
Abstract
Objectives:
The study aimed to investigate the epidemiological and clinical characteristics as well as the therapeutic results in patients with locoregional (LR) relapse after treatment of nasopharyngeal carcinoma (NPC).
Methods:
We retrospectively reviewed the medical records of patients with local and/or regional recurrent NPC over 13 years (2003-2015).
Results:
Twenty-five patients were treated for local or/and local–regional recurrence of NPC. The rate of LR relapse was 7.2%. The mean age of the patients was 46 ± 13.9 years. The median time to relapse was 25 months. The recurrence was nasopharyngeal in 17 patients, nasopharyngeal and neck lymph nodes in 7 patients, and neck lymph nodes in 1 patient. Fifteen relapsed patients had a locally advanced disease (rT3-rT4). Patients who had initially T1 or T2 tumor had a locally advanced relapsed disease (rT3rT4) in 27.3% and patients whose disease was initially classified as T3 or T4 had a locally advanced relapsed disease (rT3T4) in 85.7% (P = .005, Fisher test). Twelve patients had chemotherapy after relapse. Chemotherapy was followed by concurrent chemoradiotherapy in 3 patients and by radiotherapy (RT) in 4 patients. Nine patients had concurrent chemoradiotherapy and 1 patient had exclusive RT. The overall survival (OS) at 1 year, 3 years, and 5 years was, respectively, 58%, 18%, and 10%. The OS was significantly higher in patients with good performance status at the time of relapse (World Health Organization = 1; P = .01) and in patients with late relapse (after 2 years; P = .03).
Conclusions:
Locoregional relapse rate in our study was 7.2%. Locoregional reirradiation was the mainstay treatment modality in relapsed NPC. Relapsed NPC had a poor prognosis with a 5-year survival rate of 18%. The OS was significantly higher in patients with good performance status and in patients with late relapse (after 2 years).
Keywords
Introduction
Nasopharyngeal carcinoma (NPC) is common in Tunisia, which is one of the intermediate-risk areas for this cancer. 1 It is the second most common cancer of the head and neck after laryngeal cancer. 1 Locoregional (LR) control rate of NPC has improved significantly in the past decade due to the use of combination of chemotherapy and radiotherapy (RT) and to advances in RT techniques. 2 However, local recurrence can reach up to 20% of cases 3 and still represents a major cause of mortality and morbidity. The management of local failure remains a challenging issue in NPC. 4 The best treatment of LR failure remains controversial. 5 There are 2 therapeutic options: surgery and reirradiation, which can be associated with chemotherapy.
The study aimed to analyze the epidemiological and clinical characteristics as well as the therapeutic results in patients with LR relapse after the treatment of NPC.
Materials and Methods
We retrospectively reviewed the medical records of patients with local relapse and/or neck lymph nodes relapse of NPC over a period of 13 years (between January 2003 and December 2015).
After treatment completion, follow-up assessments were conducted every 3 months for the first 2 years, every 6 months from the third through the fifth year, and annually thereafter. Follow-up included medical history, physical examination, and nasopharyngoscopy. An enhanced magnetic resonance imaging (MRI) and/or computed tomography (CT) scan of the nasopharynx and neck areas were performed at 3 months and then every 6 to 12 months.
Recurrent disease was defined as the reappearance of nasopharyngeal tumor and/or neck lymph node 3 months after initial complete regression, while residual disease was defined as the nasopharyngeal tumor and/or lymph nodes without complete regression by 3 months after primary therapy. 6 Patients with persistent disease at 3 months after primary treatment were not included in our study.
Patients with pathologically confirmed locoregionally relapse of NPC were included. Patients with metastatic spread associated with LR relapse were not included. The tumor was classified according to the seventh edition of the TNM classification by the Union for International Cancer Control.
The therapeutic decision was made in a multidisciplinary consultation involving the medical oncologist, the radiation oncologist, the pathologist, and the head and neck surgeon. Multidisciplinary consultation allowed us to choose and adapt treatments for each patient according to clinical (especially the performance status and the age), biological features (creatinine level), previous treatment (neck RT), and the stage of the disease.
The overall survival (OS) was assessed from the date of diagnosis of the relapse to the date of the latest news or death regardless of the cause.
All variables including baseline characteristics were presented as a number with a percentage for categorical variables, mean ± standard deviation for continuous variables following a normal distribution, and median with extremes for continuous variables not following a normal distribution.
The OS was estimated according to Kaplan-Meier method. The χ2 test and Fisher exact test were used to compare the distribution of categorical variable. The stratified log-rank test was used to evaluate the single factor prognosis. Patients’ survival was compared according to gender, age (median), performance status, the time to relapse, the T and the N classification at the relapse, and the use of brachytherapy added to RT. P values <.05 were considered to indicate statistical significance. Statistical analysis used the Statistical Package for Social Sciences (SPSS) for Windows (SPSS Inc, Chicago, Illinois) software version 20.
Results
Population Characteristics
Twenty-five patients were treated for LR relapse of NPC. In the same 13-year period, 348 patients were treated for nonmetastatic NPC, so that the rate of relapse was 7.2%.
The mean age of the patients was 46 ± 13.9 years. Two patients were 19 and 20 years old. There was a male predominance (sex ratio = 4).
Characteristics and Initial Treatment of the Primary Tumor Before Relapse
Eleven (44%) patients had tumors classified as T4 and 17 (68%) patients had tumors classified as N2 to N3. Thirteen (52%) patients had an induction chemotherapy. The induction chemotherapy protocol was docetaxel–cisplatin and 5-fluorouracil (TPF) in 4 patients, 5 fluorouracil and cisplatin in 6 patients, and epirubicin-cisplatin in 3 patients.
Seventeen patients received concurrent chemoradiation. This was weekly cisplatin in 13 patients (1-7 cycles) and 5 fluorouracil–cisplatin in 4 patients (2 cycles). It was associated with induction chemotherapy in 7 patients. Two patients received 50 Gy RT since they refused to continue treatment. Twenty-three patients received 70 Gy conventional RT. The characteristics of patients before the diagnosis of recurrence are detailed in Table 1.
Epidemiological, Clinical Features, and Initial Treatment.
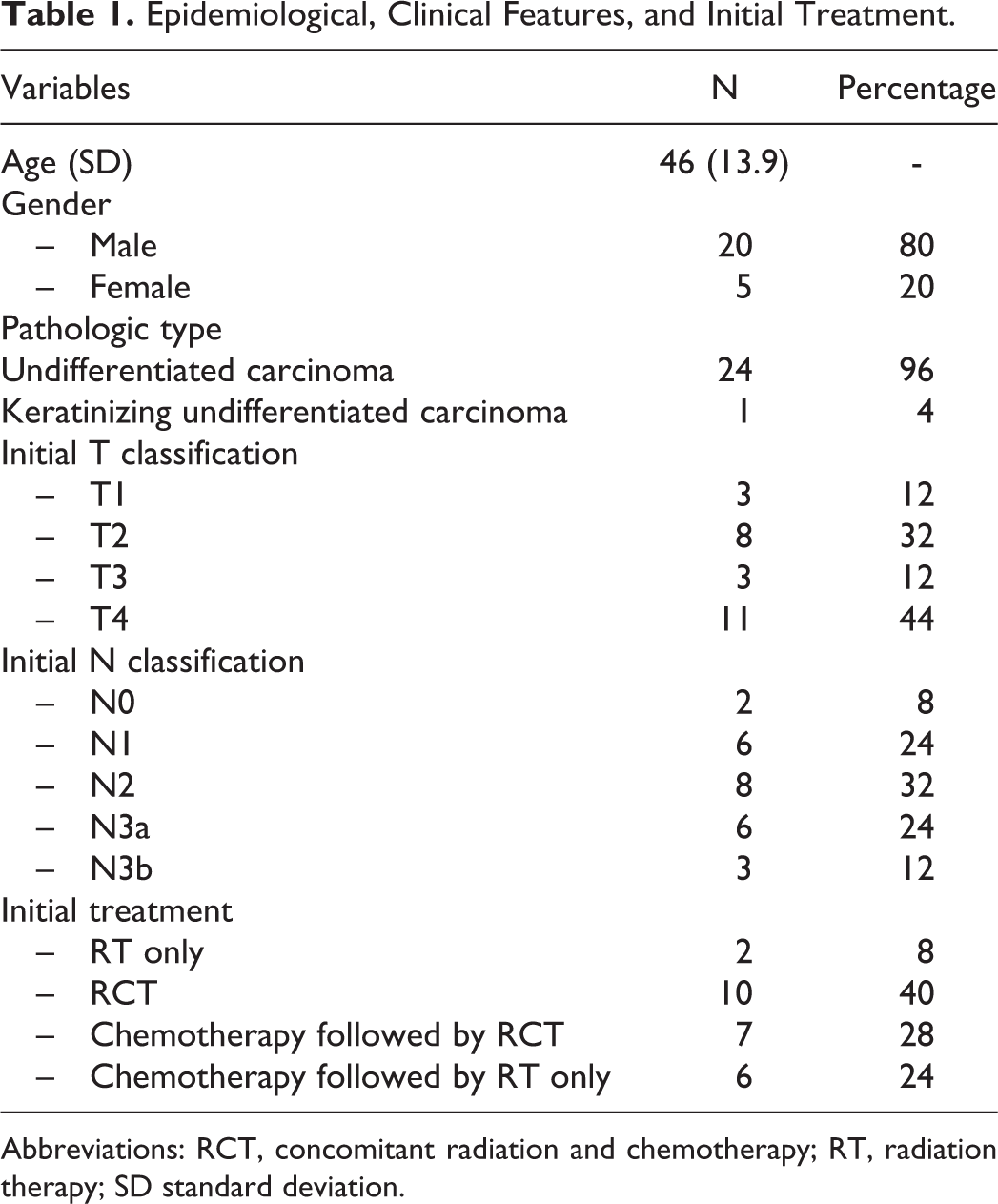
Abbreviations: RCT, concomitant radiation and chemotherapy; RT, radiation therapy; SD standard deviation.
Characteristics of Patients at the Relapse
Patients experienced local and/or regional recurrence after a median time of 25 months (3-109 months). At the moment of diagnosis of the LR relapse, 9 patients had rhinologic symptoms, 6 patients had neck lymph nodes, 3 patients had cranial nerve disorder, and 3 patients had a headache. Four patients had no symptoms. At the time of the relapse, 23 patients had a good performance status (World Health Organization = 1).
Relapse occurred in the nasopharynx in 17 patients. It was LR (nasopharyngeal and neck lymph nodes) in 7 patients and neck lymph nodes in 1 patient. Tumor relapse was classified as rT0 in 1 patient, rT1 in 6 patients, rT2 in 3 patients, rT3 in 1 patient, and rT4 in 14 patients. Neck lymph node relapse was rN1 in 5 patients, rN2 in 2 patients, and rN3b in 1 patient.
Patients who had initially T1 or T2 tumor had a locally advanced relapsed disease (rT3rT4) in 27.3% and patients whose disease was initially classified as T3 or T4 had a locally advanced relapsed disease (rT3rT4) in 85.7% (P = .005, Fisher test). None of the patients initially classified N0 had a lymph node relapse.
Treatment
Three patients died before starting treatment. Nine patients had concurrent chemoradiotherapy, 1 patient had exclusive RT, and 12 patients had chemotherapy. Chemotherapy regimens were TPF in 8 patients (2-3 cycles), 5-fluorouracil–cisplatin in 1 patient (3 cycles), cisplatin–epirubicin in 2 patients (1 and 3 cycles), and weekly methotrexate in 1 patient (4 cycles). Chemotherapy was followed by concurrent chemoradiotherapy in 3 patients and by RT in 4 patients.
Of the 8 patients who received TPF chemotherapy, 3 patients experienced severe toxicity. These were febrile neutropenia, grade 3 hematological toxicity, and renal toxicity. Twelve patients had concurrent radiochemotherapy for relapse.
Concurrent chemotherapy regimen was weekly cisplatin in 4 patients, weekly carboplatin in 3 patients, and 5 fluorouracil–cisplatin in 2 patients. The median number of concurrent chemotherapy cycles (carboplatin or cisplatin) was 5 (extremes: 1-5 cycles). Seventeen patients underwent RT at relapse.
Eight patients had nasopharyngeal reirradiation, 1 patient had neck lymph node irradiation, 2 patients had brachytherapy alone, and 6 patients had a combination of brachytherapy and external nasopharyngeal RT.
The median dose of RT at relapse was 60 Gy (24-70 Gy). The acute toxicity of RT was dry mouth in 16 patients and dysphagia in 7 patients. The different therapeutic modalities of the relapsed disease are shown in Table 2.
Treatment of the Locoregional Relapse, Disease Control, and Second-Line Treatment.
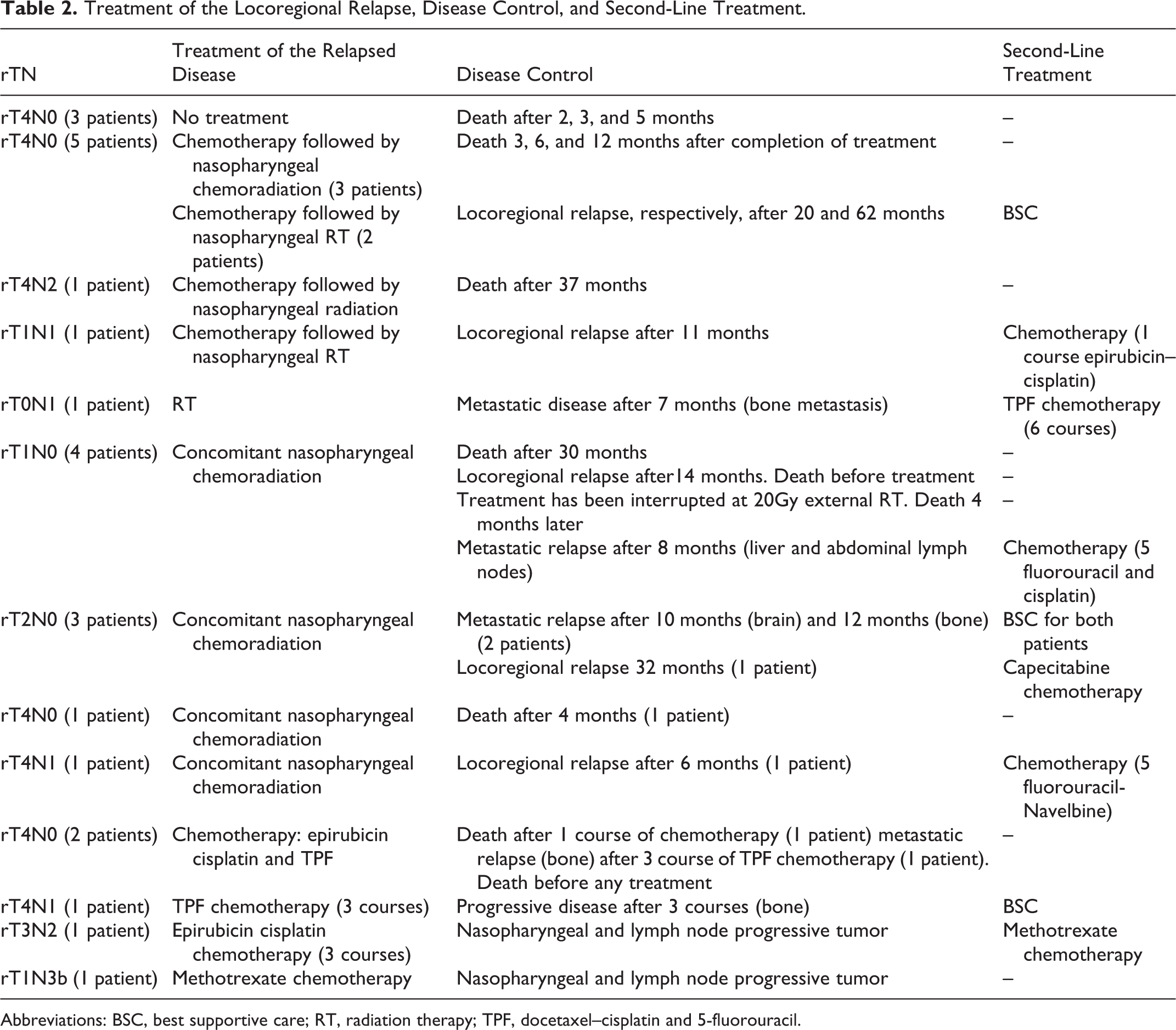
Abbreviations: BSC, best supportive care; RT, radiation therapy; TPF, docetaxel–cisplatin and 5-fluorouracil.
Prognostic Factors of Survival
The median follow-up was 14.5 months (1-78 months). The OS at 1 year, 3 years, and 5 years was, respectively, 58%, 18%, and 10% (Figure 1). Age, gender, T and N classification at the moment of relapse, and the use of brachytherapy did not affect statistically the OS (Table 3). The poor performance status and the time to relapse (<2 years) altered significantly the OS (Table 3).
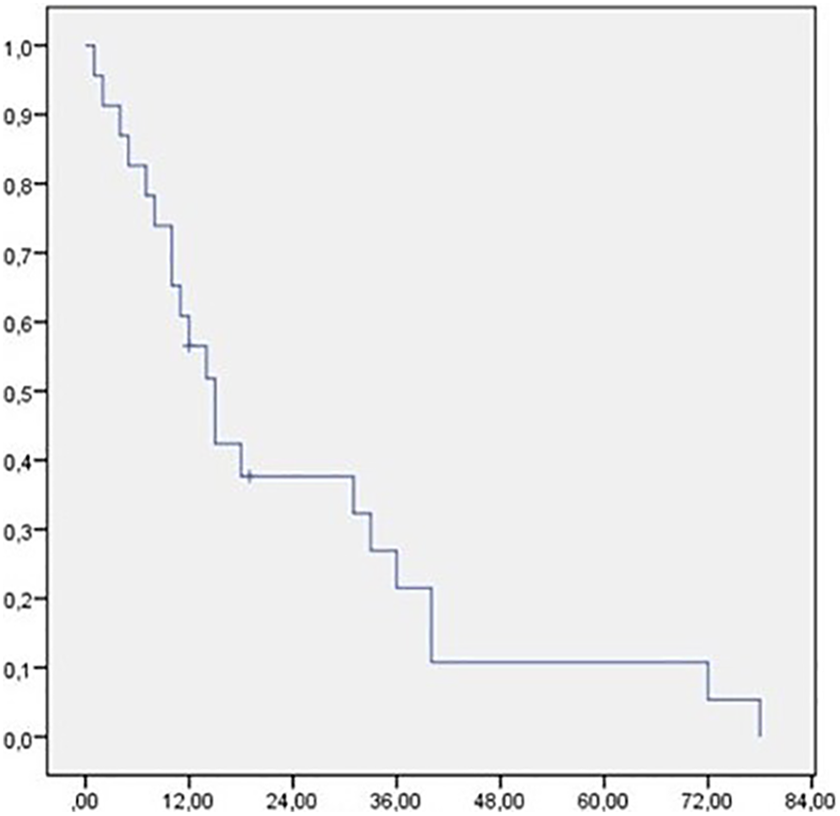
Overall survival after locoregional relapse.
Prognostic Factors in Locoregional Relapse of Nasopharyngeal Carcinoma.
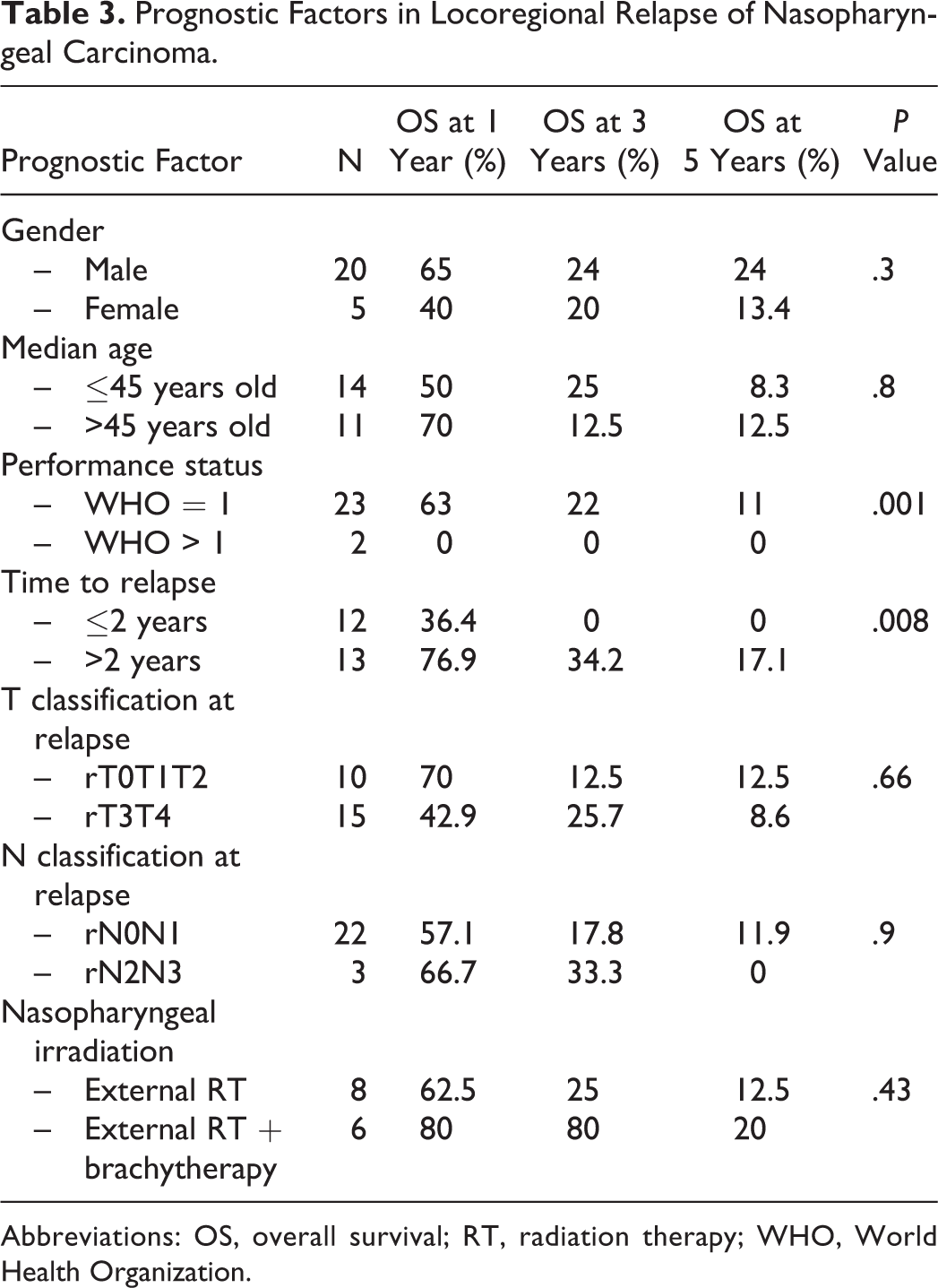
Abbreviations: OS, overall survival; RT, radiation therapy; WHO, World Health Organization.
Discussion
Despite advances in the treatment of NPC, LR relapse has been reported in 3% to 20% of cases. 7 -11 The relapse rate in our study was 7.2%.
In a retrospective study involving 447 patients with NPCs treated with RT, the mean time to relapse was 0.3 to 11.5 years (median: 1.4 years) for local relapses and 0.4 to 6.2 years (median: 1.3 years) for lymph node relapses. 7 The median time to relapse in our study was 25 months (3-109 months).
In a Chinese study of 337 patients with relapsed NPC, 12 patients suffered mainly from headache or epistaxis before the diagnosis of the relapse.
In our study, 56% of patients had a relapsed rT4 tumor and tumors initially classified as T3 or T4 relapsed as rT3 or rT4 tumors in 85.7% of cases. Wang et al 13 found in a retrospective study that T4 tumors were associated with a significant risk of LR relapse and that T stage was the only factor correlated with relapse.
The best management of LR failure remains controversial. 5 Surgery and reirradiation, which can be associated with chemotherapy, are the main therapeutic options.
According to the National Comprehensive Cancer Network recommendations, surgery is the first-line treatment for patients with LR when it is possible. 14 Indeed, the reirradiation of the nasopharynx could lead to significant toxicities on already irradiated tissue. Moreover, LR relapse could be characterized by clones of cells resistant to RT. In 4 retrospective studies of patients treated with nasopharyngectomy for recurrent NPC (31-60 patients), 15 -18 local control and 5 years OS ranged from 40% to 67% and from 30% to 52%, respectively. However, the nasopharyngectomy is usually mutilating. 19
In our study, due to the difficult exposure of the nasopharynx, and the high risk of functional deficits, no patients had nasopharyngectomy.
Through the literature series, there has been no direct comparison between surgical and nonsurgical treatment. 20 Reirradiation on relapsed tumors was the main therapeutic tool in our study.
For the localized stages rT1 and rT2, Leung et al 21 found in a retrospective study of 87 patients treated with external beam RT or brachytherapy during NPC relapse that brachytherapy significantly improves local control. Brachytherapy has the advantage of delivering an important dose within a limited volume, in a short time, while sparing the adjacent healthy tissues. It may be exclusive or may complement an external reirradiation. 22
Intensity-modulated radiotherapy (IMRT) resulted in a 60.9% local control survival at 5 years in a retrospective Chinese study about 245 patients who had rT3 or rT4 local relapse and treated with IMRT. 23
Intensity-modulated radiotherapy improved local control in relapses of NPCs in a study that included 150 patients treated with IMRT in previously irradiated patients with no gain in OS. 24
Unlike the treatment of the primary tumor, where the combination of RT and chemotherapy showed a benefit in terms of local control and survival, 23 the role of concurrent chemotherapy to RT in LR relapse was not well studied. The radiosensitization effect of concurrent cisplatin-like chemotherapy to RT on already irradiated tissue and previously treated with platinum would not be important. In phase II study, about 33 patients with locally advanced recurrent NPC, Ng et al 25 found that weekly docetaxel with cetuximab concurrent to RT improves outcomes in the treatment of locally advanced NPC relapses. The induction treatment with TPF used during LR relapse was associated with a lower response rate (4% complete response and 26% partial response) than the rate obtained with the induction of TPF in patients with de novo NPC (11% complete response and 80% partial response). 25
A retrospective study involving 24 patients with relapsed NPC showed that the 5 fluorouracil–cisplatin combination was associated with an objective response rate of 66%. 26
A phase III randomized study compared Gemcitabine plus cisplatin versus fluorouracil plus cisplatin in recurrent or metastatic NPC and found that gemcitabine–cisplatin prolonged significantly progression-free survival compared with 5 fluorouracil–cisplatin (7 months vs 5.6 months). 27
Xue et al found in a retrospective study of 54 patients with local or metastatic relapse of NPC that Sorafenib 5-fluorouracil and cisplatin followed by maintenance with Sorafenib were associated with a high response rate of 78%. 28
In a retrospective study, about 186 patients with relapsed NPC, the 1-, 3-, and 5-year survival was 54.9%, 22.1%, and 12.4%, respectively. 29 In our study, the OS at 1 year, 3 years, and 5 years was, respectively, 58%, 18%, and 10%.
Early relapse (<2 years) altered significantly the survival in our study. In fact, the most aggressive tumors are those that relapsed early. 30
In a study of 245 LR-relapsed patients, the 5-year OS was significantly poorer in patients with T4 disease compared to those with T3 disease (18.4% vs 36.9%; P < .01). 23 In a retrospective study, about 51 patients who had reirradiation for recurrent NPC after primary therapy with RT, the 5-year survival was 38% for patients with rT1–rT2 tumors and 15% for those patients with rT3–rT4. 31 These results emphasize the importance of early detection of local recurrence by nasopharyngeal endoscopy MRI and/or CT scan. In our study, the rT stage was not correlated with survival, which can be explained by the small size of our sample.
Tian et al 32 found that the association of local relapse with lymph node relapse led to worse survival (5 years OS: 31.7% vs 43%, P = .06).
The main limitation of our study was its retrospective design. Besides, no patient had surgical management in our study because of the difficult exposure of nasopharynx.
Conclusion
Locoregional relapses concern 7.2% of patients in our series, which is a rate comparable to the rates reported in the various series of the literature (3%-20%). The treatment is essentially based on LR-RT. Locoregional relapses of NPCs have a poor prognosis with a 5-year survival rate of 18%. The OS was significantly higher in patients with good performance status and in patients with late relapse (after 2 years).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.