
Abstract
Background and Objectives:
Bell’s palsy (BP) is the most frequent cause of unilateral facial paralysis, and inflammation is believed to play an important role in pathogenesis. Due to its rarity, however, no consensus has been reached regarding optimum treatment or factors affecting prognosis. In the present study, treatment outcomes and prognostic factors of BP were investigated in pediatric patients who underwent steroid therapy. The goal was to investigate the relationship between BP and inflammation using multiple inflammatory markers, including neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), mean platelet volume (MPV), and red cell distribution width (RDW).
Materials and Methods:
In all, 54 patients diagnosed with BP and 39 healthy randomly selected controls were enrolled in this retrospective study. Demographic characteristics and complete blood cell count test results were compared. In addition, prognostic factors were sought by dividing the 54 patients with BP into 2 groups according to the House-Brackmann grading system: low grade BP (grades II and III) and high grade BP (grades IV and V). Serum samples were analyzed retrospectively on initial presentation and 6 months after the symptom begins. Meaningful hematological parameters include NLR, PLR, MPV, and RDW.
Results:
The NLR values in the BP group were significantly higher than in the control group. The NLR value in the 2 groups of patients with BP differed significantly. The mean PLR value in the BP group was higher than in the control group; however, there were no significant differences between the low-grade and high-grade BP groups nor were there any statically significant differences in the other characteristics.
Conclusion:
The NLR and PLR values are readily accessible parameters that may be useful prognostic markers in pediatric patients with BP. Further studies are required to confirm these results and their utility in predicting prognosis and treating pediatric patients with BP.
Keywords
Introduction
Bell’s palsy (BP) is the most common cause of facial palsy and is characterized by acute and peripheral facial weakness; however, its pathogenesis remains unclear. 1 Numerous studies investigating the cause of BP have suggested viral infection, inflammation, and microvascular failure. 2 Nevertheless, the pathophysiology of BP appears to be no different between adults and children. 3
Recent studies investigating the neutrophil-to-lymphocyte ratio (NLR) have been conducted in relation to the diagnosis and prognosis of BP.4,5 The NLR is a simple, inexpensive, and useful marker to measure the severity of systemic inflammation. 6
The platelet-to-lymphocyte ratio (PLR) is associated with poor prognosis in patients with peripheral vascular conditions such as coronary arterial occlusive diseases. 7 Although previous studies have reported hemodynamic data from adult populations with BP, there is no clear understanding of hematological-based evaluation in pediatric BP due to its low incidence and difficulty of detection. The aim of this study, therefore, was to investigate the correlation between disease severity and hemodynamic parameters (ie, NLR and PLR) in pediatric patients with BP and to evaluate the prognostic utility of these parameters.
Materials and Methods
Patient Selection
This was a retrospective study based on a review of medical records of patients with BP between 7 years and 18 years of age diagnosed between January 2010 and December 2018 in the otolaryngology department of a tertiary hospital. Participants included 54 patients with BP and 39 randomly selected healthy individuals who visited for routine checkup. The study was approved by the institutional review board at the authors’ hospital. Patients with acute or chronic otitis media, trauma, tumor, Ramsay-Hunt syndrome, congenital facial palsy, diabetes, or other associated systemic inflammatory diseases, age older than 18 years, were excluded from analysis.
Hematological Testing
All patients underwent blood collection at admission and 6 months after the symptom begins. A complete blood count (CBC) investigation was performed to assess the number of white blood cells (WBC [lymphocytes and neutrophils]) and platelets. The authors simply calculated the PLR and NLR, mean platelet volume (MPV), and red cell distribution width (RDW) using CBC data.
Treatment and Evaluation
All patients were treated with oral systemic corticosteroid therapy. The initial dose of prednisolone was 1 mg/kg/d and was gradually tapered for at least 10 days. The severity of BP was classified according to the House-Brackmann (HB) grading system. According to the HB facial nerve grading system, 6 months after start of treatment, grades I and II were defined as satisfactory recovery, grade III and IV were defined as unsatisfactory recovery, and grades V and VI reflected no recovery.
Age, sex, treatment results, and hematological test (WBC, neutrophils, lymphocytes, monocytes, PLR, NLR, MPV, and RDW) results were analyzed and compared between the BP and control groups.
Statistical Analysis
Descriptive statistics are reported as proportions or means with standard deviations. Intergroup differences were analyzed using the Mann-Whitney U test and Kruskal-Wallis test. Categorical data were analyzed using the Fisher exact test or Pearson chi-square test. Statistical analysis was performed using SPSS version 20 (IBM Corporation, Armonk, New York); P < .05 was considered to be statistically significant.
Results
In all, 54 patients (30 [56%] male, 24 [44%] female; mean ± standard deviation [SD] age, 11.9 ± 5.2 years [range, 2-18 years]) with BP were included in the study (Table 1).
The Characteristics of the Groups.
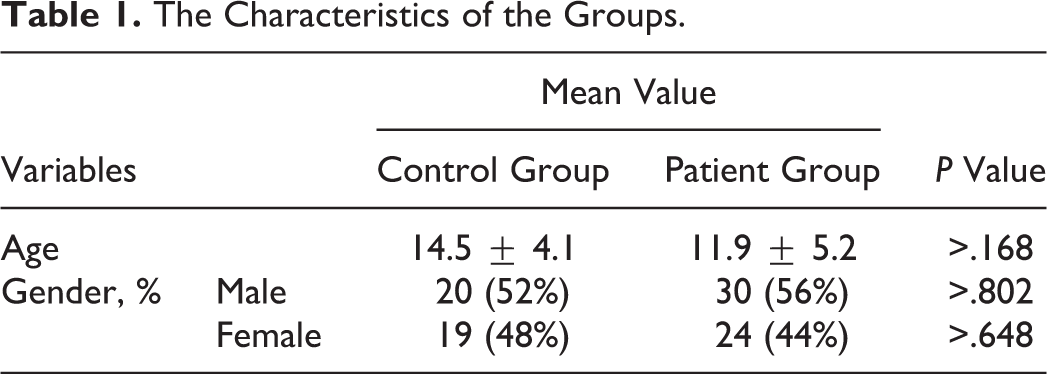
Patients diagnosed with BP were divided into groups based on the severity of their facial paralysis according to the HB grading system. Four (7.4%) patients were diagnosed with grade II, 21 (38.9%) with grade III, 25 (46.3%) with grade IV, and 4 (7.4%) with grade V palsy. Most patients were treated within 1 week of facial palsy onset.
The total WBC count was significantly higher in the BP group (9.16 ± 3.12 × 103/mm3 vs 7.06 ± 1.41 × 103/mm3, P = .020). In addition, neutrophil and lymphocyte counts were higher in the BP group (both P < .001). The mean NLR was 2.19 ± 0.90 in the BP group and 1.63 ± 0.73 in the control group (P < .001), and the mean PLR was 168.6 ± 4.10 in the BP group and 113.26 ± 33.11 in the control group (P > .010). The mean absolute neutrophil count in the BP group was 5300 ± 1900/mm3, and the mean absolute lymphocyte count was 3500 ± 1300/mm3. Mean platelet volume was 9.0 ± 0.4 fL and RDW was 12.1% ± 4.0% on admission. The mean NLR values in patients with BP were significantly higher than in the high HB group (P < .007; Table 2).
The Hemodynamic Data of the Groups.
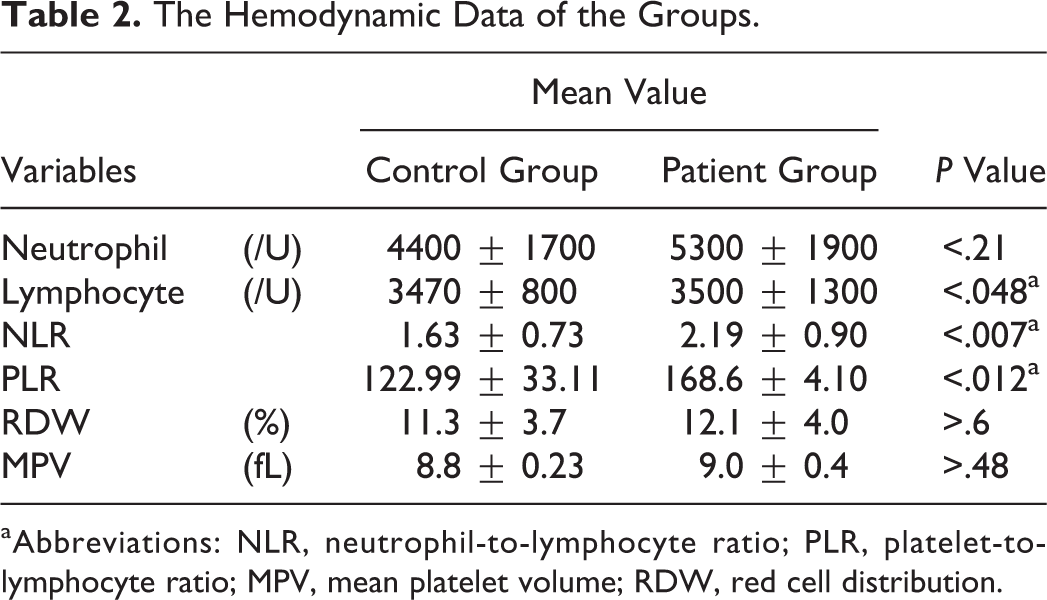
aAbbreviations: NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; MPV, mean platelet volume; RDW, red cell distribution.
There was a positive correlation between NLR and HB grade of facial paralysis (r = 0.661, P < .0001). The mean ± SD NLR values in the grades II, III, IV, and V BP subgroups were 1.91 ± 1.17, 1.87 ± 1.15, 1.89 ± 0.89, and 1.60 ± 1.28, respectively. The mean NLR values in the grade IV BP group were significantly higher than in the other groups (P < .022; Figure 1).
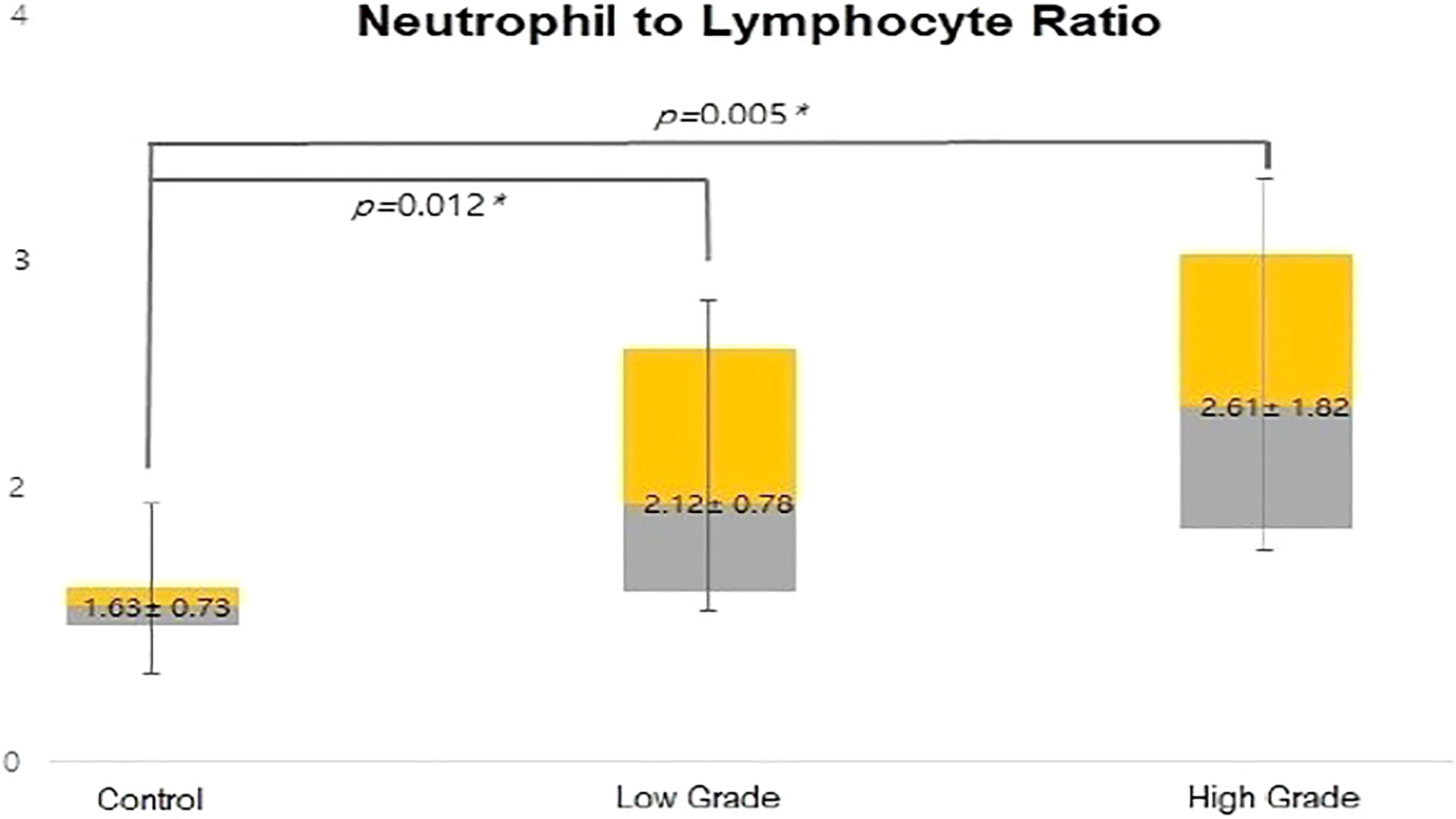
The mean neutrophil-to-lymphocyte ratio of patients with Bell’s palsy and the control group.
In addition, there was also a statistical correlation between PLR levels and the prognosis of facial palsy, which was confirmed by the percentage of patients with high PLR levels recovering below HBII after 6 months of steroid treatment (P < .012; Table 3).
The Hemodynamic Data of the Groups After Treatment.
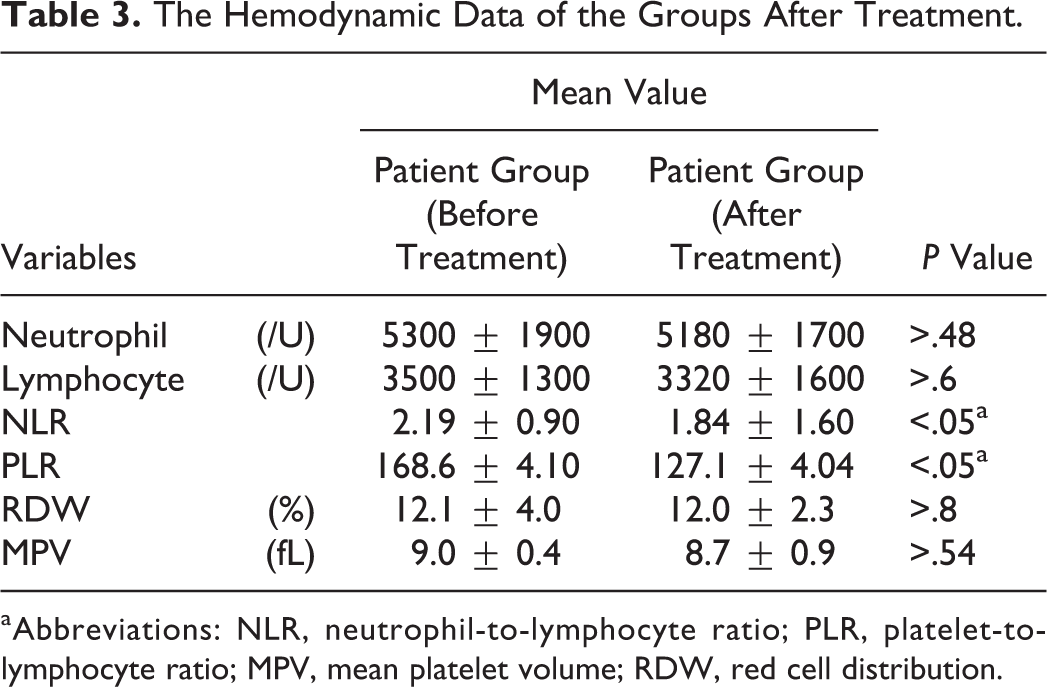
aAbbreviations: NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; MPV, mean platelet volume; RDW, red cell distribution.
Higher levels of NLR was exhibited in patients with high-grade patients with BP (HB grade IV and V) than patients with lower grade of BP (HB grade II and III; 2.41 ± 1.24 vs 1.93 ± 0.95; Figure 1).
On the other hand, PLR values were also found to have positive correlations with HB grade, patients who revealed higher level of PLR shows no good effect on treatment and the degree of improvement in facial palsy was low, although the correlations were lower compared with NLR (104.2 ± 4.19 vs 128.3 ± 4.99; Figure 2). The MPV values were measured to be low in relation to the HB grade as measured previously (9.1 ± 4.5 fL vs 9.1 ± 11.6 fL; P > 0.6; Figure 3). The RDW values demonstrated no positive correlation between the control group and patients with BP (12.7% ± 2.29% vs 11.6% ± 25.80%; P > .48; Figure 4).
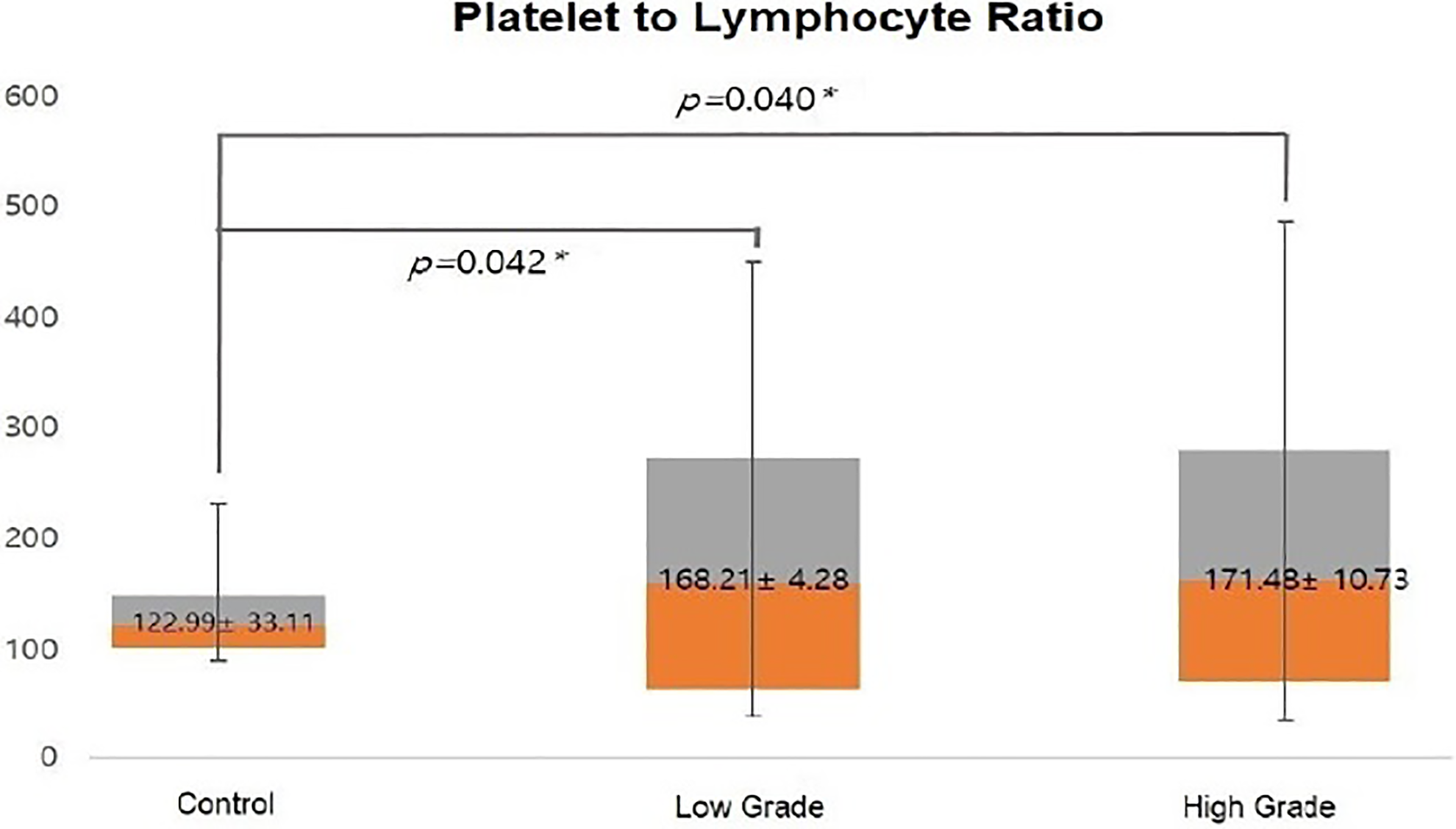
The mean platelet-to-lymphocyte ratio of the patients with Bell’s palsy and the control group.
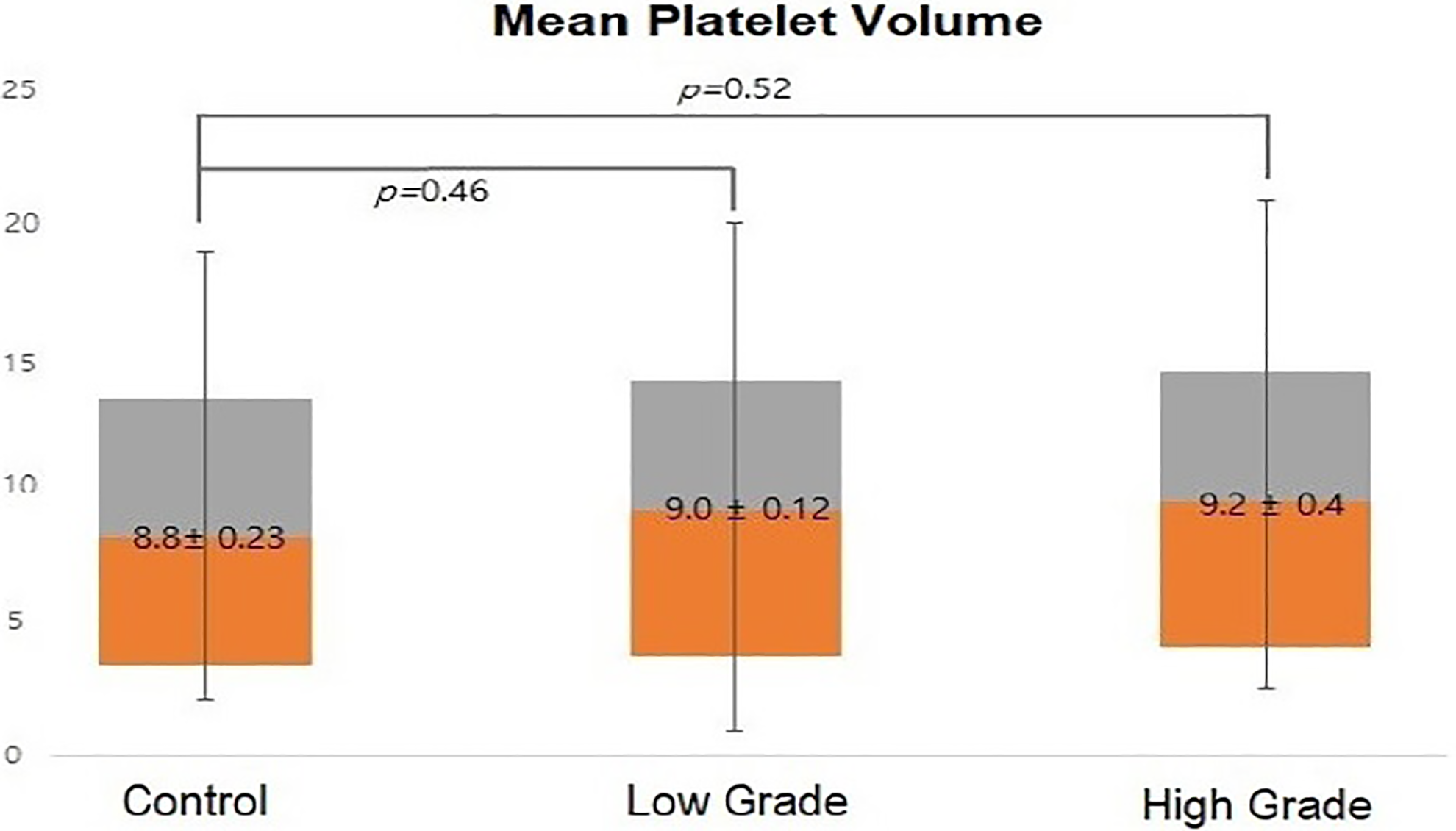
The mean platelet volume of patients with Bell’s palsy and the control group.
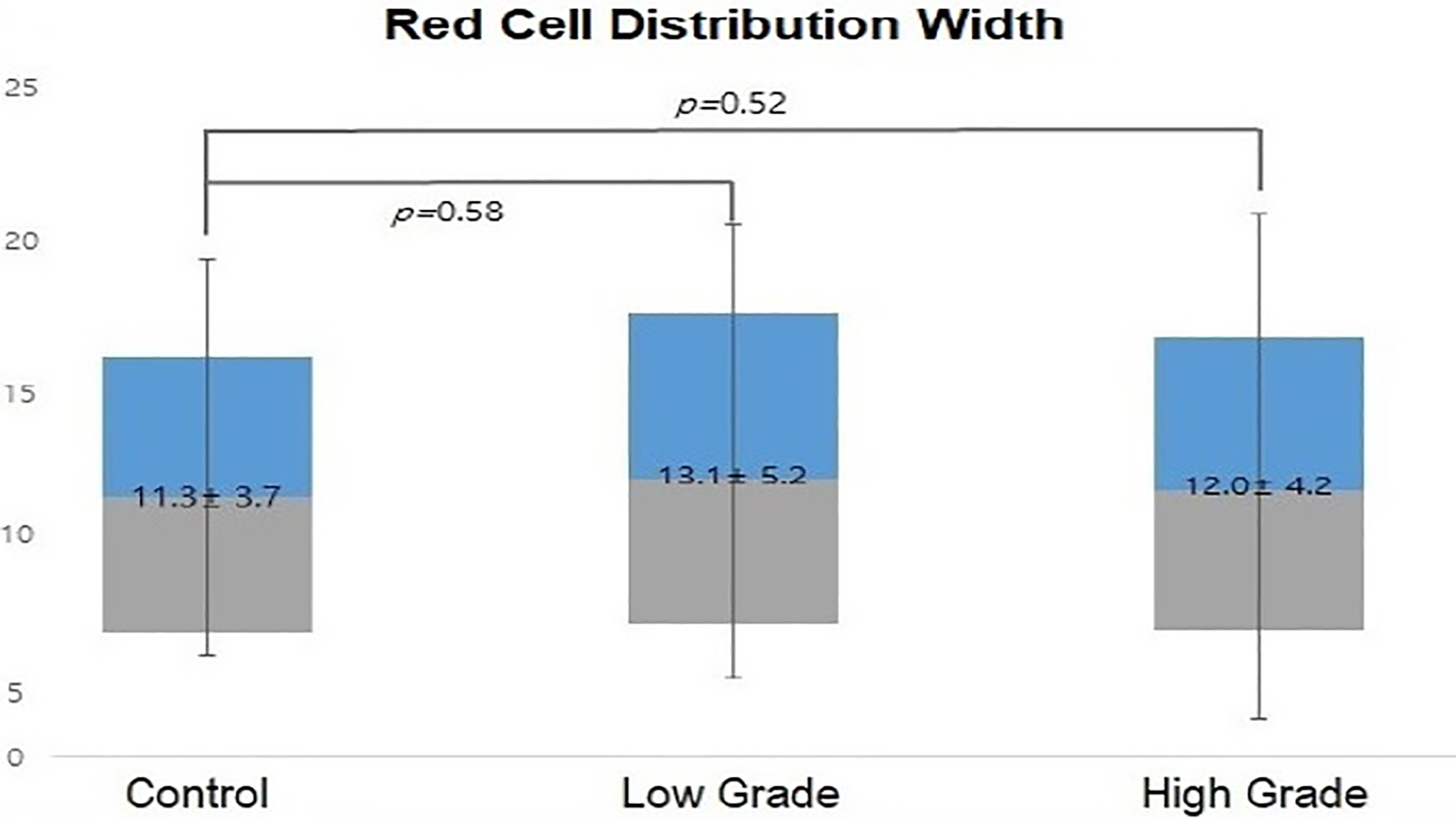
The mean red cell distribution width of patients with Bell’s palsy and the control group.
Discussion
The incidence of BP is approximately 20 to 30 per 100 000 adults 8 ; the incidence of BP in children, however, is lower, approximately 2.7 to 10.1 per 100 000. 9
The first treatment option for pediatric BP is administration of corticosteroid, which plays an important role in preventing further neural damage. Researchers have achieved favorable results in almost all patients with HB grade II BP. 10 For good recovery of facial function, investigators have recommended that physicians initiate steroid therapy within 3 days of symptom onset. 11
In a study investigating initial steroid dose, it was reported that the effect of low-dose oral prednisolone (1 mg/kg/d) was similar to high-dose therapy (2 mg/kg/d). Therefore, the authors recommended that oral prednisolone (1 mg/kg/d) was highly effective in the treatment of BP in children. 12 Accordingly, we used a low dose of oral prednisolone (1 mg/kg/d) in our study.
In a study examining the effect of oral steroids in 109 patients with BP, all children experienced full recovery with oral steroid therapy within 2 months of treatment. 13 In another study, the proportion of idiopathic facial palsy in children was 77.8%, and the recovery rate at 2 months within HB grade II was 89.4%. 14
The prognosis of facial nerve palsy in children appears to be more favorable than in adults. In a study using electrophysiological testing comparing adults and children, the authors reported a more favorable prognosis for facial nerve palsy in children, which was explained by the shorter length of the facial nerve, and faster and better regenerative capacity of damaged axons at younger ages. 15
Some reports have described the effect of combined corticosteroid and antiviral agent therapy in patients with BP. There were no additional benefits of antiviral agents compared with treatment using corticosteroid alone in BP.16,17 Consequently, the effect of antiviral agents has not yet been verified. 16
The causes of BP remain unclear, although viral infection, microvascular circulatory impairment, and genetic and immunological diseases have been proposed as possible factors. 17 A magnetic resonance imaging study using gadolinium revealed marked facial nerve enhancement in the distal intrameatal portion, geniculate ganglion, and proximal labyrinthine segment in patients with BP, which may support a hypothesis involving nerve inflammation. 18
A CBC provides useful information for evaluating a patient’s general state and inflammation status. The NLR and PLR can be easily calculated from CBC data. The NLR is regarded as a marker of systemic inflammation. It reflects inflammatory status and also provides important information about prognosis. 19 The PLR has been used to gauge the risk for microcirculatory thromboembolism. In BP, one group of investigators reported a correlation between high PLR and BP in adult patients.20,21
Eryilmaz et al 4 reported that NLR values were higher in pediatric patients with BP than in the control group and, thus, suggested that NLR is a supportive parameter in the diagnosis of pediatric BP. 4 Our study yielded results consistent with those reported by Eryilmaz et al.
According to a study that used hematological findings from patients with BP, WBC count was the same in the recovery group and nonrecovery group. However, the neutrophil ratio was higher and lymphocyte ratio was lower in the nonrecovery group compared with the recovery group. The NLR was significantly increased in the nonrecovery group. The authors proposed that pretreatment hematological laboratory results reflect the severity of inflammation and bone marrow dysfunction caused by viral infections. 22
In 2017, Sahin and Varım 23 reported that NLR and neutrophil count were significantly higher in patients with BP than in the control group. On the other hand, there was no significant change in PLR, MPV, or RDW. Accordingly, the authors concluded that BP may more likely be an inflammatory than ischemic disease. 23
In cases of BP in adults, the mean NLR values of patients with BP were significantly higher than in the control group, and there was a significant correlation between initial facial palsy grade based on the HB grading system and NLR values. 24 Based on this point, the authors proposed that NLR is a new predictive and prognostic factor in BP. 24 Bucak et al found a correlation between higher NLR values and unsatisfactory recovery after steroid treatment. The authors commented that there could be a more intense inflammatory process in patients with high NLR values. 5 In contrast, other investigators have reported no correlation.4,21 Additionally, NLR was considered to be a reliable marker for predicting diagnosis and prognosis of patients with other otological diseases such as sudden sensorineural hearing loss. 25
Both MPV and RDW can be easily ascertained in a routine CBC study and indicate inflammatory and thrombotic status. High MPV value has been proposed to be a marker for platelet size and high platelet activity but not their actual number. 26 The authors commented that MPV was increased in thrombotic events including stroke or obstructive coronary artery disease. However, MPV values have wide variability according to sex, age, and ethnicity; therefore, MPV values are not useful for the diagnosis of disease and prediction of prognosis. 26 There was no difference in MPV values between control and patients with BP in research investigating MPV values in adult patients with BP.19,23
The present study was the advanced study to investigate pediatric BP, and our results may inform the development of future guidelines for prognosis of children with the disease. Furthermore, it suggests directions for further study of BP in childhood.
Red cell distribution width is a parameter indicating the diameter and variation of erythrocyte volume. Red cell distribution width can increase in anemia, and in hemolytic, microvascular thrombotic, 27 and inflammatory 28 diseases. In recent research, RDW was significantly higher in nonrecovered patients with BP than in those who recovered. The authors proposed the RDW could be a useful prognostic factor in patients with BP. 29 In contrast, RDW values were no significantly higher in patients with BP in another report. 23 Our results also demonstrated that there were no significant differences in MPV or RDW, which suggests that MPV and RDW are not meaningful parameters in children with BP.
We calculate the effect size between the mean value of NLR, PLR, MPV, and RDW of our study. Therefore, effect size of variables, such as NLR and PLR, shows medium and large effect, relatively (0.435, 5.231) but MDV and PDW has small effect (less than 0.001 and 0.060, relatively).
Limitations of this study include its retrospective design and small number of pediatric patients with BP. Thus, further, multicenter, prospective studies are warranted.
In conclusion, pretreatment hematological findings in pediatric patients with BP provide useful information. The NLR and PLR values were increased in pediatric patients with BP. As a result, we suggest that the cause of pediatric BP may be a combination of inflammatory response and microcirculatory problems.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.