
Abstract
Spontaneous cerebrospinal fluid otorrhea is very rare. Because of nonspecific symptoms, it is usually diagnosed when complications such as meningitis occur. Cerebrospinal fluid leak may be caused by cochlea malformation, which permits nonphysiological communication between subarachnoid space and tympanomastoid cavity. Nearly 20% of congenital sensorineural hearing loss is connected with inner ear bone malformation. We present a case of 40-year-old man suffering since early childhood from recurrent meningitis and right ear deafness, caused by congenital internal ear malformation. For many years, patient with sensorineural hearing loss had not undergone diagnostic radiology; computed tomography scans of the temporal bone had not been performed. Developing meningitis in early childhood was regarded as the reason for deafness.
Keywords
Introduction
A cerebrospinal fluid (CSF) leak can be potentially life-threatening. It can be posttraumatic—as presented in 21% of patients with a temporal bone fracture, iatrogenic—in 6% to 15% of patients after a skull base surgery, or rarely, spontaneous. Until now, spontaneous CSF has been reported in less than 500 cases in the literature. 1 Thus far, there have been 20 cases of chronic otitis media with CSF leak described in the literature. 2 It is usually presented with nonspecific symptoms such as ear fullness, tinnitus, headache, and vertigo. In some cases, rhinorrhea, otorrhea, or a middle ear effusion can mask a CSF leak for a long time. Spontaneous CSF otorrhea is caused by an abnormal communication of the sterile subarachnoid space with the tympanomastoid cavity. This condition predisposes to various viral or bacterial infections and can increase the risk of developing meningitis in 93% of children and 38% of adults. 1,3
Fistulas extending from the subarachnoid space to the middle ear cavity can be classified as perilabyrinthine or translabyrinthine. The translabyrinthine type is associated with a developmental anomaly of the cochlea. 4,5 Cochlear malformations in the translabyrinthine type cause a lack of well-developed modiolus, permit communication between the CSF and the perilymphatic spaces, and make the leakage through the oval window or a hole in the stapes footplate. 4 -6
Approximately 20% of cases of congenital sensorineural hearing loss are connected with inner ear bone malformations. They are easy to detect with a radiological investigation such as computed tomography (CT) or magnetic resonance imaging (MRI) scans of the ear. 7 Jackler’s classification, which is based on 98 malformed ears, is the most widely accepted. In 1987, his classification distinguished deformities such as complete labyrinthine aplasia (Michel deformity), cochlear aplasia, cochlear hypoplasia, incomplete partition (Mondini deformity), and common cavity. 8 Nowadays, thanks to more frequent CT scans of the ear, which are performed prior to cochlear implantations, Sennaroglu and Saatci have made some modifications in the classification and have added the terms for 2 different incomplete partition deformities: IP-1 (cystic cochleovestibular malformity) and IP-2 (the classic Mondini deformity). It was created in order to describe these groups of malformations more precisely. 7 For many years, patients with sensorineural hearing loss had not undergone diagnostic radiology; CT scans of the temporal bone had not been performed. This precluded identification of the inner ear deformity and caused suspicion of fistulas. Developing meningitis in early childhood was regarded as the reason for deafness. One of such cases is described below.
Case Study
We present a case of a 40-year-old man suffering from recurrent meningitis. He has been deaf in his right ear since early childhood, presumably due to the first episode of meningitis. The episode of rhinorrhea occurred after vacuuming, during which his head was in an extended inclined position. The patient had not had a CT scan of the temporal bone for years, and the radiologist who performed a CT scan of the head noticed no malformation. Many years later, after having the sixth episode of meningitis, during another ENT consultation, a lateral semicircular canal deformation was noted in a CT scan of the head. A CT scan of the temporal bone was advised. Upon performing the advised CT scan, which showed the right internal ear malformation, IP-1 and fluid in the middle ear were stated (Figures 1 –3). The CSF was confirmed by β-tracepepide analysis. Transcanal microscopic operation was performed. Dehiscence of oval windows was identified, and CSF leak was noted. The stapes were removed, and the obliteration of a vestibule with the use of the crushed temporalis muscle was performed. The perichondrium was put on the oval window and then covered with TachoSil. During the operation, after the stapes had been removed, an intensive outflow of CSF was observed. Packing the vestibule with a muscle stopped a CSF gush. Four-day-long bed rest was recommended, and the head of his bed was elevated. We did not apply a lumbar drain. After the operation, the patient did not suffer from vertigo, and CSF leak was not observed. There was no episode of meningitis during the 12-month period following the operation. Periodic MRI scans show a complete opacification of the whole vestibule with a muscle and no fluid in the middle ear cavity (Figure 4). Otoscopy view doesn’t show CSF fluid in the middle ear (Figure 5).
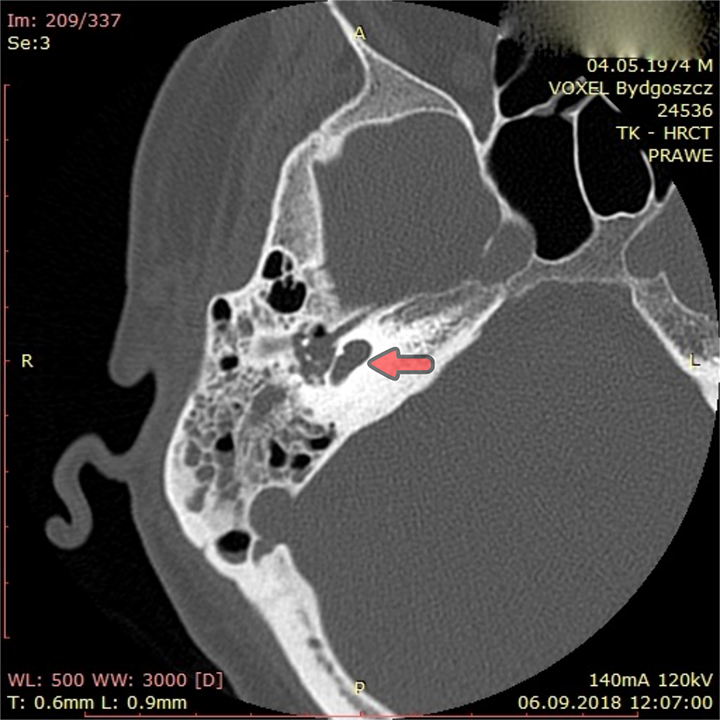
High-resolution computed tomography scan of the ear. Incomplete partition 1. Red arrow: cochlear.
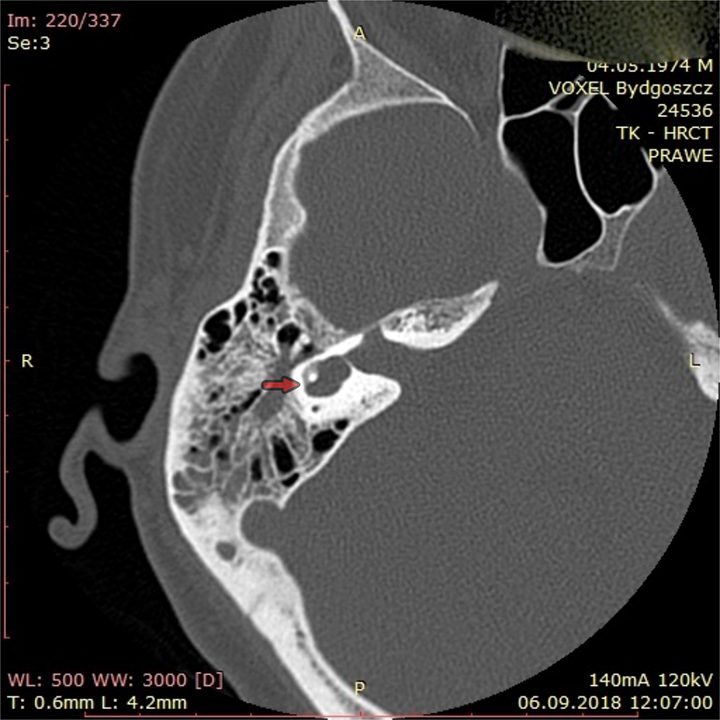
High-resolution computed tomography scan of the ear. Incomplete partition 1 (IP-1), fluid in the middle ear. Red arrow: labyrinth malformation with a small bony island and dysmorphic small lateral semicircular canal (it may exist in IP-1).
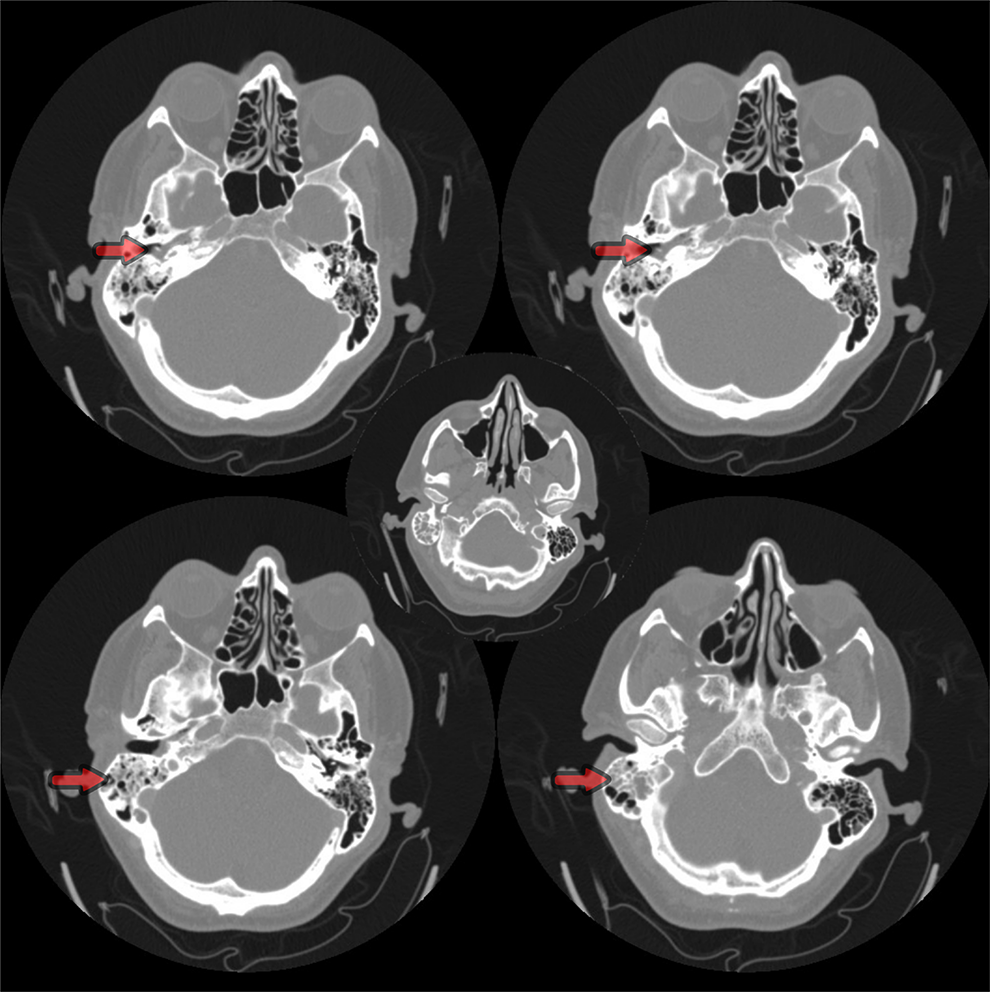
High-resolution computed tomography scans of the ear before surgery. Red arrow: cerebrospinal fluid leakage in the middle ear.
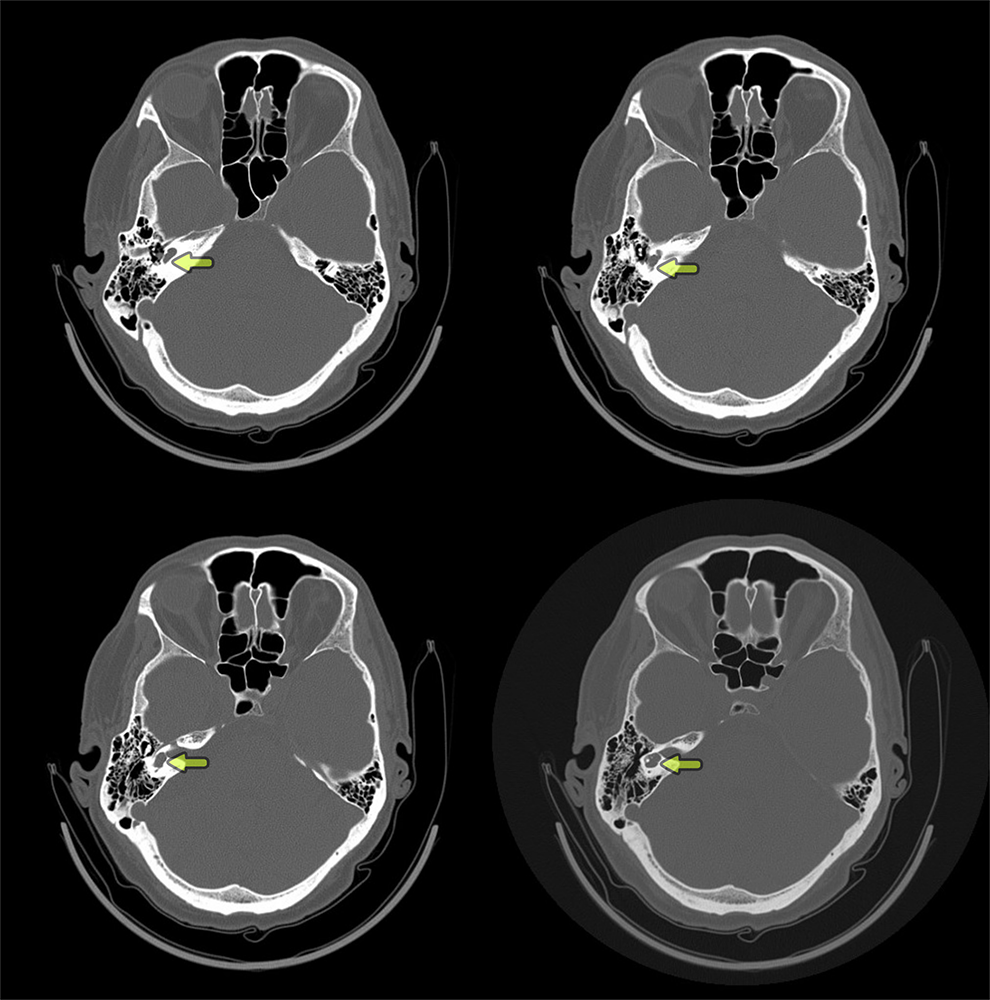
Control high-resolution computed tomography scans of the ear 12 months after surgery. Volt arrow: cochlear obliterated with muscle.
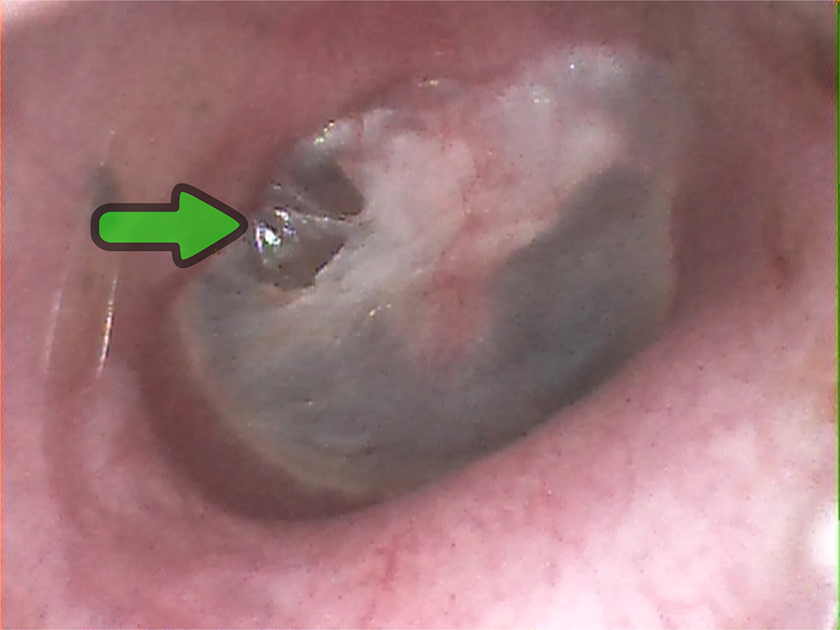
Control otoscopy 12 months after surgery. Green arrow: small retraction of tympanic membrane. No fluid in the middle ear.
Discussion
Congenital internal ear malformations with fistula and meningitis occur twice more often on the right side than on the left side. Till now, there have been 39 fistulas on the right side, 20 on the left side, and 16 bilaterally described. 9 There have only been 11 reports concerning children with IP-1 and meningitis. It seems to be essential to describe a new case and analyze diagnosis and treatment methods. Our patient had right-sided internal ear malformation type IP-1. The average period of meningitis recurrences is 3.27 years, and in our case, it was 6 years. 8
Performing a CT scan of the temporal bone in young patients with sensorineural hearing loss is controversial because of the costs, the risk of anesthesia, and the exposition to radiation. On the other hand, the treatment of complications from unrecognized illness pathology is expensive as well. Internal ear malformations should be discovered during the evaluations of hearing loss. Patients with inner ear malformations are at increased risk of bacterial meningitis. 10 Studies performed by Park et al 11 show that the average age for the recognition of inner ear malformations is 25.7 months. Stein et al 12 show the same result. Our patient seems to be holding a record of the longest time a human has had an unrecognized congenital ear malformation with CSF otorrhea and recurrent meningitis. Review form the last 20 years (1995-2015) performed by Muzzi et al describes 67 cases, and the oldest patient was 15 years old. 9 Thanks to the National Hearing Screening Program, which has been operating in Poland since 2002 until the present day, almost 5.8 million newborn children have been evaluated, which is nearly 100% of all children born at that time. These children could be diagnosed faster, but unfortunately for our patient, he was born before the program had been introduced. It was assumed that his deafness was caused by meningitis in childhood. No other diagnoses were performed, and the next 5 recurrences of meningitis were treated with antibiotics in an isolation hospital. Kuczkowski et al described 3 other cases of recurrent meningitis with internal ear malformations in Poland. 13 The children were 4, 5, and 15 years old. The 2 youngest children were born in the era of the National Hearing Screening Program, while the oldest one was born before it. It seems that the program results in a decrease of age at which the malformation is recognized. Still, there is a need for performing CT scans of the temporal bone in adults with sensorineural hearing loss and the episode of meningitis. Other authors see the necessity of performing CT scans as well. To decrease the cost and time of the exposition, Harcourt et al 14 described the protocol for performing a CT scan to evaluate idiopathic bilateral sensorineural hearing loss in older patients. Contiguous axial 1.2 mm sections were obtained from the superior semicircular canal to the inferior aspect of the cochlea. Cuts in both the axial and coronal planes were taken.
There have been a number of approaches for the closure of the fistula described, such as microscopic stapedectomy, 15 transcanal endoscopic ear surgery with oval windows closure, 16 blind sac closure of the ear canal, which is performed concurrently with a subtotal petrosectomy, 13 and the transmastoid lateral semicircular canal approach. 16,17
We performed a microscopic stapedectomy with removal of the posterior wall margin to identify processus cochleariformis, eminentia pyramidalis, facial nerve doorstep, and oval window. Then fistula on the oval window was identified, stapes was removed. We observed gusher, so obliteration of vestibule with the huge crushed temporalis muscle was done. After performing obliteration, we didn’t observer the leakage of perilymph. Tympanic membrane was supported by perichondrium taken from the tragus and ear was closed.
Before the surgery, patient was informed that an open approach (subtotal petrosectomy with the obliteration of the mastoid, middle ear, and the Eustachian tube with a muscle, along with the closure of the ear canal) might be necessary, depending on the intraoperative findings. In this case, after the vestibular obliterations, we put the perichondrium over the oval window and then TachoSil. We haven’t observed a direct leakage of CSF neither after the closure of the fistula nor during a 12-month period of the medical checkups. This procedure seems to be sufficient in this case, although we observed a severe CSF gushing after the stapes had been removed. In literature, this traditional method of repair has a failure rate of 30% to 60%. 15 Till now, packing the fistula both endoscopic and microscopic has been performed twice more often than subtotal petrosectomy: 17 cases and 8 cases, respectively. 9 For this reason, we should wonder whether the subtotal petrosectomy in these cases should be the first treatment of choice, due to its much more aggressive surgery.
Conclusions
Patients with inner ear malformations are at increased risk of bacterial meningitis. We recommend a CT scan of the temporal bone in children with progressive hearing loss or with a history of recurrent meningitis. The protocol proposed by Harcourt should be applied to reduce scan time and radiation dose. Deaf adults with recurrent meningitis should undergo radiological examination, which can identify the possible presence of internal ear malformations and fistulas. These patients are advised to avoid contact sports, scuba diving, or any other activities, which may result in the change of the pressure in the middle or inner ear. Thanks to the development of the hearing screening programs, the age at which malformations are recognized and, most probably, the mortality rate for recurrent meningitis have decreased. The transcanal microscopic approach has allowed a good view and the possibility of performing the operation with 2 hands. Packing the vestibule with the crushed temporalis muscle is sufficient.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.