
Abstract
Objectives:
(1) To investigate the state of diversity and inclusion initiatives in otolaryngology–head and neck surgery (OHNS) as compared to general surgery and (2) assess their effects on female representation in these programs.
Methods:
The websites of OHNS residency programs, general surgery residency programs, and their associated academic medical institutions were indexed for content related to diversity and inclusion (D&I) initiatives. Gender data were gathered and used as a proxy for identity diversity.
Results:
All programs surveyed (N = 198) have D&I programs at the institutional level and have an office of D&I (or equivalent program). However, only 18% of general surgery programs and 19% of otolaryngology programs have additional department-level D&I initiatives. There was an increase in the proportion of female residents across all residency programs if the program mentioned D&I on their website (44% vs 38%, P = .004) and if the program reported a D&I initiative (45% vs 38%, P < .001).
Conclusion:
Despite the ACGME’s recent emphasis on the importance of recruiting and retaining a diverse physician workforce, the minority of otolaryngology residency programs advertise any concerted, department-level efforts toward increasing D&I at their residency program. General surgery programs have a significantly higher proportion of female department chairs and higher mean proportion of female residents when compared to OHNS. Programs that mention the diversity of their residents or faculty on the program website and programs with their own D&I initiatives have a higher mean proportion of female residents.
Introduction
The United States is a rich, multicultural, multiethnic tapestry growing more diverse daily. Minority populations in the United States are increasing, with non-Hispanic whites projected to be a minority by 2045. 1 This diversity outpaces that of the medical workforce to the detriment of patients.2-16 Although black and Hispanic Americans represent roughly 13.4% and 18.1% of the US population, respectively, they make up only 6.3% and 5.1% of enrolled US medical students. 17 Increasing gender, racial, ethnic, and cognitive diversity of the medical workforce is paramount to serve increasingly diverse populations. The Accreditation Council for Graduate Medical Education (ACGME) recognizes this, mandating as of July 2019 that programs “engage in practices that focus on mission-driven, ongoing, systematic recruitment and retention of a diverse and inclusive workforce” as part of their “Common Program Requirements. 18 Adopting these practices is critically important in otolaryngology. Otolaryngology consistently ranks near the bottom in gender and ethnic diversity compared to other subspecialties.19,20 Despite modest gains in recent years, 19 women and underrepresented minorities (URMs) still experience lack of advancement into leadership positions in medicine at large,21-26 and in otolaryngology specifically.27-29
Two noteworthy efforts have attempted to diversify the ethnic, racial, and gender composition of medical trainees and faculty. The first is the Sullivan Commission, 30 which was established in April 2003 by the Duke University School of Medicine. This commission sought to “make policy recommendations to bring about systemic change that will address the scarcity of minorities in our health profession.” However, there have been no reports on the effects of these recommendations. Assessments of these recommendations is difficult, as they primarily speak to health systems-level changes and don’t address residency program-level diversity and inclusion (D&I) initiatives. The second is a 10-year diversity initiative to increase the number of women and URMs in the Department of Otolaryngology–Head and Neck Surgery (OHNS) at Johns Hopkins University. This multifaceted endeavor successfully increased representation for women and URMs in their department. 31
To date, little research has been done to characterize the number and extent of D&I initiatives promoted on residency program websites and their impact on the proportions of women in otolaryngology training. The primary objective of this study was to evaluate the prevalence of D&I language on program websites and the presence or absence of D&I initiatives. The secondary objective was to determine if the presence of D&I initiatives, on either departmental- or institutional-level web pages, impacts the gender diversity of faculty and/or trainees at the associated residency programs. General surgery programs at these same institutions were used as comparators.
Methods
Ethical Approval
This study is an analysis of publicly available information from residency program websites and does not qualify as human subjects research.
Definitions
Gender representation of OHNS and general surgery faculty members and residents was captured from departmental websites from June 1, 2019, to June 21, 2019. We did not gather race or ethnicity data from faculty profiles on program websites as these are self-ascribed traits. Furthermore, surveying all otolaryngology faculty and residents is neither practical nor likely to result in survey response levels sufficient for meaningful conclusions. Gender, determined by reviewing faculty portraits and pronouns in faculty biographies, serves as a proxy in our understanding of the current state of diversity in otolaryngology.
Program-Specific Diversity Initiative Data Sources
Residency programs were identified using the ACGME’s “List of Programs by Specialty,” which identified 109 allopathic residency programs for OHNS. Each program’s website was reviewed for the presence of language regarding D&I (Table 1) and other program characteristics such as the presence of pipeline or mentorship programs, diversity benchmarks, and availability of research and away rotation funding for women and URMs. “Pipeline programs” are designed to provide educational and career support to trainees with ethnic or racial minority backgrounds and/or other challenges entering medical training programs. Residency programs were considered to have diversity benchmarks if they articulated clear, specific, measurable goals related to improving D&I.
Examples of Diversity and Inclusion Language From Program Websites.
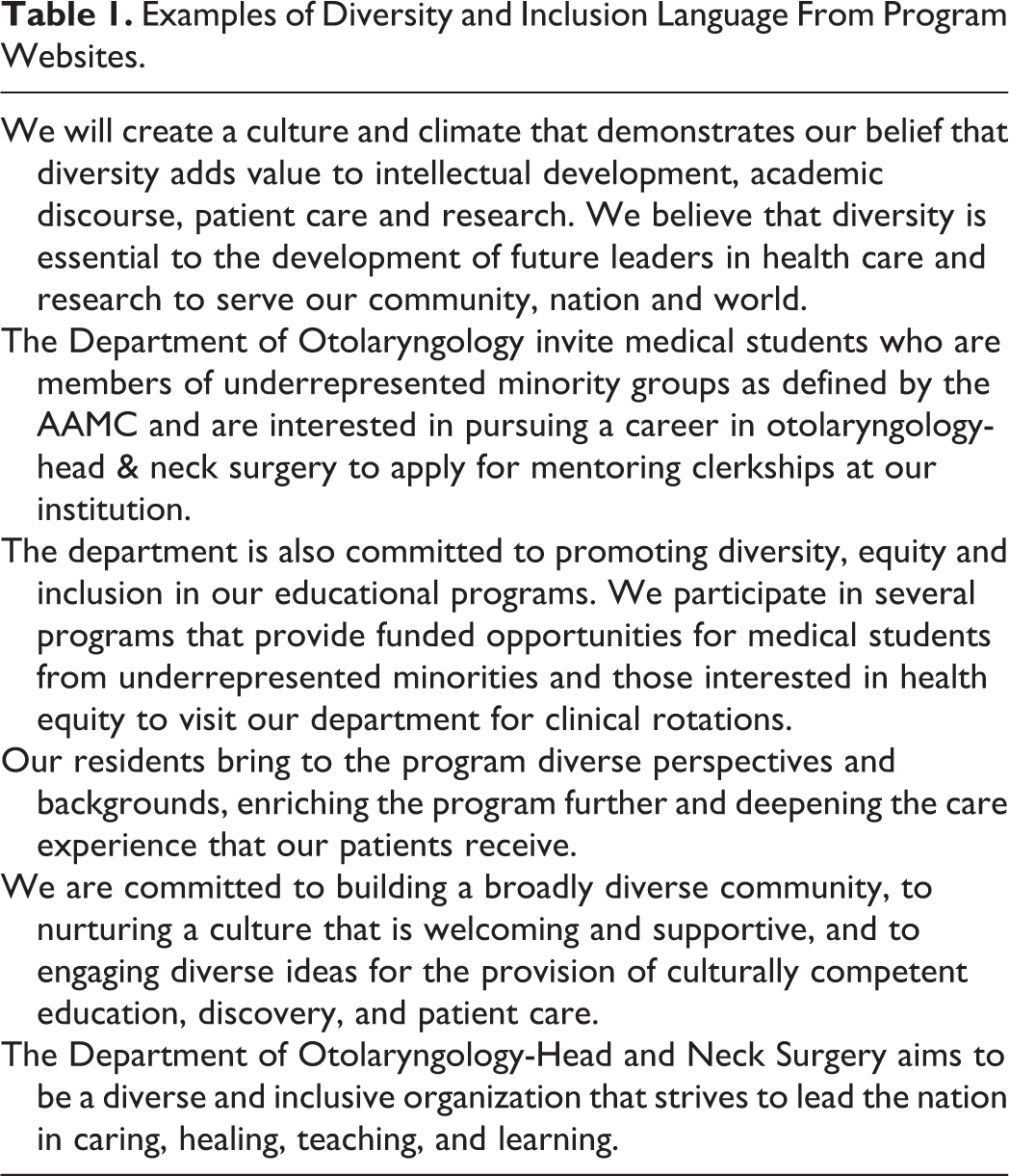
We also looked for D&I language on university and school of medicine web pages. Excerpts of representative D&I language are provided in Table 1. In the interest of accurately characterizing the state of gender equity in otolaryngology and general surgery, numbers on otolaryngology faculty members reflect only MD (or equivalent degree, eg, MBBS) clinical faculty and do not include research faculty, audiologists, speech and language pathologists, or other providers.
Inclusion/Exclusion Criteria
Programs included for study are all ACGME accredited, allopathic, civilian otolaryngology residency programs, and their comparator general surgery programs from the same institution. Programs were excluded if they were not ACGME accredited, were exclusively military match programs, or did not have a comparator general surgery program.
Statistical Analysis
Statistical analysis was performed using SPSS Statistics (version 25.0; IBM Corporation, Armonk, New York). Descriptive statistics including proportions were calculated to compare programs across specialties by gender and according to the presence of D&I programing. Statistical comparisons of these proportions were performed using χ2 or Fisher exact tests as appropriate. Statistical significance was established a priori at α = .05.
Results
One hundred nine unique allopathic otolaryngology residency programs were identified. Of these programs, 6 programs were identified as participating exclusively in the military match and were excluded. Three programs did not have a matching general surgery program for comparison and were excluded. One program did not have enough data available on the Internet to be included for analysis. The websites of the remaining 99 otolaryngology residency programs and their matching general surgery programs were reviewed. Program characteristics and prevalence of D&I programs are given in Table 2. Regarding D&I programming, general surgery residency programs and otolaryngology residency programs were statistically similar. General surgery programs had a higher mean proportion of female residents and more female department chairs.
Program Characteristics and Diversity and Inclusion Programs.
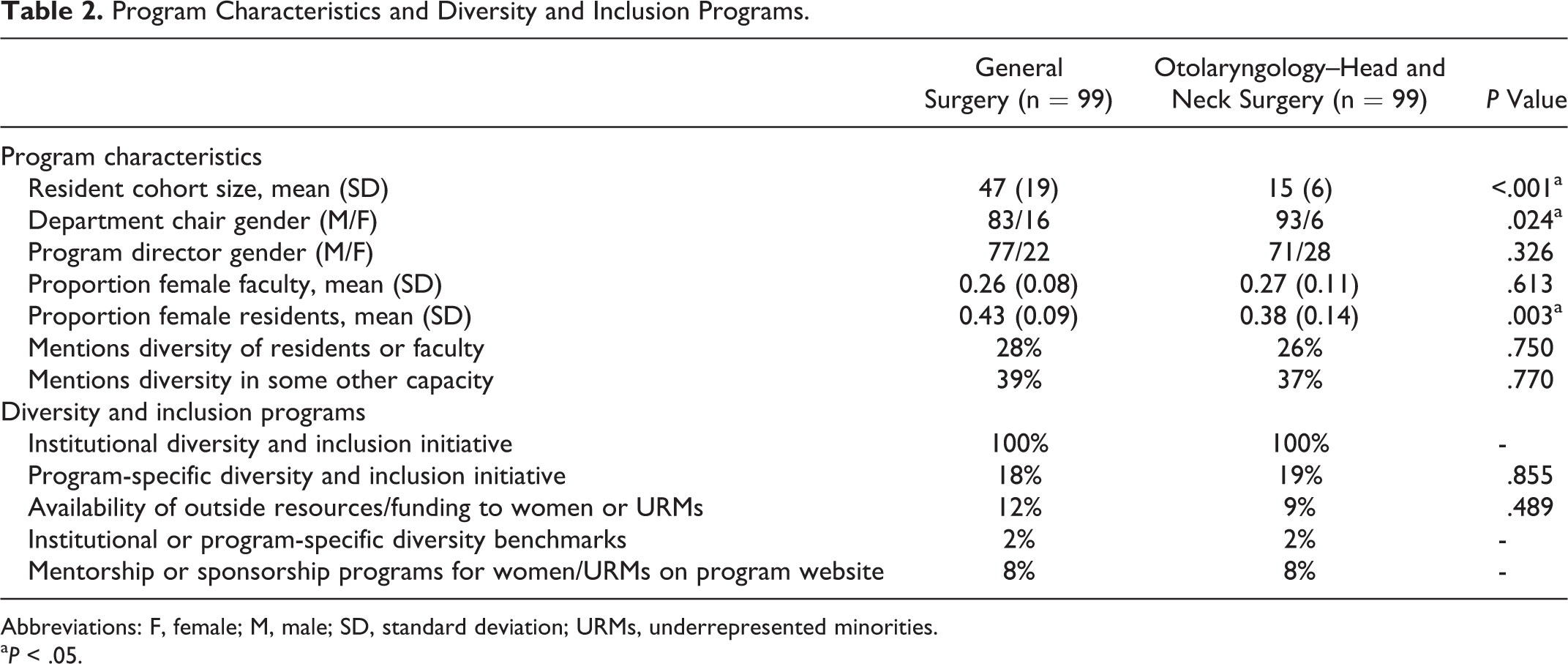
Abbreviations: F, female; M, male; SD, standard deviation; URMs, underrepresented minorities.
aP < .05.
Of the variables included in analyses, only the presence of D&I language on the program website and program-specific D&I initiatives were associated with a statistically significant increase in the proportion of female residents. The magnitude of effect of these variables on the proportion of female residents is described in Table 3.
Influence of Leadership and Initiatives on the Proportion of Female Residents.
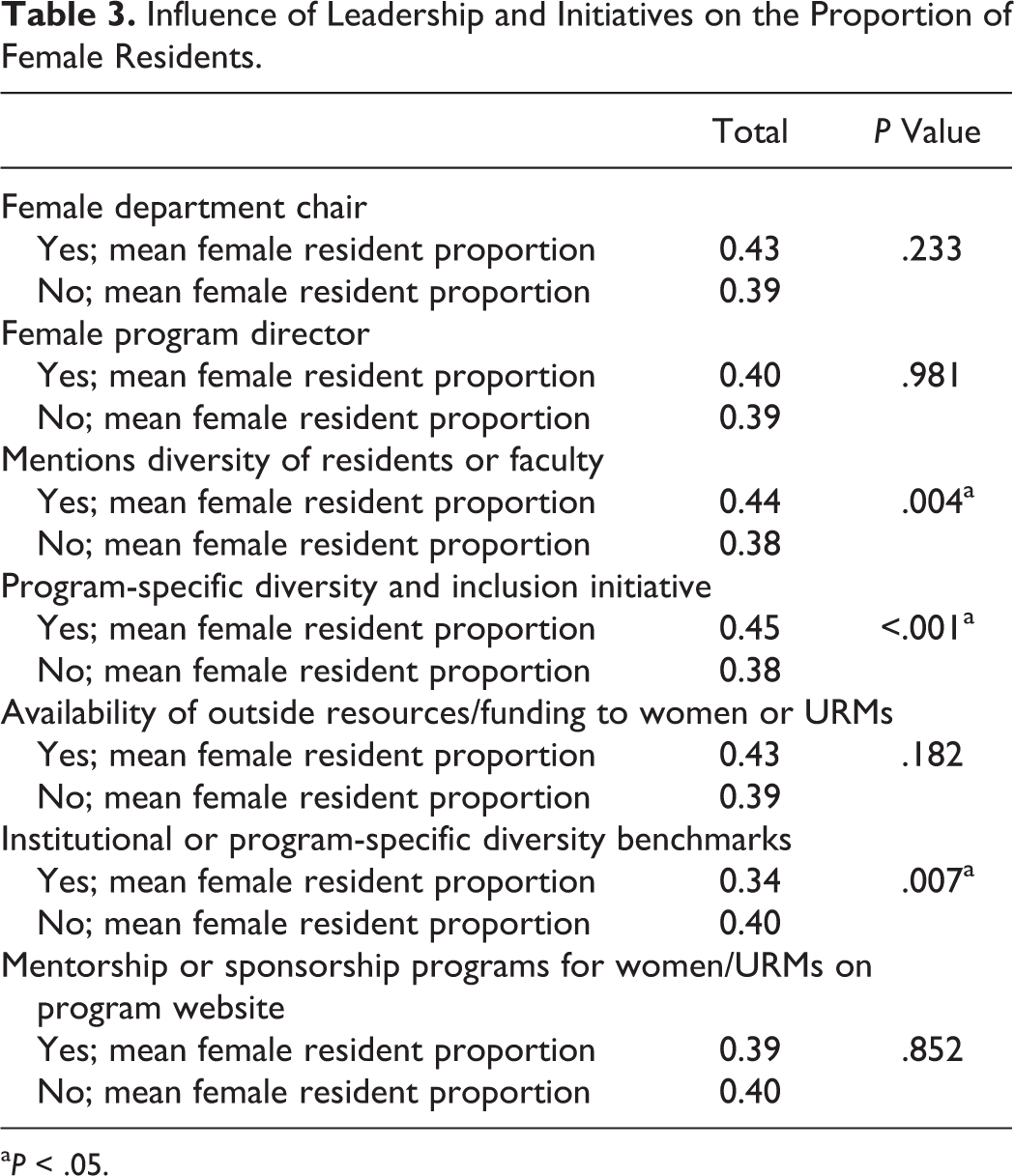
aP < .05.
Discussion
In response to the ACGME’s D&I mandate, our primary objective was to quantify and describe D&I initiatives present in OHNS and general surgery residency programs and their host institutions. To our knowledge, this has not been previously described. We found no statistically significant differences between D&I programming in otolaryngology residency programs when compared to general surgery programs. While all programs have institution-wide D&I initiatives, only 19 otolaryngology programs and 18 general surgery programs promoted initiatives of their own aimed at recruiting and retaining diverse faculty and residents. Our secondary objective was to characterize the relationship between the presence of these initiatives and program-specific gender diversity. We found, as seen in other studies,23-29 that women are underrepresented in both OHNS and general surgery residency programs and in leadership positions.
At baseline, otolaryngology and general surgery residency programs have similar proportions of female faculty and program directors. There was a significantly higher proportion of female residents at programs that talked about the importance of D&I or had D&I initiatives listed on their websites. There was also a significantly higher proportion of female faculty and residents in programs with specific and measurable diversity goals or benchmarks.
The case for diversity has been made emphatically in disciplines outside of medicine. The Harvard Business Review article, “Why Diverse Teams are Smarter,” highlights a 2015 report on 366 public companies. Those in the top quartile for ethnic and racial diversity in management positions were 35% more likely to report financial returns outperforming the industry mean; those in the top quartile for gender diversity were 15% more likely to outperform the industry mean. 32 Additionally, one group assessed the effect of pro-diversity policies on corporate innovation by studying the performance of over 3000 publicly traded companies. Companies fulfilling 9 positive diversity requirements were more productive and resilient in response to the 2008 financial crisis. 33 Simply put, striving for D&I is not only a good ethical objective, it is also a good business strategy. The literature on D&I initiatives in higher education demonstrates similarly positive outcomes (Figure 1).34,35
Benefits of diverse academic learning environments.
The case for a diverse health-care workforce typically highlights the potential for (1) advancing cultural competency in health-care delivery, (2) increasing access to high-quality health-care services, and (3) broadening the medical research agenda by including diverse talent. 36 Nonetheless, there is a lack of diversity in otolaryngology despite repeated calls for an increase in gender, racial, and ethnic diversity.11,16,21-23,36-41 In a 2013 study by Schwartz et al, the authors reported that annual growth rates among African American and Native American residents in OHNS were not statistically significant, hovering at ∼2%. 19 The growth rate for Hispanic Americans in OHNS was significant, but occurring at only half the growth rate of the Hispanic population in the United States. They did find a statistically significant increase of women in OHNS. Our data support this finding but also suggest women are still underrepresented in leadership positions.19,27-29
A Call to Action
Dr Joan Reede, a pediatrician and Harvard’s Dean for Diversity and Community Partnership, describes D&I as more akin to gene editing than cosmetic surgery: “You can make a pretty picture by adding different-colored faces, but the goal of improving representation has to be added to a school’s DNA—it has to be embedded in the organizational infrastructure. 42 Institutional change is possible, but not without courageous leadership and specific action. To affect change in residency training programs, we must set specific, actionable goals leading to diversity and inclusivity (Figures 2 and 3).
A multifaceted approach to increasing representation for women and underrepresented minorities.

Several specialty and program characteristics are important to women and URM students in their selection process, including pipeline programs, availability of mentorship by other women or URMs, presence of minority association groups and specialty-specific interest groups for women, years to complete training, and match rate.43-48 By these metrics, our data suggest otolaryngology is doing poorly as a field. Otolaryngology applicants are feeling decreasingly capable of measuring up to their understanding of an “ideal otolaryngology applicant” and increasingly like matching in otolaryngology is nearly impossible.49,50 Thus, we recommend OHNS programs invest in pipeline and mentorship programs and other D&I initiatives to make OHNS more attractive to women and URM applicants.
Newsome et al found in a survey of otolaryngology programs that most departments have one or zero URM faculty members. This translates to a limited number of URM mentors for medical students and residents. 51 While mentorship of women and URM medical students has been found to increase interest in OHNS residency training, 48 our study identified such opportunities in only 8 of 102 program websites surveyed. This may not be a perfect indicator of mentorship at these institutions, as organic mentorship develops over time and may occur out of the public eye. However, the dearth of publicly available information limits the ability of applicants to assess training programs for these resources. We recommend increasing the availability and active promotion of mentorship and sponsorship opportunities for women and URMs in OHNS.
Our study found women to comprise a minority of otolaryngology faculty (26%), and while they are proportionately represented among program directors, they are vastly underrepresented as department chairs. This reflects the “decanal divide” described by Schor wherein women are prevalent in leadership positions focusing on education, mentoring, and public image, while underrepresented in strategy, policy, and research. 52 This also reflects stereotype threat, where people feel at risk of conforming to negative stereotypes about their racial, ethnic, gender, or cultural group.53-55 A salient example of this is how Asian-American women perform better on math tests when reminded of their ethnic identity but worse when reminded of their gender identity. 56 Classically, women are seen as more nurturing, kind, sympathetic, and agreeable, while men are seen as more assertive, ambitious, competitive, and independent.57,58 This descriptive difference has prescriptive implications: the mental model of leadership remains predominately male, and men are assumed to be more competent than women with identical credentials,57,59,60 despite studies of leadership effectiveness showing women to be equally effective.61,62 To mitigate this, we must support women and URMs in leadership positions across OHNS.
Addressing disparities in representation demands action on behalf of leadership and institutions. Changing the culture of institutions demands authentic, bold, and courageous leadership that empowers others to speak up, creates a culture of inclusivity, and addresses obstacles and power structures that have historically systemically disenfranchised women, LGBTQ+ individuals, and people of color. Moreover, it requires our programs and institutions to meaningfully devote resources—both time and money—to increase D&I. Of 99 otolaryngology residency websites reviewed, only 9 indicated availability of funding for URM students wishing to spend a month training at their institution and 8 indicated mentorship opportunities specifically for women or URMs. While this perceived lack of resources may be a result of residency program websites being “inadequately comprehensive, 63 it highlights the importance of maintaining accurate, up-to-date information on websites as we seek to attract a diverse physician workforce. Change requires attention and commitment; thus, we recommend institutions demonstrate this by meaningfully devoting resources to fund sustainable D&I initiatives.
This study is not without limitations. We were only able to gather data on gender of faculty members and residents at general surgery and otolaryngology residency programs based on information available on institutional and program websites. Gender describes only one portion of identity diversity. We were unable to collect the race or ethnicity of the individuals included in this study. Similarly, faculty and resident profiles provide insufficient detail to allow capture of data that may contribute to cognitive diversity (eg, multicultural background, first generation physician, rural vs urban upbringing). As such, gender serves as a proxy for our understanding of overall diversity. Additionally, our cross-sectional sample does not control for fluctuations in the relative proportion of female faculty members or residents over time. Despite this limitation, these data serve as an important baseline for understanding the prevalence of D&I initiatives within otolaryngology. Because the number of programs with specific diversity benchmarks were so few (n = 4), the significance of the relationship between these benchmarks and increased diversity should be interpreted cautiously. Finally, the data in this study were captured from the websites of programs. These websites may not accurately represent the current members of the department or the programs aiming to increase D&I. Importantly, if departments are aiming to recruit a more diverse workforce, these efforts should be reflected in their Internet image. Future studies may look to compare diversity metrics within otolaryngology to those in nonsurgical subspecialties within academic medicine such as internal medicine, as these fields have traditionally been thought of as perpetuating less gender bias.
Conclusions
Diversity in medicine positively impacts patients and health-care teams. Otolaryngology suffers from significant underrepresentation of minorities and women. Despite the ACGME’s recent emphasis on recruiting and retaining a diverse physician workforce, few otolaryngology residency programs advertise concerted, funded efforts toward increasing D&I in their residency programs. While women may be experiencing representative growth in otolaryngology and general surgery, they still lag in representation in leadership positions, especially at the departmental chair level. Programs that have D&I initiatives have a higher proportion of female residents. To increase representation of women and URMs in OHNS, systemic change is required, including but not limited to increased support for women and URMs in leadership positions, further development of pipeline and mentorship programs, and meaningful devotion of resources to D&I.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.