
Abstract

Osteochondroma is a benign, cartilage-capped outgrowth of medullary and cortical bone. It represents 20% to 50% of all benign bone tumors, and may be developmental or associated with trauma or irradiation. 1 The tumor arises from a trapped cartilage and grows at right angles to normal growth plate via endochondral ossification. Most lesions have a limited growth potential that ceases with skeletal maturity. Osteochondroma may be solitary or may occur in multiple form associated with the syndrome hereditary multiple exostoses, which also comprises short stature, knee and ankle valgus deformities, and forearm abnormalities. 1
Within the craniofacial bones, osteochondromas have been reported most frequently in the mandibular condyle and coronoid process. Jaw lesions tend to occur at a later age than do their counterparts in long bones. 2 Patients with condylar osteochondroma may have preauricular swelling, limitation of jaw movement, changes in dental occlusion, and deviation of the mandible to the contralateral side (Figure 1). 3 Osteochondroma of the coronoid process may impinge on the posterior surface of the zygoma, restricting mandibular opening. 4
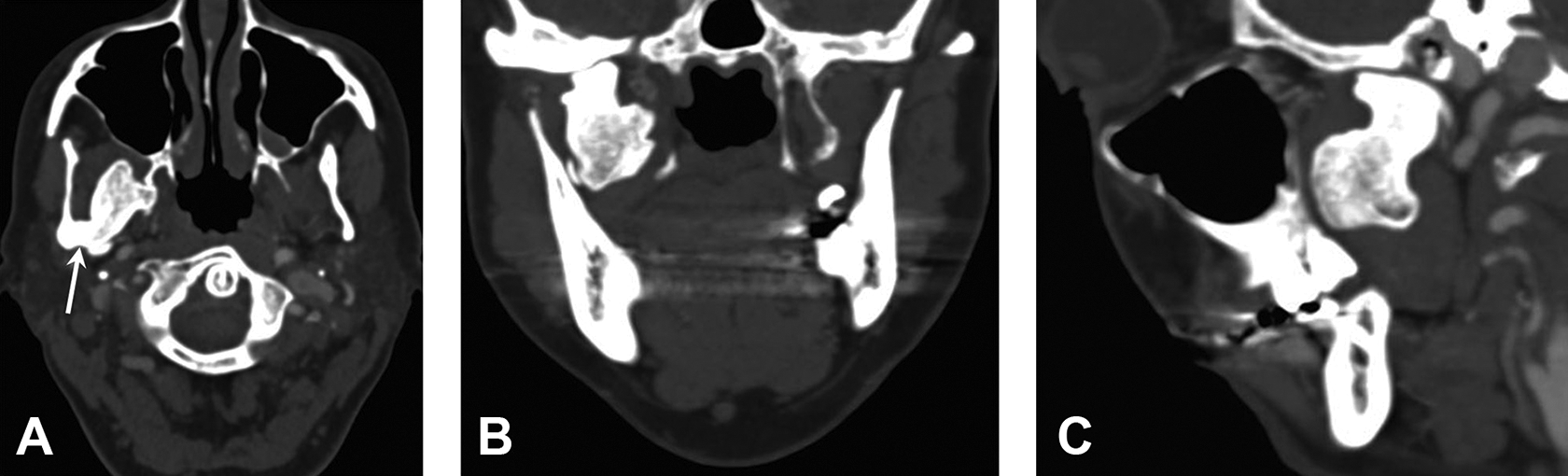
Osteochondroma of the mandibular condyle in a 53-year-old woman with a long history of limited jaw opening. A-C, Contrast-enhanced computed tomographic images show a circumscribed lobulated sclerotic mass arising from the anteromedial aspect of the right mandibular condyle and extending along the lateral pterygoid muscle into the infratemporal fossa. A, Axial view shows the narrow stalk and cortical continuity (arrow) to the underlying condyle, pathognomonic of an osteochondroma.
Radiographically, the tumor presents as an irregular, often pedunculated radiopaque mass attached to the bone surface. The most useful radiographic characteristic to distinguish osteochondroma from osteoma is the corticomedullary continuity; the cortical and medullary structure of the osteochondroma is continuous with the underlying native bone (Figure 1). Computed tomographic imaging is the modality of choice to demonstrate the characteristic appearance of marrow and cortical continuity. 1 The hyaline cartilage cap is not visible on plain images. Occasionally, the chondroid tissue is suggested by the identification of stippled calcifications. 1 The nonmineralized cartilage cap has high signal intensity on T2-weighted or proton-density magnetic resonance (MR) images, reflecting its high water content. The tumor has a nonhomogeneous low to intermediate signal intensity on all MR imaging sequences, with peripheral enhancement on gadolinium-enhanced T1-weighted images. 5 Bone scintigraphy of osteochondromas shows markedly increased uptake; however, this is a nonspecific finding that represents any underlying bone condition with increased osteoblastic activity.
Parosteal osteosarcoma and myositis ossificans are common mimics of osteochondroma. The ossification pattern of parosteal osteosarcoma is the radiographic inverse of that seen in osteochondroma, with gradual ossification of the lesion from the center toward the periphery. In contrast to osteochondroma, myositis ossificans lacks corticomedullary continuity between the lesion and underlying bone. 6 Occasionally, condylar hyperplasia may simulate a condylar osteochondroma, but the normal shape of the condyle in the former condition should be discriminatory.
Approximately 1% of solitary osteochondromas may undergo malignant transformation into chondrosarcoma. 1 Continued active growth and a cartilage cap greater than 2 cm in thickness, after skeletal maturation, should increase suspicion of malignant transformation. 7
Osteochondromas are treated with surgical excision. Recurrence has rarely been noted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.