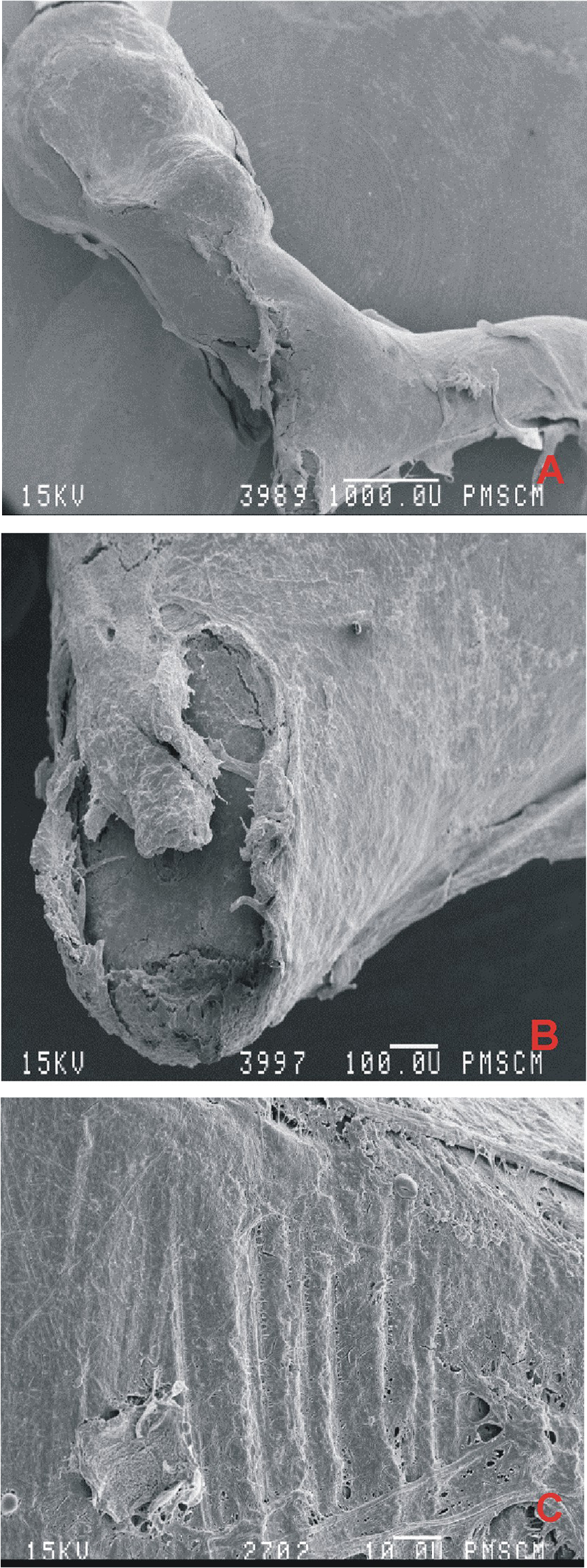
Simple chronic otitis media. Removed malleus (group III, P17). Scanning electron microscopy showed damaged malleus ×20 (A), eroded lateral process ×100 (B), eroded malleus surface ×200 (C).
Simple chronic otitis media. Removed hammer (group III, P18). Scanning electron microscopy showed eroded short process ×200.
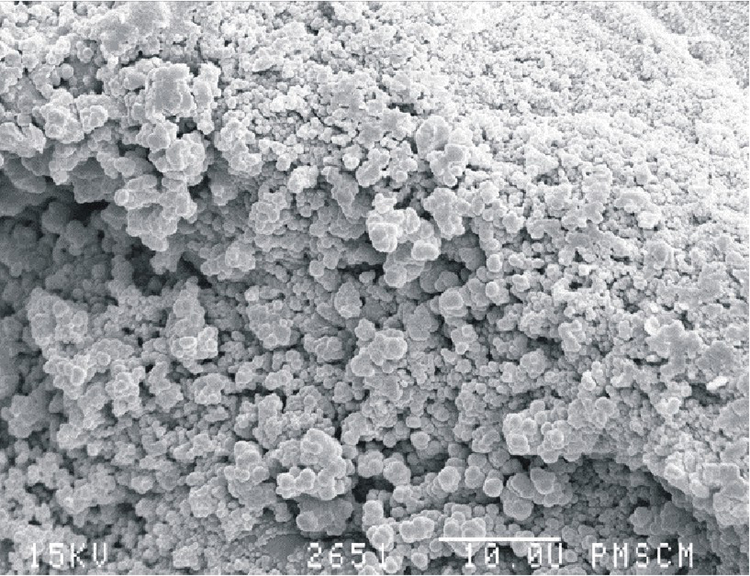
Simple chronic otitis media. Removed hammer (group III, P18). Scanning electron microscopy showed biofilm colonization ×2000.
The observed lesions and the degree of bone surface damage are summarized in Table 2 to compare bone damage depending on the type of chronic inflammation of the middle ear.
Lesions and Damage to the Surface of the Examined Ossicles Observed by Scanning Electron Microscopy.
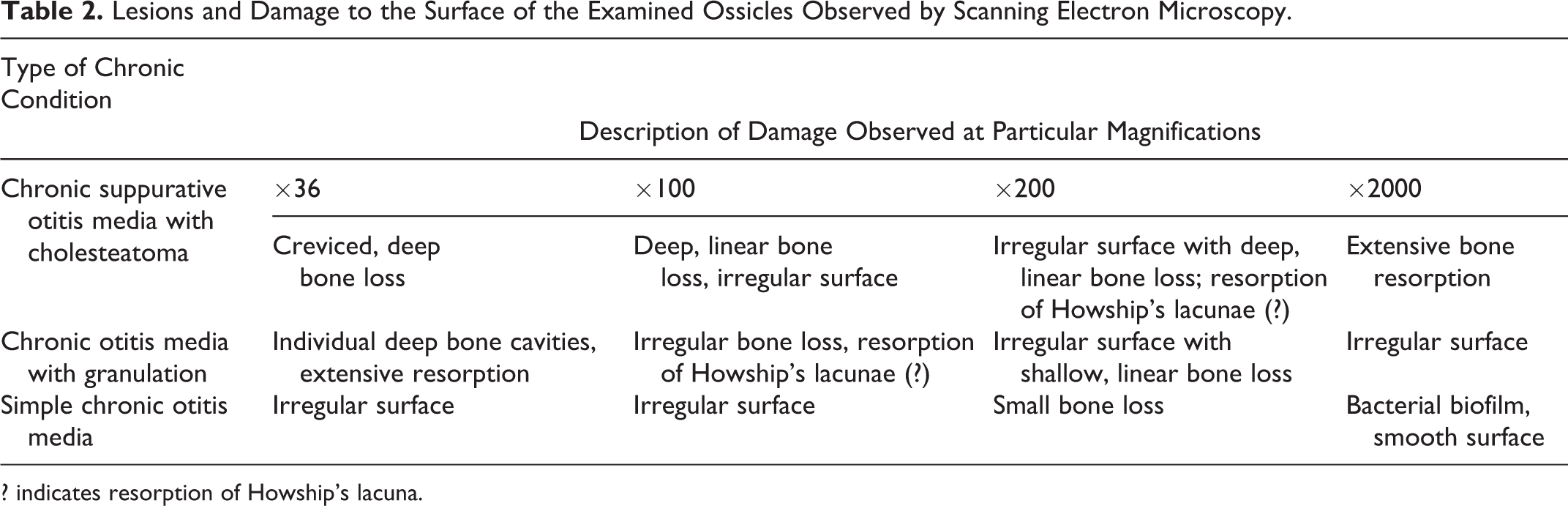
? indicates resorption of Howship’s lacuna.
Discussion
The process of resorption and reconstruction in chronic inflammation of the middle ear is responsible for lesions in bone tissue of the ossicular chain. Remodeling and reconstruction are based on the cyclical processes of bone resorption and formation occurring one after the other, activated and modified by a number of inflammatory factors. The degree of bone tissue damage largely depends on the type of chronic inflammation, its duration and the extent of inflammatory lesions, or the etiology of inflammation (bacterial, fungal). The greatest damage is observed, which is consistent with our observations, in the case of cholesteatoma of the middle ear. Research to explain the mechanisms of soft tissue and bone damage in this type of inflammation was undertaken by Virchow, who, at the end of 1864, was the first to show the destructive effect of cholesteatoma on bone. The expansive effect of cholesteatoma causing bone destruction via the mechanism of pressure and thus bone destruction was supported in 1951 by Walsh. 6 This theory was overturned in 1987 after studies by Orisek and Chole, 7 who showed that the pressure in the capillaries under the cholesteatoma varied from 1.3 to 11.9 mm Hg (normal: 25 mm Hg). Thomsen et al 8 and Chole 9 have shown that acid phosphatase is responsible for bone resorption in cholesteatoma, and lowering the pH promotes the demineralization of hydroxyapatite. Moriyama et al 10 have found that cholesteatoma induces bone resorption by altering the electrical potential of the environment and causing the accumulation of monocytes in subepithelial areas. The destructive effect of cathepsin D on bone was shown in 2002 by Chodynicki et al. 11 Based on this research, the most likely mechanism responsible for the process of bone resorption in cholesteatoma is the molecular cascade of osteoclast differentiation factors, which consist of OPG, the RANK (a protein belonging to the family of TNF receptors, regulated by IL-4 and transforming growth factor beta in T and cluster of differentiation 40 + lymphocytes), and the RANKL (a cytokine in the TNF family), forming the so-called OPG-RANKL-RANK triad. Osteoprotegerin, by binding with the RANKL protein, prevents binding with the RANK receptor and thus blocks the process of osteoclast maturation. The ratio of RANKL to OPG has been shown to be higher in cases of cholesteatoma than in a healthy ear. In 2000, Cinamon et al 12 presented an image of a bone adhering to the mass of cholesteatoma in the form of empty lagoons, ossification bands, eosinophilic vesicles, and periosteal continuity disorders. In the mechanism of bone tissue damage in chronic otitis media with granulation, major roles are played by IL-1α, TNF-α, and serine proteases, as well as the OPG-RANKL-RANK triad to a lesser extent, and the cascade of bone destruction, as in the case of chronic cholesteatoma of the middle ear, consists of several stages; however, it seems to be less complicated than that in the bone destruction process described above. Nevertheless, there have been no detailed analyses, such as works on chronic otitis media with cholesteatoma. In all of the analyzed fragments of ossicles, we observed lesions and remodeling that indicate ongoing chronic inflammation. The largest changes were observed in cholesteatoma of the middle ear, where none of the analyzed ossicles were suitable for use in reconstruction of the middle ear conduction system. The lesions reached deep into the bone matrix and were observed at the highest magnifications (×2000 and ×4000). We observed smaller lesions in chronic otitis media with granulation; however, the damage disqualified the possibility of using the material for reconstruction in these cases as well. The smallest lesions in the osseous tissue of the ossicles were observed in simple otitis media.
This study unequivocally shows superficial microdestruction of the ossicles observed by SEM even if the appearance under the surgical microscope was unchanged in patients with chronic cholesteatomatous otitis media. The above relationship was especially visible if the elements of the ossicular chain had close contact with a cholesteatoma lesion. Destruction to the surface of the ossicles prevents their use as a reconstructive material ossiculoplasty. Direct adhesion of the cholesteatoma to the ossicular chain seems to disturb the structure of the ossicles and change their features; thus, their use in tympanoplasty is controversial. Because of the different methods of preparing surgical specimens for SEM analysis, it is not possible to compare the presented results to those of previous studies by other authors. 13,14
Conclusions
Chronic inflammation involving the ossicles destroys individual elements of the auditory ossicular chain to various degrees, often preventing their use as a reconstructive material, despite their suitable macroscopic appearance.
The largest destructive changes in the ossicular chain were observed in chronic otitis media with cholesteatoma; smaller changes were observed in chronic otitis media with granulation. The process of bone destruction also occurs in simple chronic otitis media to a small degree.
In cases of severe damage to the ossicles inflicted by the inflammatory process, in ossiculoplasty, the otosurgeon should use material taken from outside the tympanic cavity (eg, modeled bone block made of a temporal bone) or an artificial prosthesis (eg, made of titanium or a biomaterial).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by statutory funds of the Department of Otolaryngology of the Jagiellonian University, Krakow, Poland.