
Abstract
Importance:
This is the first randomized study to compare the quality of life of patients undergoing endoscopic septoplasty compared to traditional trans-nasal trans-speculum (TNTS) septoplasty.
Objective:
To assess the clinical outcomes and quality of life results of endoscopic versus TNTS septoplasty in patients with septal deviation and nasal obstruction.
Design:
A prospective, randomized controlled trial comparing 2 approaches of septoplasty: endoscopic and TNTS septoplasty performed in a single institution during the years 2016 to2017. The follow-up time was 3 months.
Setting:
A single institution study in a tertiary health-care referral center.
Participants:
Patients who underwent primary surgery for repairing deviated nasal septum due to nasal obstruction, were older than 18 years old, and were eligible for study inclusion. Sixty-five patients were enrolled in this study, 34 in the endoscopic arm and 31 in the TNTS septoplasty arm. The overall follow-up rate was 94% at the first visit (2 weeks) and 92% at the last visit (12 weeks). Thus, the final cohort consisted of 60 patients, 30 in each study arm. The patients ranged in age from 18 to 71 years (mean 27 years) old.
Main Outcomes and Measures:
The primary outcome was the Sino-Nasal Outcome Test-22 (SNOT-22) score. Secondary outcomes were the Short Form 36 (SF36) QOL score and complication rates. Both questionnaires were administered at 2 weeks and 3 months following surgery.
Results:
Sixty patients completed this study, 30 in each study arm. Sino-Nasal Outcome Test-22 scores were improved after 3 months, with no difference between the study arms. There were no cases of septal perforation or profound bleeding requiring repeated surgery.
Conclusions and Relevance:
Endoscopic septoplasty and TNTS show similar results for treatment of nasal septum deviation.
Introduction
Nasal obstruction is one of the most common complaints that otorhinolaryngologists face in their daily practice. Deviated nasal septum (DNS) is a frequently encountered cause of such obstruction. In addition to causing breathing difficulties, DNS results in improper aeration of paranasal sinuses, predisposing to sinusitis, and results in drying of mucosa, leading to crusting and epistaxis.1,2 Deviated nasal septum is sometimes accompanied by hypertrophic nasal turbinates, thus causing sleep disturbances and snoring. 3
Nasal septoplasty is a common surgical intervention, directed to improve nasal breathing 4 and sleep disturbances. 3 The traditional trans-nasal trans-speculum (TNTS) septoplasty involves submucosal resection of the nasal septum; the complication rate is 3%-30%.There is no consensus on the long-term relief of symptoms after this procedure.5,6
Endoscopic septoplasty is a minimally invasive technique that was developed as an alternative to the traditional submucosal resection for correction of DNS. In the last 2 decades, endoscopic sinonasal surgery has been widely used for indications of inflammatory and neoplastic diseases. The excellent visualization of this approach is presumed to decrease morbidity and postoperative swelling, by limiting the excision to the area of deviation in the involved area. 2 Furthermore, diagnosing and treating abnormalities of the nose during the same procedure, including concha bullosa and polyps, are often only possible in the endoscopic approach. Nevertheless, no randomized studies have evaluated the utility of the endoscopic and TNTS techniques for DNS. In this randomized study, we evaluated the results, complications and quality of life (QOL) in patients undergoing traditional TNTS septoplasty compared to endoscopic septoplasty.
Patients and Methods
This prospective, randomized controlled trial was conducted after its protocol was approved by the review board of our institution (0576-15-RMB). The study took place at the Otolaryngology Head and Neck Surgery Department, the Head and Neck Center, at Rambam Medical Center, Haifa, Israel. Patients who underwent primary surgery for repairing DNS due to nasal obstruction, were older than 18 years old, and were eligible for study inclusion. Exclusion criteria included bilateral acute or chronic rhinosinusitis, nasal polyposis, concha bullosa, inflammatory disease (eg, Wegener granulomatosis, sarcoidosis), neoplastic nasal pathology, diagnosis of systemic conditions affecting the nose (eg, cystic fibrosis, Kartagener syndrome), and an intention to undergo revision surgery.
Between March 2016 and November 2017, patients scheduled for primary surgery for DNS were enrolled in the study after providing informed consent to participate. The random allocation sequence (1:1) was generated using a computer-generated list. The 2 arms consisted of: a control arm of patients undergoing TNTS septoplasty for DNS; and an experimental arm, which included patients undergoing endoscopic septoplasty. All surgeries were performed by the same surgeon.
Surgical Technique
The TNTS septoplasty was performed using a headlight, loups, and a speculum. After injection, a Killian incision was made using a No. 15 blade. The incision was performed on the side of the deviation. Then the submucosal flaps were elevated and the deviated segment was removed with an adequate strut left intact to prevent columellar collapse. Cartilage was replaced and nasal packing (Medtronic’s Xomed, Jacksonville, Florida) was used. If indicated, inferior turbinate reduction was also performed. The endoscopic septoplasty was performed using a similar technique, but under visualization with a 4-mm, 0° rigid endoscope (Stor, Tuttlingen, Germany). The endoscope was used to identify the deviated segment of the septum and for visualization during dissection under the flap. If indicated, inferior turbinate reduction was also performed.
Outcome Measures
All patients were followed with fiber optic endoscopes during the first 3 months after surgery. The primary outcome was the change in the Sino-Nasal Outcome Test-22 (SNOT-22) scores. 7 Sino-Nasal Outcome Test-22 was previously shown to evaluate symptomatic relief following septoplasty. 8 The score on the Short Form 36 (SF36) QOL questionnaire9,10 was a secondary outcome. Short Form 36 is a short questionnaire consisting of 36 questions regarding patients’ global health, and physical, social, and psychological domains.
Postoperative complications (eg, epistaxis, perforation of the septum, and formation of synechiae) were evaluated in the follow-up visits. All outcome measures were evaluated at baseline (maximum 3 months before surgery), at 2 weeks, and at 3 months after the surgery. Figure 1 shows the flowchart of the study design.
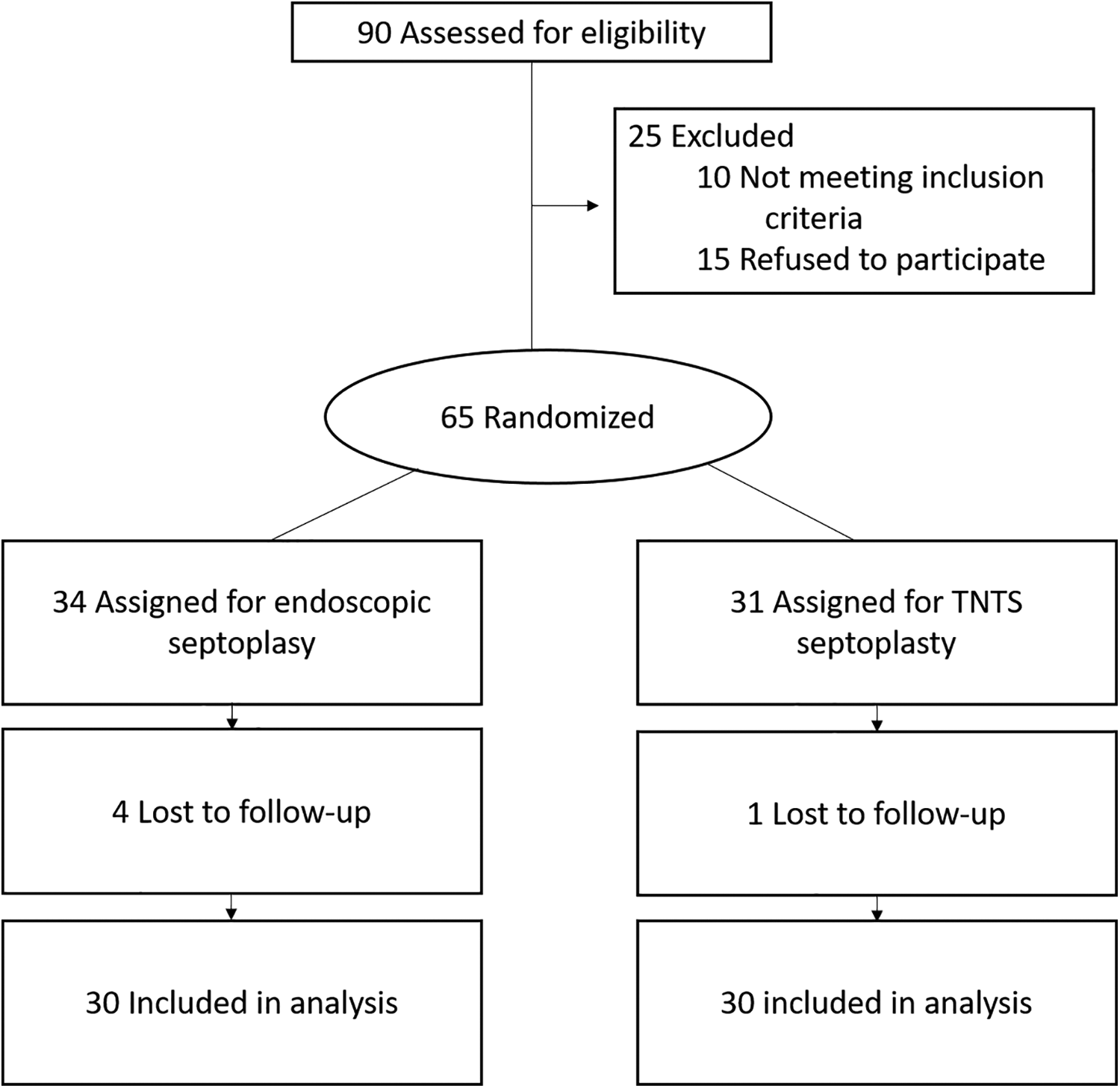
CONSORT flow chart of the study. TNTS indicates trans-nasal trans-speculum.
Statistical Analysis
An a priori sample size calculation was performed. Using SNOT-22 scores as the primary outcome, as per the above, with an α of .05 and β of .8, 22 patients per arm are required to demonstrate a 20-point difference between the arms, which would be deemed clinically significant. This determined a study population of at least 44 patients in total. Descriptive statistics were presented as means with standard deviations. Analysis of variance and χ2 testing were used as appropriate for data analysis, and all tests were 2-tailed, with a α = .05 set as the level of significance. All analyses were done using JMP10 software for windows (SAS, Inc, Chicago, Illinois).
Results
Sixty-five patients were enrolled in this study, 34 in the endoscopic arm and 31 in the TNTS septoplasty arm. The overall follow-up rate was 94% at the first visit (2 weeks) and 92% at the last visit (12 weeks). Four in the endoscopic arm dropped out, and 1 in the TNTS arm. Thus, the final cohort consisted of 60 patients, 30 in each study arm.
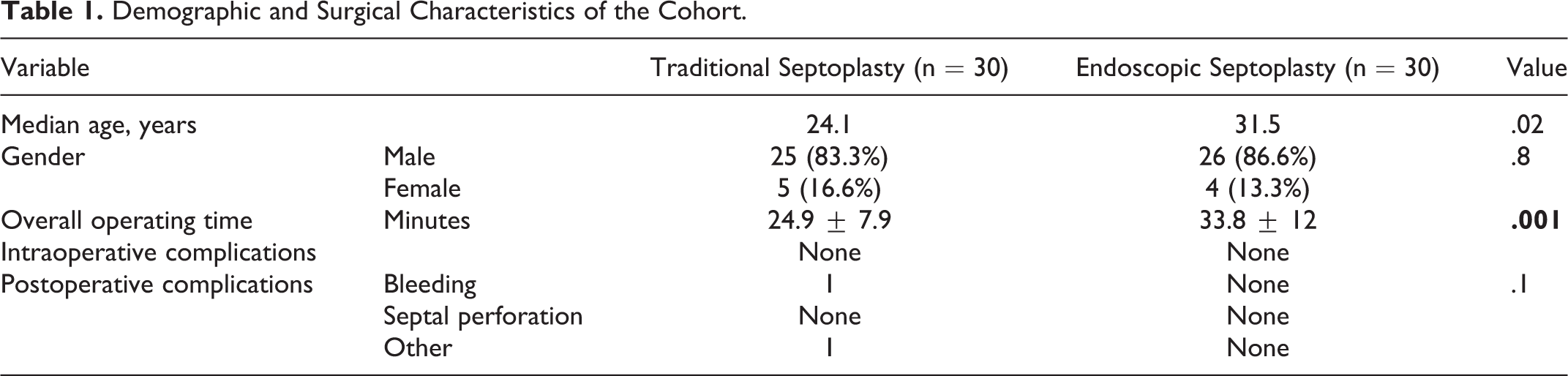
The patients ranged in age from 18 to 71 years (mean 27 years) old. Table 1 shows that the mean total operative time was 24.9 ± 7.9 minutes in the traditional septoplasty arm compared to 33.8 ± 12 minutes in the endoscopic septoplasty arm (P = .001). There were no complications in the endoscopic septoplasty arm, whereas in the TNTS arm, complications included epistaxis requiring cauterization and a surgical site granuloma that was removed in the clinic (P = .1). There were no cases of septal perforation in either of the arms.
Demographic and Surgical Characteristics of the Cohort.
We compared the SNOT-22 scores between the 2 study arms at 3 time points. Prior to surgery, patients in both arms had similar scores (mean 43.8 in the TNTS arm and 46.2 in the endoscopic arm, P = .64). Figure 2 shows that the SNOT-22 scores improved in both arms at 2 weeks postoperatively (mean 30.8 in the TNTS arm and 41.4 in the endoscopic arm). Improvement in nasal symptoms was unremarkable in both arms (Figure 3A). However, in the TNTS arm, the scores were better than in the endoscopic arm regarding the following questions: less waking up at night (28.1% compared to 8.5%), productivity (20.0% compared to 9.5%), and less embarrassment (22.9% compared to 3.8%). Overall, the scores in the TNTS were significantly better than in the endoscopic arm at 2 weeks (P = .03).
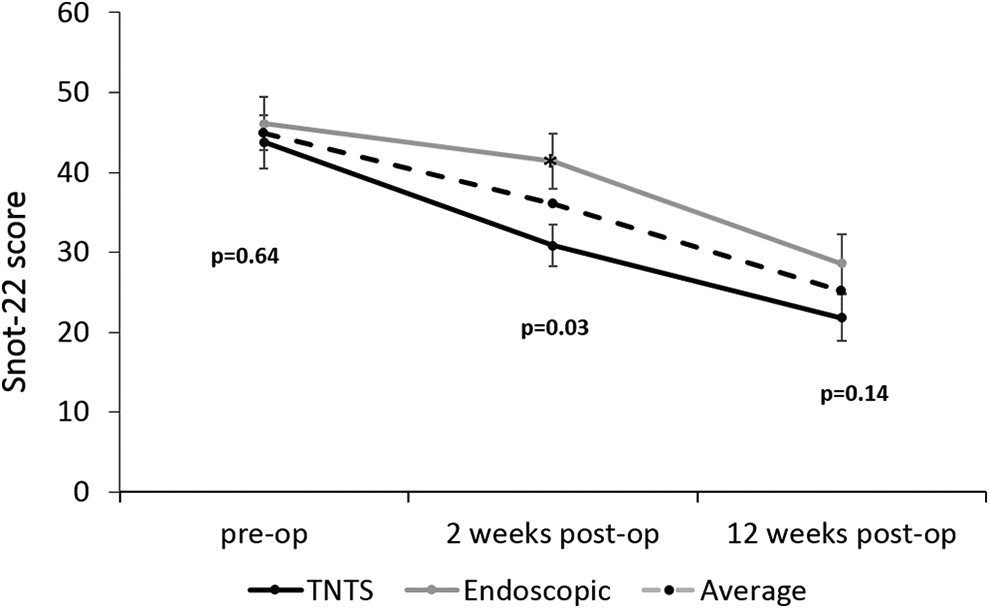
Sino-Nasal Outcome Test-22 score. Analysis of the total SNOT-22 questionnaire scores for both study arms. SNOT-22 indicates Sino-Nasal Outcome Test-22; TNTS, trans-nasal trans-speculum.
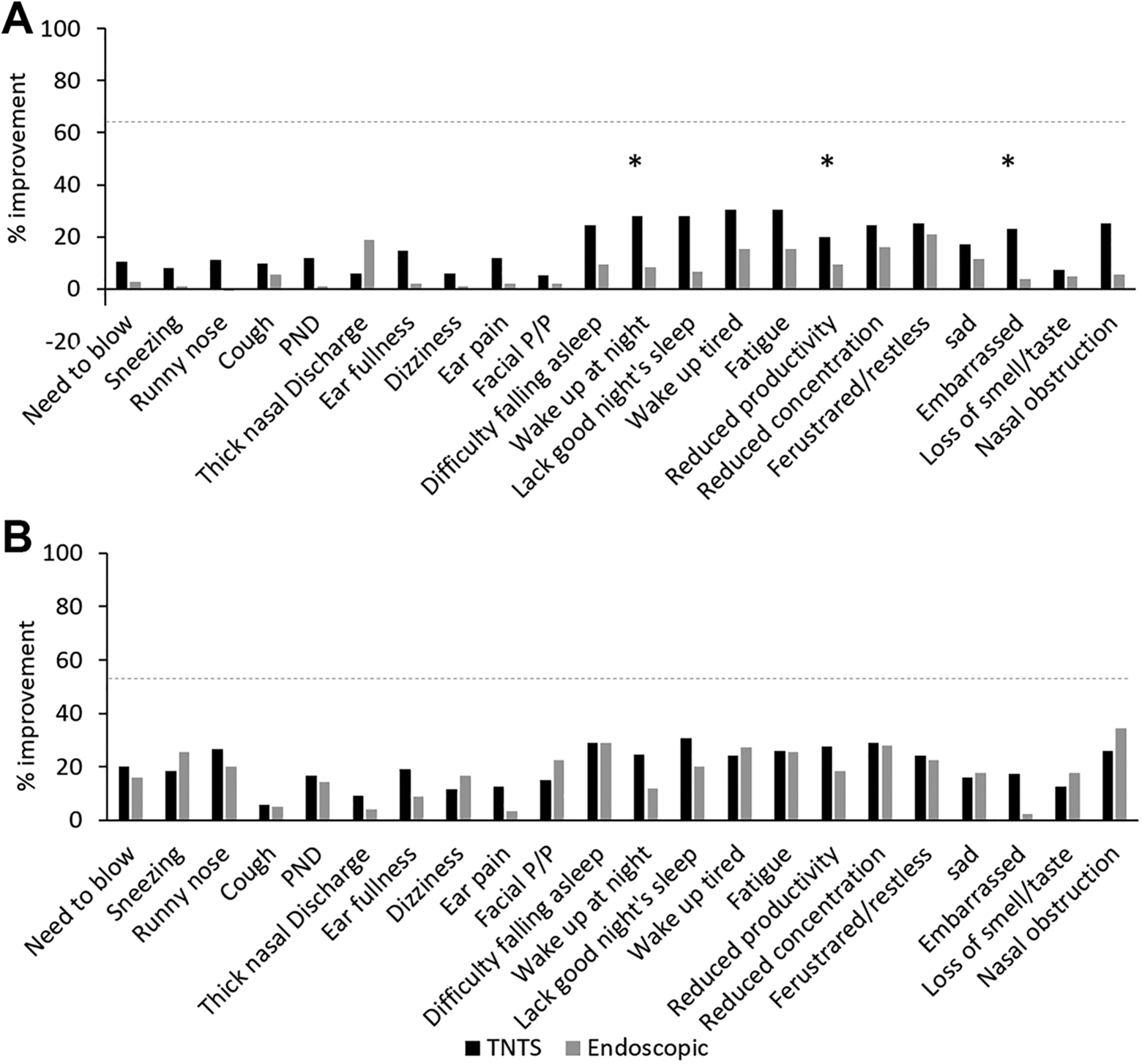
Univariate analysis of postoperative SNOT-22 scores. A, Two weeks postoperative; (B) 3 months postoperative. SNOT-22 indicates Sino-Nasal Outcome Test-22; TNTS, trans-nasal trans-speculum.
The SNOT-22 scores continued to improve following the surgery, and there was no difference between the arms at 3 months postoperatively (mean 21.8 in the TNTS arm and 28.6 in the endoscopic arm, P = .1). At this point in time, scores were similar for all parameters in both arms (Figure 3B). Looking specifically into the domain of nasal symptoms, SNOT-22 analysis results show that the most significant improvement was in nasal obstruction, runny nose, and sneezing (25.8%, 26.6%, and 18.3% in the TNTS arm, and 34.4%, 20.0%, and 25.6% in the endoscopic arm, respectively).
We evaluated changes in QOL, using the SF36 questionnaire. Overall, the total score (from 1-100) improved significantly in the 3 months after surgery (from mean 65.8-81.4, P < .001) for the entire cohort (Figure 4). Prior to the surgery, the scores were similar in the TNTS and the endoscopic arms: mean 66.8 and 64.8, respectively, P = .69. Two weeks following the surgery, the total mean score improved in the TNTS septoplasty arm, from 66.8-69.6 (P = .4); while in the endoscopic septoplasty arm, worsening, with borderline statistical significance, was observed, from 64.9 to 58.3 (P = .07). However, 3 months postoperative, both arms showed significant improvement in the SF36 compared to the preoperative scores: mean 83.4 in the TNTS arm and 81.4 in the endoscopic arm (P = .26). Supplementary Figure 1 shows for each study arm, the changes in each domain of the SF36 questionnaire during the follow-up.
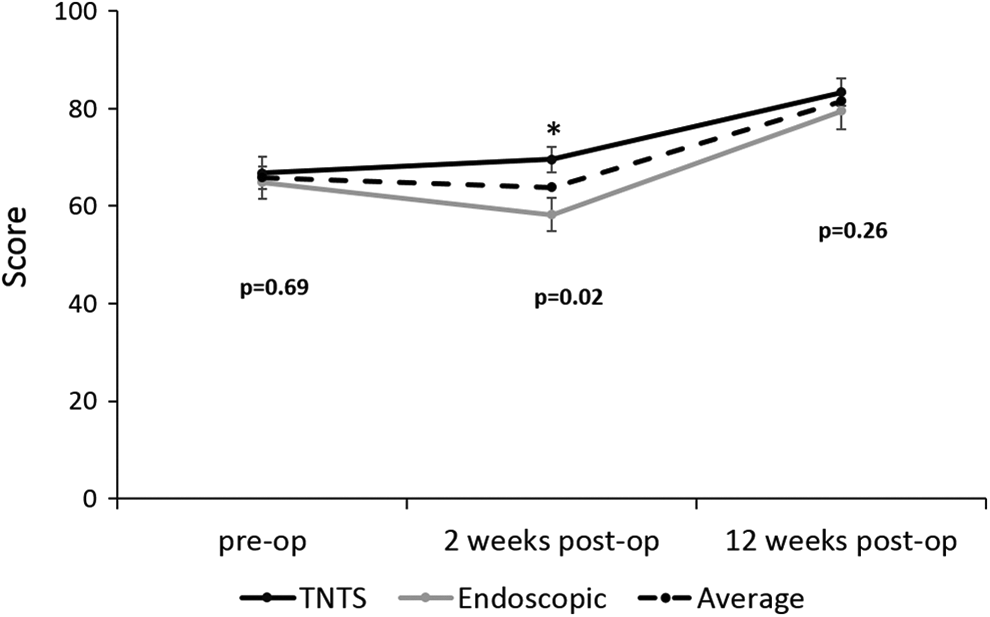
Short Form 36 score. Analysis of the total SF36 scores for both study arms. SF36, indicates Short Form 36; TNTS, trans-nasal trans-speculum.
Discussion
Submucosal resection is a common operation performed with the aim of improving nasal breathing, nasal symptoms, and sometimes snoring in patients with DNS. The traditional septoplasty procedure involves submucosal resection of the anterior septum. Not all patients experience improvement in their symptoms or in QOL after this operation. With the introduction of the endoscopic sino-nasal approach for septoplasty, this study aimed to compare the outcomes of the 2 approaches on nasal symptoms and quality of life.
The demographic and surgical parameters were similar between the arms except that the mean age was lower in the traditional septoplasty arm. Two weeks postoperatively, patients who underwent traditional septoplasty reported better QOL scores than patients who underwent endoscopic septoplasty. The QOL of all the patients was improved at 3 months following the operation, as evaluated by the SNOT-22 and SF36 questionnaires. After 3 months, the results of surgery were similar in the 2 arms.
Trans-nasal trans-speculum septoplasty is considered the traditional approach for submucosal resection and has been utilized for decades by the majority of ENT surgeons. However, long-term assessments of this surgery are contradictory, with most publications rating it as unsatisfactory. Studies that evaluated success rates according to various definitions of success, reported rates of 27% to 84%, 6 months to 11 years after surgery.11-16 Some used functional measures,11-14 while others used subjective questionnaires and assessed the QOL of the patients after the surgery.15,16 The complication rate of TNTS septoplasty varies between 3% and 30%, with contradictory reports on the long-term relief of symptoms after this procedure.5,6
Endoscopic septoplasty is a recently developed technique that has gained popularity in the last decade. The effectiveness of this approach was evaluated using objective functional tests, anatomical results, and complication rates.1,2 However, no published study prospectively evaluated changes in QOL following this procedure.
When comparing both approaches, the endoscopic approach accounted for a longer operating time with results that were similar to TNTS (with the same complications rate and similar QOL scores). Due to the enhanced depth of vision it allows, endoscopic septoplasty may be advantageous for correction of a posterior vomer deviation, concha bullosa, or choanal obstruction (adenoid enlargement or tail of the inferior turbinate). Where there is a localized septal deviation, the endoscopic approach may help to guide the incision and orient the correction to a more limited area of the septum. Any final decision should be based on surgeon preference and familiarity with each approach.
In conclusion, this study showed that septoplasty, both by TNTS and endoscopy, is effective in improving the symptoms and general QOL of patients with DNS.
Supplemental Material
supp_fig_1 - Endoscopic Septoplasty Versus Traditional Septoplasty for Treating Deviated Nasal Septum: A Prospective, Randomized Controlled Trial
supp_fig_1 for Endoscopic Septoplasty Versus Traditional Septoplasty for Treating Deviated Nasal Septum: A Prospective, Randomized Controlled Trial by Shorook Na’ara, Boris Kaptzan, Ziv Gil and Dimitry Ostrovsky in Ear, Nose & Throat Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.