
Abstract
Candidiasis is a rare entity reported as an isolated and primary laryngeal disease. In this condition, inhaled steroids were the single most common predisposing factor. Also mycotic infections of larynx are frequently seen in patients with immune insufficiency, although they have also been reported in individual with normal immune status. We report a case of isolated laryngeal Candidiasis in an immunocompetent individual, with an unusual presentation with exophytic lesion, edema, ulceration, white plaque, and pseudomembranous formation mimicking supraglottic carcinoma, to highlight the clinical of this condition and provide a review of the literature.
Introduction
Several opportunistic and/or pathogenic fungal species can cause acute or chronic laryngeal dysfunction. Candida albicans is the most frequent opportunistic organism colonizing the respiratory. 1 Laryngeal candidiasis is an uncommon form of laryngeal disease primarily seen in immune-compromised patients, but less frequently Candida can be the cause of laryngitis in immune-competent patients too.
Moreover, isolated laryngeal candidiasis in immune-competent individuals is infrequently recognized and poorly documented. Recently, a new type of laryngitis has been describing, the so-called “steroid inhaler laryngitis,” which has been reported in 10% to 15% of patients complaining of dysphonia during treatment with inhaled steroid therapy (IST). 2,3
Inhaled steroid therapy has become the standard of care for patients with obstructive lung disease. The topical complications of IST consist in oral candidiasis, throat pain, glossitis, and a mild laryngeal myopathy resulting in hoarseness. The reported incidence of candidiasis ranges from 0% to 91% and that of sore throat and dysphonia from 0% to 55%. 4
Here, we present a rare case with a serious complication of prolonged IST for asthma: primary laryngeal candidiasis in an immune-competent host mimicking a laryngeal carcinoma. With cessation of steroid inhalation and pharmacological antifungal therapy, the dysphonia, dysphagia, and laryngeal abnormality were rapidly resolved in 1 week.
Case Report
A 68-year-old immunocompetent male patient, a heavy smoker, was addressed to our Department for suspect laryngeal carcinoma. He referred fluctuating hoarseness for 4 months which had become more constant in the last month. He had smoked approximately 20 cigarettes a day for 40 years. He was asthmatic and affected by chronic obstructive pulmonary disease treated with inhaled fluticasone propionate (500 μg, twice in day) combined with salmeterol xinafoate (50 ng) via the use of a large volume spacer device for 1 year. He had been visited by Otolaryngologist who works in another Hospital for dysphonia with diagnosis of laryngeal carcinoma. So, he was referred to our ENT Department of University Federico II of Naples.
The laryngeal examination through rigid fiber-optic laryngoscope revealed whitish lesion/ulcerate lesion, suspicious for malignancy, involving epiglottis extended down to the arytenoids and aryepiglottic folds bilaterally and significant pooling of saliva (Figures 1 and 2). No fever, stridor, or dyspnea were noted. On physical examination, the oral cavity appeared normal and no neck lymphadenopathy was identified. All admission laboratory test results were within normal limits.
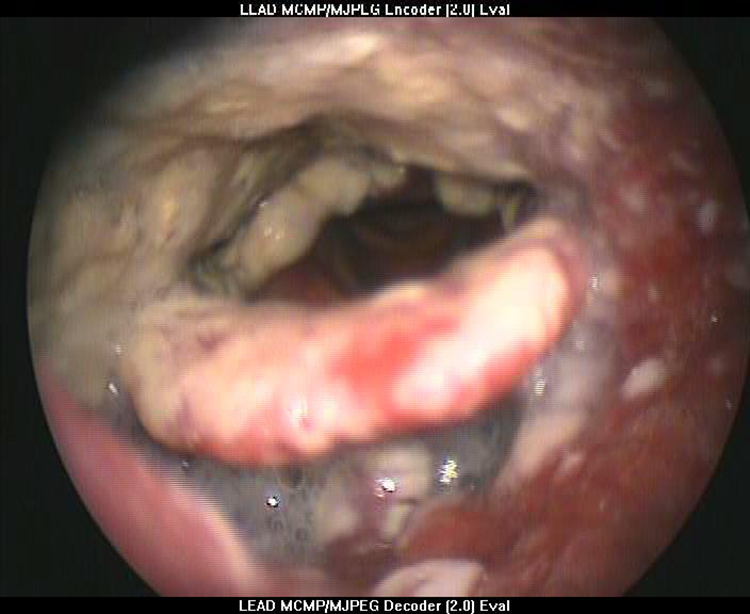
The laryngeal examination revealed whitish lesion/ulcerate lesion, suspicious for malignancy, involving epiglottis extended down to the arytenoids and aryepiglottic folds bilaterally.

Ulcerated lesion involving epiglottis.
Based on anamnesis and an endoscopic view with an uncleared picture, we made provisional diagnosis of fungal laryngitis and the patient was empirically started on antifungal therapy.
In particular, he was treated with oral fluconazole given at a dose of 100 mg daily which was continued for 15 days and inhaled corticosteroids were ceased. We had counseled the patient the need for further investigation if there was no resolution of symptoms. He remained on inhaled salbutamol as required, and her asthma symptoms were infrequent. He showed dramatic improvement within 7 days. Repeat laryngoscopy at 10 days, 20 days, 1 month, and 3 months demonstrated complete resolution of the lesion with normal voice and deglutition, and there has been no recurrence of the fungal infection (Figure 3).

Laryngoscopy demonstrated complete resolution of the lesion with normal voice and deglutition, and there has been no recurrence of fungal infection.
Discussion
Topical inhalers have been used in the treatment of asthma for more than 50 years. Recently, a combination product has been developed for the long-term control of asthma. It combines the use of a corticosteroid (fluticasone propionate) as an anti-inflammatory agent and a long-acting β 2 agonist (salmeterol xinafoate) as a bronchodilator. Its long-term use has been found to result in improved lung functions such as peak expiratory flow rates and forced expiratory volume in 1 second. 2
As the use of this combination therapy has become increasing popular, many patients who had been treated on concurrent 2-drug therapy or on systemic steroids and an inhaler have been switched to this form of inhaler. Some of the side effects noted from the use of the inhaler have been hoarseness (1%-5%, headache (2%-5%), throat irritation (1%-4%), and oral candidiasis (1%-4%). 2,5,6
The physical changes that are seen in the larynx of patients using inhaled fluticasone range from minimal to severe. Mild physical findings include edema and erythema. Moderate changes include mucosal thickening and vocal cord bowing. The most dramatic changes include leukoplakia, granulation, and laryngeal candidiasis. Physical findings may be minimal in patients with dysphonia caused using steroid inhalers, with only mild edema of the vocal cords. 3 The changes appear to be the result of a mucosal inflammatory reaction to the steroid. Treatment involves the use of oral antifungal agents. Reduction or cessation of IST should be undertaken if the condition does not clear up with antifungal therapy. The use of spacers to reduce the oral deposition of steroid appears to reduce the occurrence of oral candidiasis but not the degree of laryngopharyngeal symptoms and may increase the symptoms by delivering a larger amount of steroid to the larynx and pharynx. 3
Fungal laryngeal dysfunction is an uncommon form of laryngeal disease primarily seen in immunosuppressed host, such as patients with congenital or acquired immunodeficiency syndromes, with underlying hematologic or oncologic malignancies, with diabetes mellitus or nutritional deficiency, patients who have undergone successful organ transplantation and/or immune-suppressing therapy and/or practicing long-term oral steroid therapy or broad-spectrum antimicrobial therapy. 7
Otherwise, acute or chronic fungal laryngitis is considered only a rare manifestation in immune-competent patients. Moreover, when it occurs, it is often seen as a part of a bronchopulmonary fungal infections 8 and involvement of the larynx and other body sites outside the lung generally indicates a widely disseminated form of the disease. Isolated and primary occurrence as fungal laryngeal infection is uncommon with just few cases reported in literature. 9,10 For this reason, while it is easy suspecting fungal laryngitis in immunocompromised patients, it isn’t the same when there’s any evidence of alteration of immune status.
Clinical presentation of fungal laryngeal dysfunction can vary. Main symptoms usually consist in sore throat, hoarseness, and dysphagia, 11,12 but respiratory distress, fever, cough, and/or Gerd-like symptoms are reported too. 7,13
Video-laryngoscopic pictures of fungal laryngitis in immune-competent host are not always typical and can be confusing. Most cases show punctuated white patches adherent to mucosa, mucosal edema, erythema, 8,13 or white plaques with pseudomembranous lesion, 2 but in some cases exophytic lesions such as verrucous/papilliform mass 14,15 or ulcerous proliferative lesions 8 can resemble benign and malignant laryngeal lesions, for example, leukoplakia or carcinoma. So, the diagnosis of fungal laryngitis is often overlooked in immune-competent patients because it is commonly considered a disease of the immunocompromised, 16 and for this reason when the possibility of a malignancy is considered, biopsy of the lesion is soon carried out. A variable amount of submucosal edema may give the underlying tissue an irregular appearance the most typical location of laryngeal candidiasis is in the supraglottic larynx (especially epiglottis, arytenoid, plicae aryepiglottidis) where it may infrequently form large ulcerations although such lesions can be limited to the true vocal folds. The evidence of hyphae, philaments, or yeasts clarifies the diagnosis of a fungal infection. Ulcerative lesions are encountered in laryngeal disease, but although many ulcers have similar clinical appearances, their etiologies can vary from reactive to neoplastic. Although many studies have reported that fungal disease can cause oral ulcers, there have been few reports of oral ulcers associated with Candida, 17 while instead no manuscript of laryngeal ulcers associated with Candida secondary to steroid intake has been published before our documentation. The underlying mechanism of drug-induced ulceration is often unclear, and histopathological examination usually reveals nonspecific ulcer formation with marked infiltration as inflammatory cells. 18
Our patient complained of subacute onset of dysphonia and videolaryngoscopic images of larynx showed a picture resembling a supraglottic carcinoma characterized by the presence of dysphonia and dysphagia. The history of inhaled corticosteroid therapy let us to suspect mycotic laryngitis mimicking a malignant process.
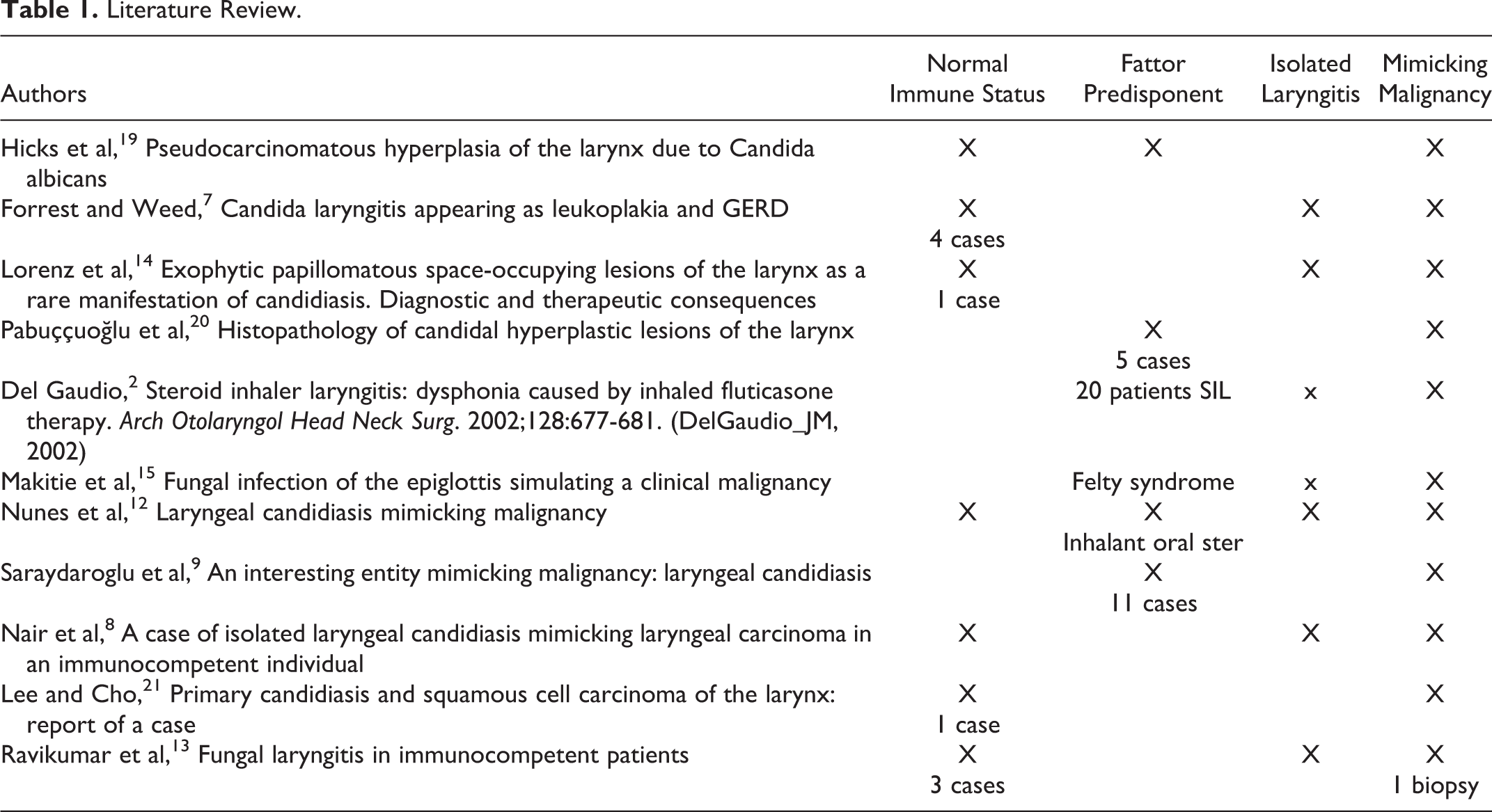
Several authors have documented mycotic laryngitis in patients with normal immune status. Many authors reported case of laryngitis caused by Candida species in immunocompetent host (Table 1). Only few of these authors reported isolated laryngitis mimicking malignancy too. 19,22 In particular:
Literature Review.
Forrest and Weed 7 showed a case of laryngeal candidiasis producing physical findings, such as erythema and leukoplakia, such as reflux laryngopharyngitis, treated without any improvement with aggressive antireflux therapy and then undergone to lesion biopsy, which revealed candida infection. Since this case, 3 other patients had presented with similar picture responding pharmacological therapy prior to any surgical intervention.
Nunes et al 12 illustrated a case of a stumpy, thickened and granular epiglottis with slight ulceration, extending down to the arytenoids, suspicious for carcinoma. Histological examination showed pseudohyphae and budding yeasts consistent with Candida;
Nair et al 8 reported a case of isolated laryngeal candidiasis in an immunocompetent Indian male mimicking laryngeal carcinoma to make provisional diagnosis of carcinoma supraglottic. Biopsy of the lesion was carried out to rule out malignancy, concluding for candidiasis;
Lee and Cho 21 revealed that chronic candida infection leads to epithelial hyperplasia and, possibly, to the development of epithelial atypia with observable malignant changes.
Pabuççuoğlu et al 20 showed histopathological features of a series of 5 patients with laryngeal candidiasis, observing that chronic candida infection of the larynx can produce exophytic lesions mimicking squamous cell carcinoma.
Recent evidences suggest that mycotic laryngitis can occur in immune-competent hosts in whom there are laryngeal mucosal barrier impairment. 7,13,16,23,24 Opportunistic organism, in fact, needs an impairment of host’s immune mechanisms and of the mucosal barrier to induce infection. Risk factors predisposing to local mucosal barrier damage can be identify in long-term IST, gastro-pharyngo-laryngeal reflux, previous radiotherapy, smoking, and trauma.
Saraydaroglu et al identified 7 cases of hyperplastic laryngeal candidiasis of immunocompetent patients, recognizing inhaled steroids therapy, and reflux the most common risk factors present, respectively, in 43% and 29% of them.
Mirza et al 3 evaluated the laryngeal findings in 9 users of combination of corticosteroid and broncho dilatator inhaler therapy: They reported the appearance of laryngeal vascular lesion and laryngeal areas of thickening, irregularity and leukoplakia, and dysphonia in all patients.
Wong et al 25 presented a series on laryngeal candidiasis counting 54 patients from 1995 to 2005, 48 (89%) of which were on steroid inhalers.
Del Gaudio 2 described physical changes seen in the larynx of patients using inhaled fluticasone, considering them as the result of a mucosal inflammatory reaction to the steroid.
The patient we expose started complaining of dysphonia after 1 year of treatment with inhaled steroids for chronic obstructive pulmonary disease. For these evidences, we made provisional diagnosis of fungal laryngitis and the patient was empirically started on antifungal therapy. We had counseled the patient the need for further investigation if there was no resolution of symptoms.
Therapy of fungal laryngitis consists in prolonged treatment by systemic antimycotics. According to literature, fluconazole given at a dose of 100 to 400 mg daily is the main choice. 5,12 It is the best option for patients with candida infections, as this oral agent has a higher rate of absorption. 7 Duration of treatment can vary from 10 to 30 days with noticeable clinical resolution of symptoms. An alternative is represented by itraconazole given at a dose of 100 mg twice a day for 4 weeks. 18
We started him on antifungal therapy with 100 mg of oral fluconazole daily which was continued for 15 days. He showed dramatic improvement within 7 days. Our case points out the possibility of a fungal laryngeal lesion in an immunocompetent individual and highlights the importance of considering it as a diagnosis prior to planning a biopsy to rule out malignancy.
We recommend that cessation of inhaled steroids be considered if clinically safe to do so, when patients develop hoarseness. Previous reports have outlined the importance of biopsy in making the diagnosis of laryngeal Candidiasis. We feel this is not necessary because treatment response can confirm the diagnosis. Furthermore, a biopsy might cause vocal fold scarring which can be extremely difficult to treat. Indications for biopsy for histopathology and fungal cultures include an incomplete response to adequate therapy or high suspicion of malignancy. However, the first step in the treatment is to eliminate the predisposing factors (in our cases inhaled corticosteroid therapy).
Conclusion
The increasing occurrence of primary fungal laryngeal dysfunction in immune-competent patients is an emerging trend in immune-competent patients. Laryngeal mycotic lesions may be confused with benign or malignant processes. A high index of suspicion is required to make the diagnosis, and fungal laryngitis should be considered in the differential diagnosis in any immune-competent patient with risk factors predisposing to local mucosal barrier impairment, especially long-term IST. In such cases, empirical antifungal therapy can clarify the diagnosis. The role of biopsy is justifiable if there is high suspicion of a malignancy, remaining an essential part of differential diagnosis when clinical improvements are not quickly gained through antifungal therapy. Anyway, a correct therapy must be started as soon as possible because long-term fungal infection might start malignant process. The diagnosis of Candidiasis should be considered in the differential in those patients with history of prolonged inhaled steroid use.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.