
Abstract
Tapia syndrome is a rare complication after surgery, with ipsilateral paralysis of vocal cord and tongue due to extracranial involvement of recurrent laryngeal and hypoglossal nerves. Tapia’s case report is extremely interesting for both the rarity of the reported cases and for the importance of an early rehabilitation. In a previous work, we reported a case of Tapia syndrome after cardiac surgery for aortic aneurysm, and the protocol of logopedic rehabilitation adopted. In the postoperative period, he developed severe dyspnea and dysphagia that required a tracheostomy and a logopedic rehabilitation therapy that led to a fast and efficient swallowing without aspiration after 47 sessions (less than 4 months). The progressive recovery of the function suggests aprassic nerve damage. However, the logopedic therapy is recommended to limit the possibility of permanent functional deficits and quickly recover swallowing and phonation.
Ear, Nose and Throat Journal recently published a work by Deveci et al 1 concerning a patient with Tapia syndrome occurred after total thyroidectomy.
Tapia syndrome is a rare complication after surgery, with ipsilateral paralysis of vocal cord and tongue due to extracranial involvement of recurrent laryngeal and hypoglossal nerves.
The pathogenic hypotheses are the pressure-related neuropathy of XII cranial nerve during intubation and the compression of anterior branch of recurrent laryngeal nerve between the cuff of a dislocated endotracheal tube and posterior portion of the thyroid shield. 2,3 Tapia’s case report is extremely interesting for both the rarity of the reported cases and for the importance of an early rehabilitation.
In a previous work, 4 we reported a case of Tapia syndrome after cardiac surgery for aortic aneurysm.
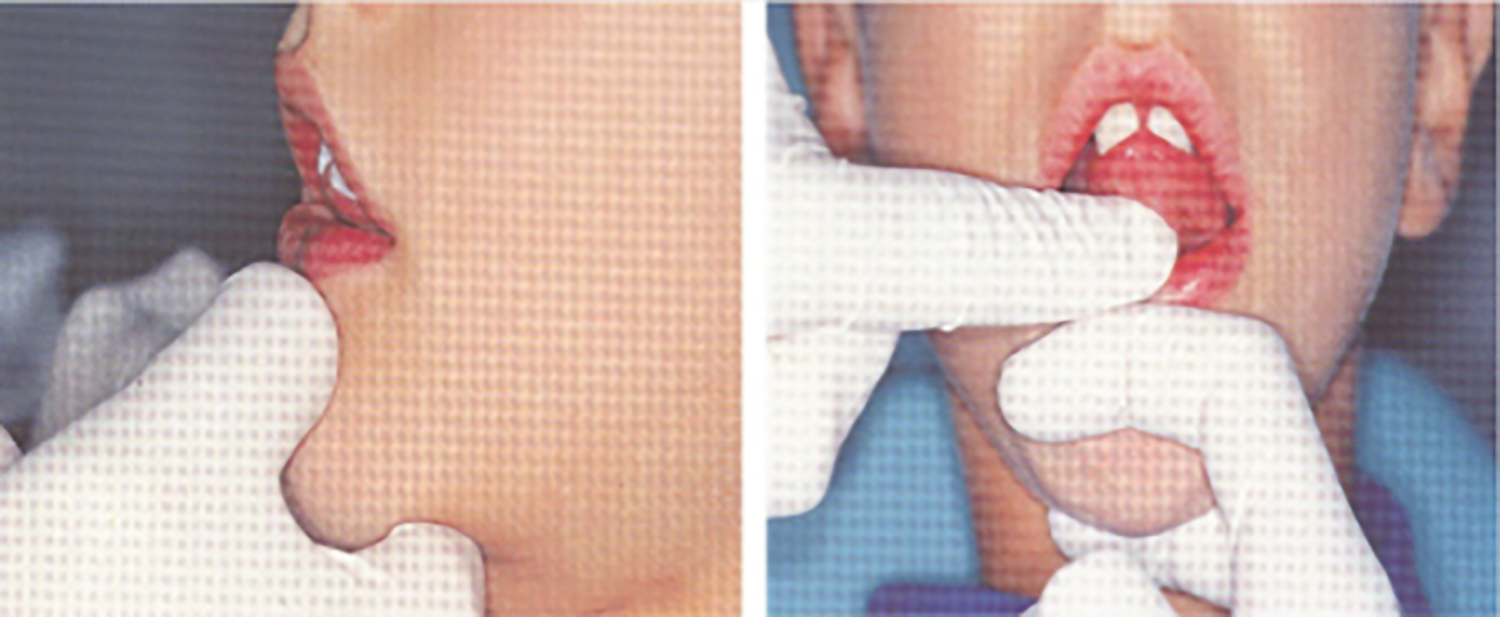
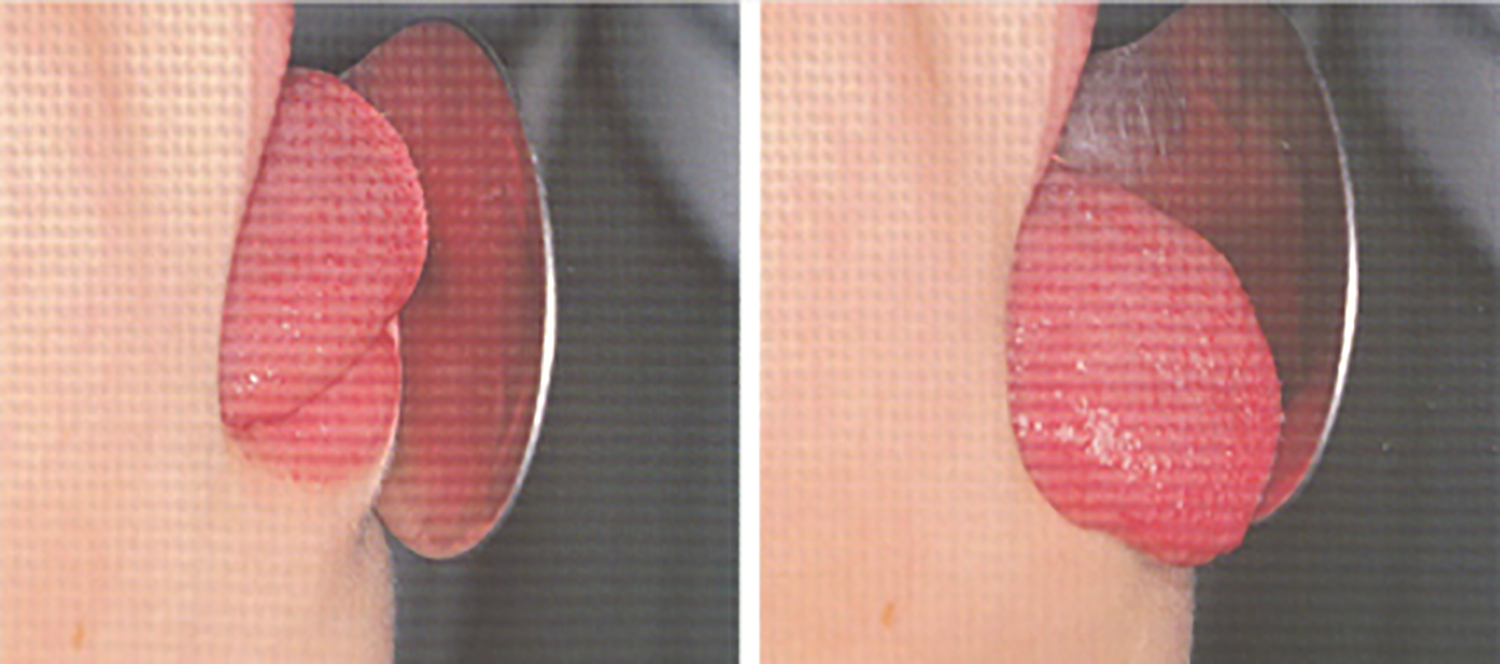
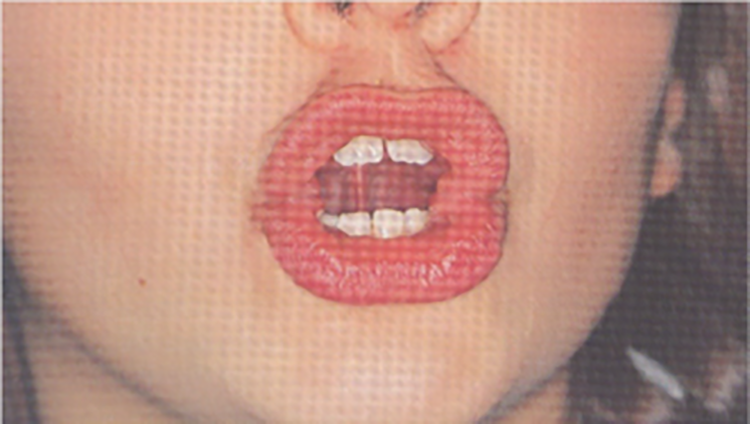
A month after the onset of the syndrome, we proposed this rehabilitation plan: Individualized logopedic treatment to: Improve speed and efficiency of swallowing; Remove suction through compensatory strategies; Improve the dysphagia through 2 different paths, compensation and rehabilitation, to ensure the patient to safely feed. The work plan acted on: General area: on being vigilant, as our patient was, and activation of metacognition to identify, discriminate, and recognize swallowing movements, at every stage; Sectorial area: on general relaxation, body awareness, and breathing control; Specific area: therapeutic measures on the structure involved in swallowing and bound to recovery of the tone, compensation of patient disability by facilitative posture, and dietary tricks. Proprioception exercises achieving neuromuscular response through stimulation of proprioceptors, free nerve endings, and receptors that govern tactile and thermal sensitivity of tongue: “Cooling” exercise (Figure 1): an ice cube wrapped in gauze at level of the retroincisive papilla on the 2 sides of the tongue, evoking tongue elevation toward the stimulated area. Exercise to retraces pharyngeal phase of swallowing (Figure 1): patient is asked to open his mouth, to bring the tip of his tongue in contact with the papilla, to raise the whole tongue toward palate and to flatten it against this, for 5 seconds, and then to remove the dorsum of tongue from the palate, while maintaining the tip in contact with it. Muscular gymnastic and functional recovery exercise “Packing” exercise for muscles of the mouth floor (Figure 2): the tip of the tongue rests on the palate, in contact with saltine winkles. Patient has to slightly open his mouth and press the tip of the tongue very strong against the palate, maintaining the same position. “Tongue depressor” exercise for the tip of tongue (Figure 3): patient is asked to push his tongue tip horizontally against a tongue depressor placed over his mouth; “Spoon” exercise for the tip of tongue (Figure 4): push and simultaneously move the tip of tongue against the concave surface of a spoon, circumferentially from right to left; “Gallop” exercise for the body tongue (Figure 5): the tongue, initially positioned with the tip in contact with palate, detaches from it, in a sweeping motion toward the mouth floor, imitating noise of a galloping horse. With the production of sounds A and O, the exercise also alternatively acts on labial commissures, thus enhancing buccinator muscles. “Yawning” exercise for tongue retrusion and for posterior portion of the tongue: patient has to yawn and feel the position that the tongue assumes; then, repeating the movement without yawning, the tongue must flatten and move back. Exercises of circling of lingual apex and displacing appropriate pseudo-boluses within oral cavity; in particular, we used whole olives asking to eat the fruit and eject the core. Exercises of phonoarticular rehabilitation: Slow and hyperarticulate repetition of letters produced by bringing the tip of the tongue on incisive papilla, that is, “L-T-N-D,” with vowel emissions before and after these letters; Addition of a wheezing prolonged “S” and repetition of words with these groups fast changing articulatory position, even for other groups like “LT-LD-ND”; Say, for as long as possible, the letter “R,” by vibrating the tip of the tongue against the anterior portion of palate; Use letters produced with the middle parts of tongue against the palate, that is, “C” and “G,” and by lifting the back of the tongue and vela-pharyngeal structures, that is, “K” and “G.” Up: “cooling” exercise (duration: 5 seconds, frequency: 10 times a day); down: exercise of the pharyngeal phase of swallowing (duration: 5 seconds, frequency: 20 times a day). “Packing” exercise (duration: 5 seconds, frequency 10 times a day). “Tongue depressor” exercise (duration: 5 seconds, frequency: 20 times a day). “Spoon” exercise (duration: 10 seconds, frequency: 20 times a day). “Gallop” exercise (duration: 2 seconds, frequency: 20 times a day for the first week, 40 times a day for the second week, and then 80 times a day for next weeks).


Treatment session were 47 in 4 months. At 19th session, patient began to drink semiliquids with a glass; at 23th session, tracheostomy tube was removed and he began to eat semisolids and, at 26th session, he began to eat solids. At 47th session, he showed mild difficulties only for liquids and increased tone of voice with reduced hoarseness.